Masterclass in Orthopaedic Surgical Approaches: Foot and Ankle
Key Takeaway
Mastering surgical approaches to the foot and ankle requires a profound understanding of local anatomy, internervous planes, and biomechanics. This guide provides orthopaedic surgeons with evidence-based, step-by-step techniques for accessing the phalanges, calcaneus, and tarsus. Emphasizing soft-tissue preservation and optimal exposure, these protocols minimize complications while maximizing surgical efficacy for trauma, reconstruction, and arthroplasty procedures.
FUNDAMENTAL PRINCIPLES OF SURGICAL APPROACHES
In the evolution of operative orthopaedics, while many "new" surgical approaches have been described over the last several decades, few are truly original. The vast majority represent rediscovered historical exposures or nuanced modifications of established techniques. A master orthopaedic surgeon must possess an intimate understanding of cross-sectional and topographic anatomy to not only execute standard approaches but to dynamically adapt or design custom exposures when complex pathology dictates.
A meticulously planned surgical approach must provide unhindered access to all targeted osseous and soft-tissue structures. The incision must be of adequate length; a smaller incision that compromises visualization and makes the procedure exponentially more difficult can lead to catastrophic iatrogenic injury.
Soft Tissue and Incision Management
When practical, incisions should parallel or respect the natural resting skin tension lines (Langer’s lines) to optimize cosmesis and minimize hypertrophic scarring. For instance, a longitudinal incision crossing the flexor or extensor crease of a joint can precipitate a restrictive keloid, permanently impairing range of motion. Conversely, a longitudinal midlateral incision—particularly on the phalanges or the ulnar/fibular borders of the hand and foot—produces minimal scarring due to the relative immobility of the skin in these neutral axes.
🔪 Surgical Warning: Previous Scars
Unnecessary scarring and disfigurement must be avoided. Making a new longitudinal incision parallel to a previous scar is biologically unjustified and vascularly perilous. A second incision made parallel and adjacent to an old scar severely impairs the angiosome circulation in the intervening skin bridge, frequently culminating in full-thickness skin slough. Always utilize the prior incision, extending it as necessary, or maintain a minimum bridge of 7 cm if a parallel approach is unavoidable.
Hemostasis and Tourniquet Application
A pneumatic tourniquet should be universally employed in extremity surgery unless specifically contraindicated (e.g., severe peripheral vascular disease, sickle cell trait, or compromised soft-tissue envelopes). The exsanguinated, dry field facilitates precise dissection, minimizes traumatic tissue handling, and significantly reduces operative time. Furthermore, a bloodless field is critical for the reliable identification and preservation of delicate cutaneous nerves, which often serve as anatomical landmarks for deeper internervous planes.
Even with temporary ischemia, an electrocautery unit must be utilized to meticulously coagulate small vessels crossing the incision, preventing postoperative hematoma formation upon tourniquet deflation. In axial or proximal regions where a tourniquet is unfeasible (e.g., shoulder, hip, pelvis), electrocautery becomes the primary modality for maintaining visualization and minimizing blood loss.
SURGICAL APPROACHES TO THE TOES
Pathologies of the forefoot, including hallux valgus, rigidus, and lesser toe deformities (hammer, claw, and mallet toes), require precise surgical exposures that respect the delicate dorsal and plantar neurovascular bundles.
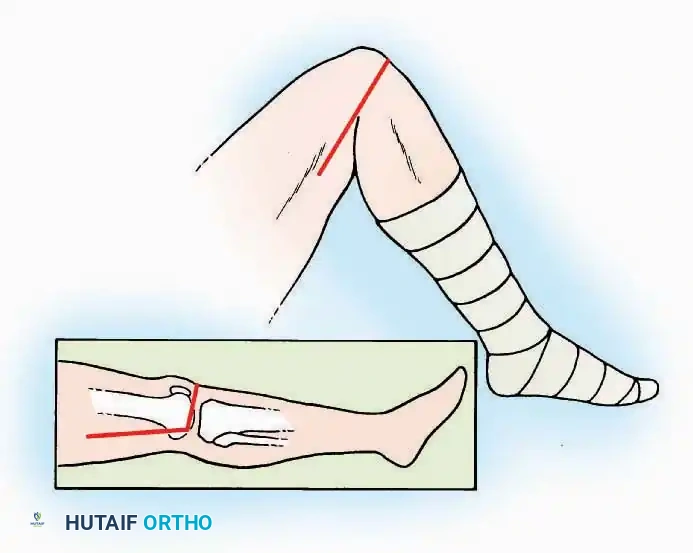
Approaches to the Interphalangeal (IP) Joints
💡 Clinical Pearl
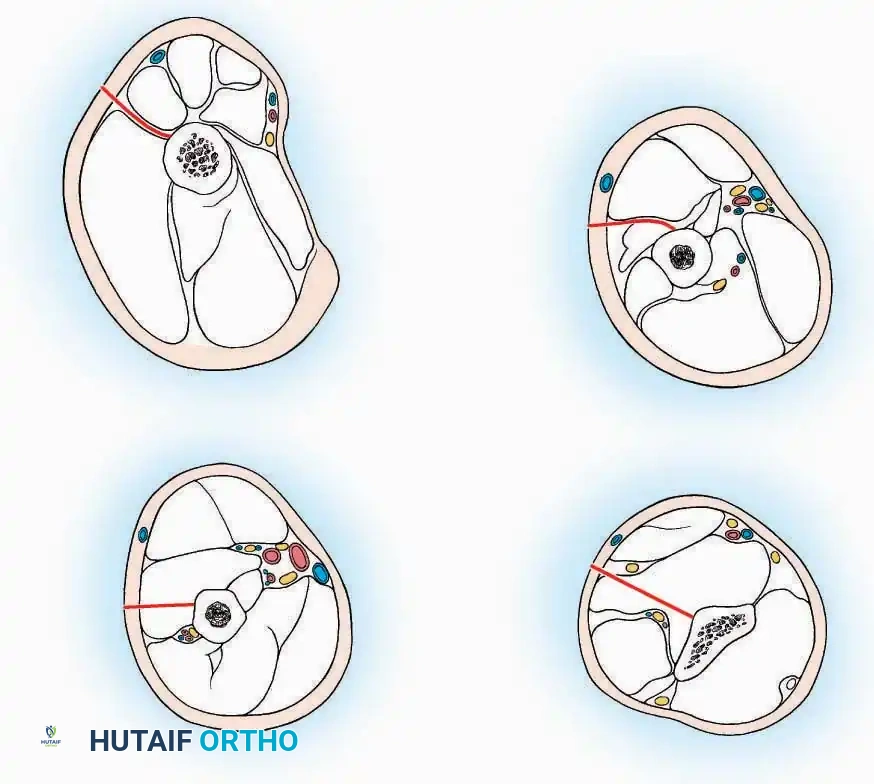
The neurovascular bundles of the toes run in the plantar-medial and plantar-lateral quadrants. Dorsal incisions or midaxial incisions are preferred to avoid painful plantar scars and iatrogenic nerve injury.
Indications: Arthrodesis for hammer toe deformities, excision of intra-articular osteophytes, or reduction of irreducible dislocations.
Surgical Technique:
* Great Toe: Make a 2.5 cm longitudinal incision strictly on the medial midaxial aspect of the toe.
* Fifth Toe: Utilize a lateral midaxial incision to avoid interdigital maceration.
* Lesser Toes (2nd, 3rd, 4th): Approach the IP joints through a dorsal longitudinal incision placed just lateral to the corresponding extensor digitorum longus (EDL) tendon.
* Deep Dissection: Carry the dissection sharply through the subcutaneous tissue and superficial fascia directly to the joint capsule.
* Neurovascular Protection: Reflect the skin edges with meticulous care. Retract the dorsal digital nerves and vessels dorsally, and the plantar nerves and vessels plantarward.
* Capsulotomy: Open the capsule either transversely (for joint resection/arthrodesis) or longitudinally (for exploration), exposing the articular surfaces.
Approaches to the Metatarsophalangeal (MTP) Joint of the Great Toe
The first MTP joint is the epicenter of forefoot reconstructive surgery. Exposure can be achieved via medial or dorsomedial trajectories.
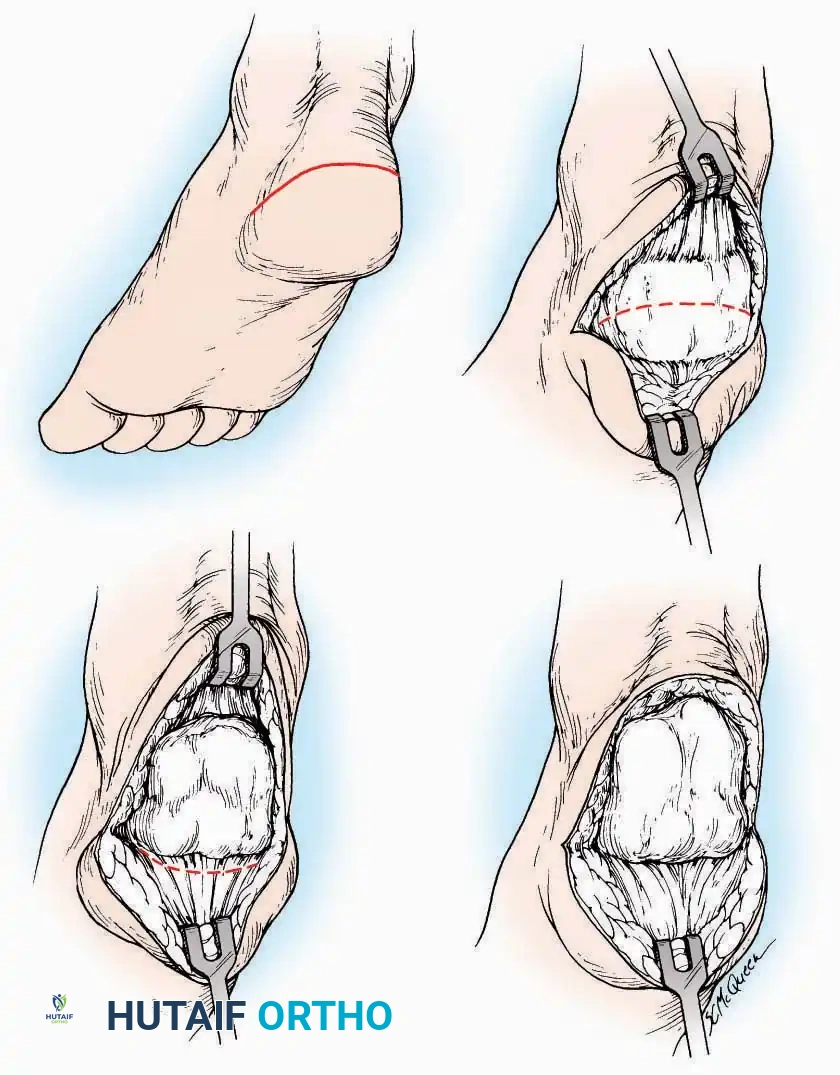
Medial Approach
Indications: Hallux valgus correction (bunionectomy), first MTP arthrodesis, or cheilectomy.
Surgical Technique:
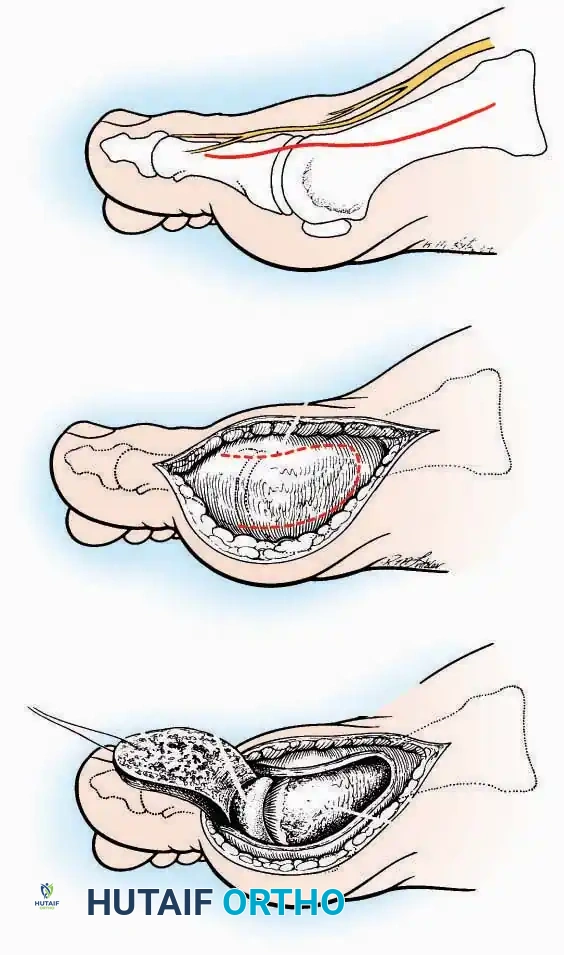
* Incision: Make a curved incision 5 cm long on the medial aspect of the joint. Begin just proximal to the IP joint, curve it over the dorsum of the MTP joint (medial to the extensor hallucis longus [EHL] tendon), and terminate on the medial aspect of the first metatarsal 2.5 cm proximal to the joint.
* Superficial Dissection: As the deep fascia is incised, identify and laterally retract the medial branch of the first dorsal metatarsal artery and the medial branch of the dorsomedial nerve (a terminal branch of the superficial peroneal nerve).
* Deep Dissection: Dissect the fascia from the dorsum down to the bursa overlying the medial eminence of the metatarsal head.
* Capsulotomy: Make a curved incision through the bursa and joint capsule. Begin dorsomedially, continue proximally dorsal to the metatarsal head, sweep plantarward, and end distally on the medioplantar aspect of the joint. This creates an elliptical, racquet-shaped flap attached at the base of the proximal phalanx.
⚠️ Surgical Pitfall
While distal reflection of this racquet flap provides ample exposure of the first MTP joint, the extensive subfascial undermining required can compromise the vascularity of the skin flap, leading to delayed healing or necrosis. Consequently, the dorsomedial approach is often preferred in modern practice.
Dorsomedial Approach
Indications: Preferred approach for primary and revision first MTP arthroplasty, arthrodesis, and complex bunion corrections due to superior angiosome preservation.
Surgical Technique:
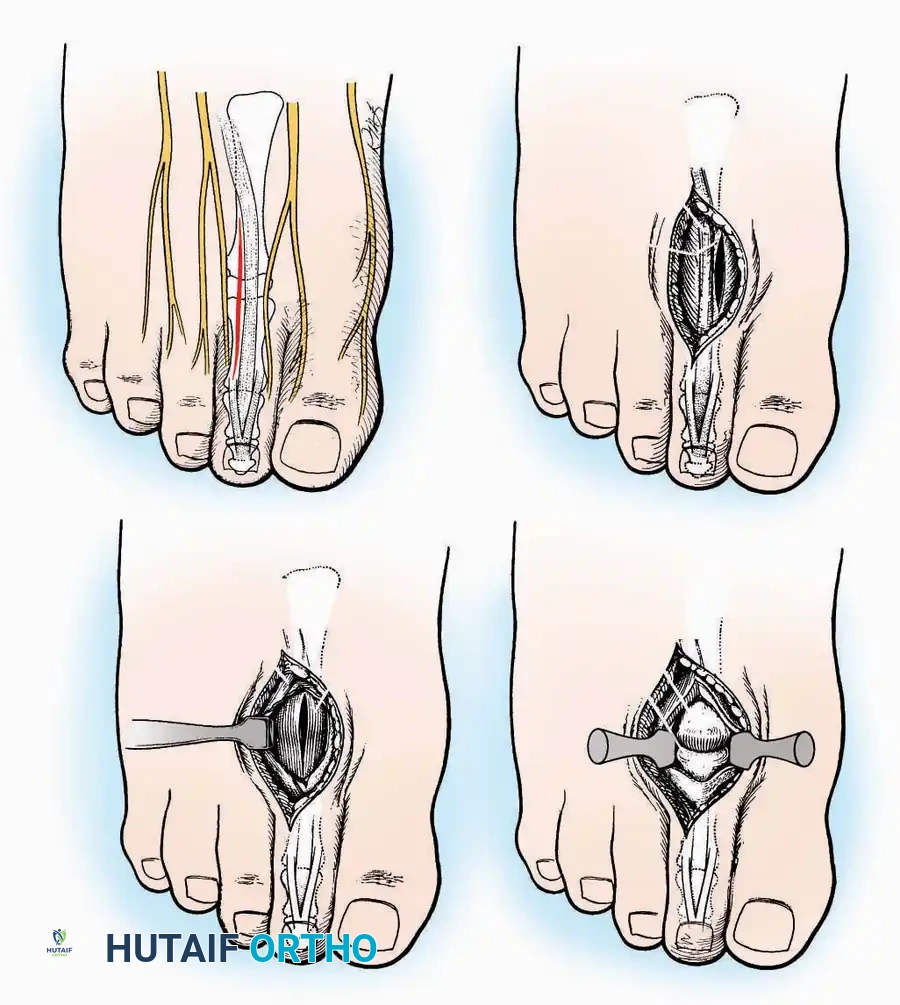
* Incision: Begin just proximal to the IP joint and extend proximally for 5 cm, running parallel and strictly medial to the EHL tendon.
* Exposure: Divide the superficial fascia. Identify and retract the EHL tendon laterally.
* Capsulotomy: The capsule can be incised longitudinally in the exact plane of the skin incision, allowing for subperiosteal elevation of the capsule medially and laterally, preserving the vascular supply to the medial skin flap.
Approaches to the Metatarsophalangeal Joints of the Lesser Toes
Indications: Metatarsal head resections (Weil osteotomies), plantar plate repairs, or correction of severe crossover toe deformities.
Surgical Technique:
* Incision (2nd, 3rd, 4th Toes): Utilize a dorsolateral longitudinal incision parallel to the corresponding extensor tendon. This avoids the primary dorsal cutaneous nerves which typically run strictly dorsally.
* Incision (5th Toe): Best exposed via a straight or gently curved dorsal or dorsolateral incision to avoid the lateral shoe-wear friction zone.
* Capsulotomy: The joint capsules are opened longitudinally. For adjacent MTP pathology (e.g., 2nd and 3rd MTP joints), a single dorsal incision placed in the intermetatarsal space can be utilized to access both joints via medial and lateral subfascial windows.
SURGICAL APPROACHES TO THE CALCANEUS
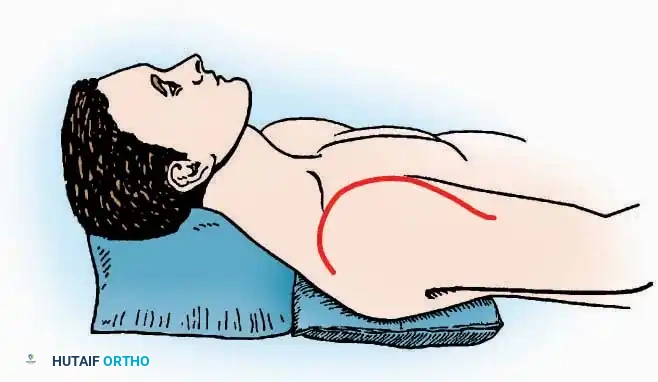
Approaches to the calcaneus are dictated by the pathology—trauma (intra-articular fractures) versus tumor/infection. Positioning is critical; while the prone position offers excellent bilateral access, the lateral decubitus or modified supine positions are more frequently utilized for unilateral trauma.
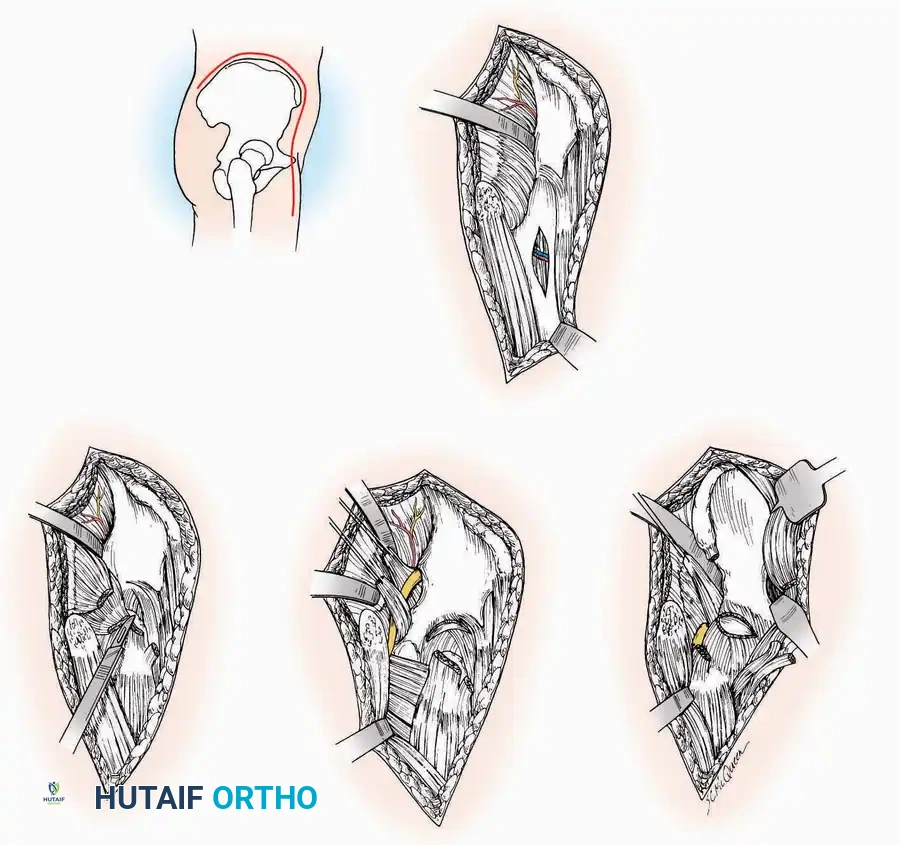
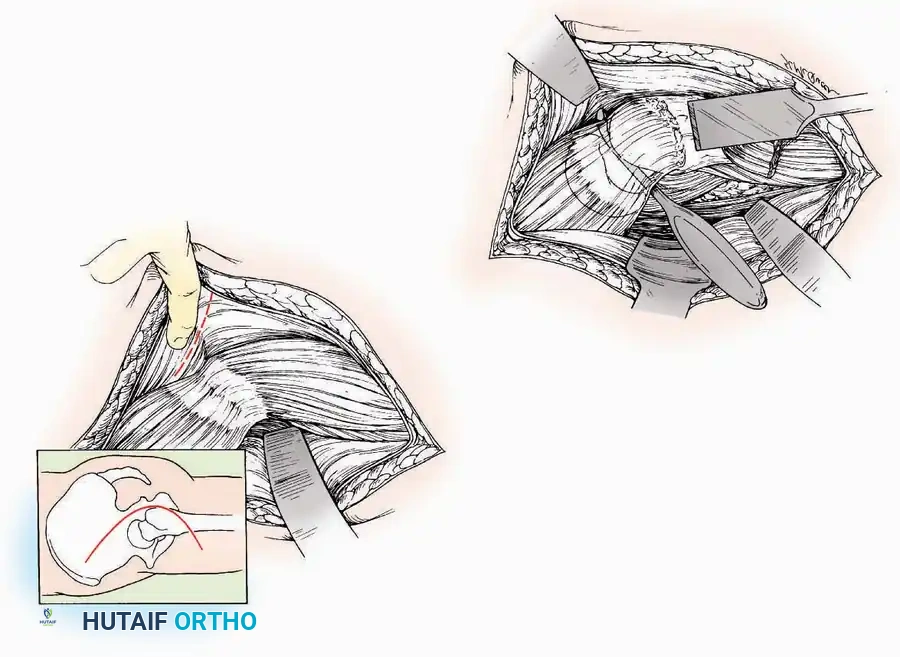
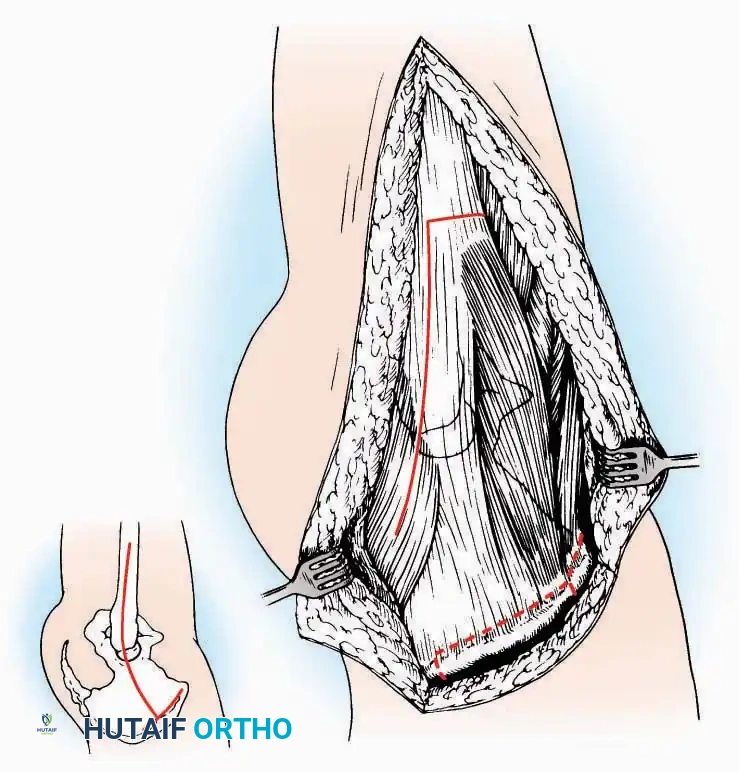
Lateral Approach (Extensile Lateral)
This is the workhorse approach for open reduction and internal fixation (ORIF) of displaced intra-articular calcaneal fractures.
Indications: ORIF of calcaneus fractures, lateral wall exostectomy, subtalar arthrodesis.
Positioning: Lateral decubitus with the operative leg up, or supine with a large bump under the ipsilateral hip to internally rotate the leg.
Surgical Technique:
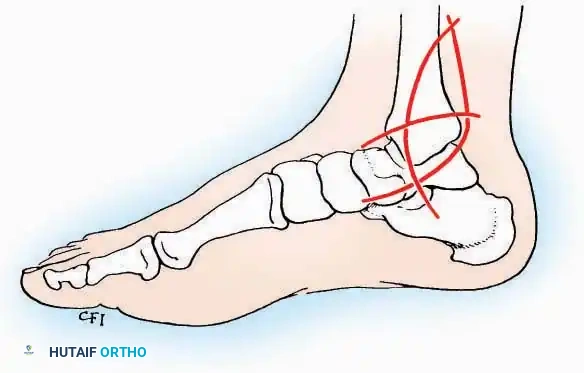
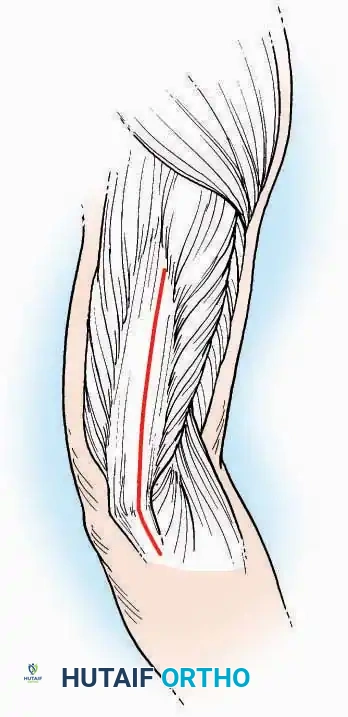
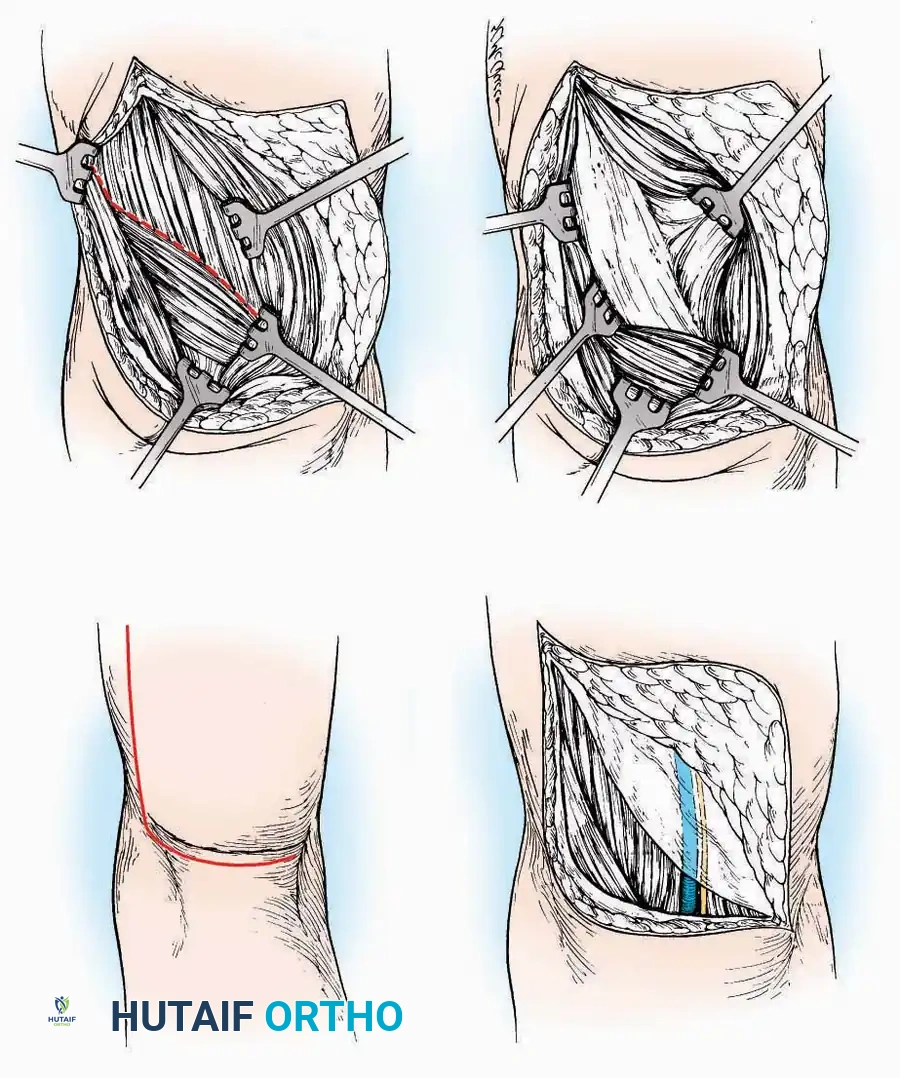
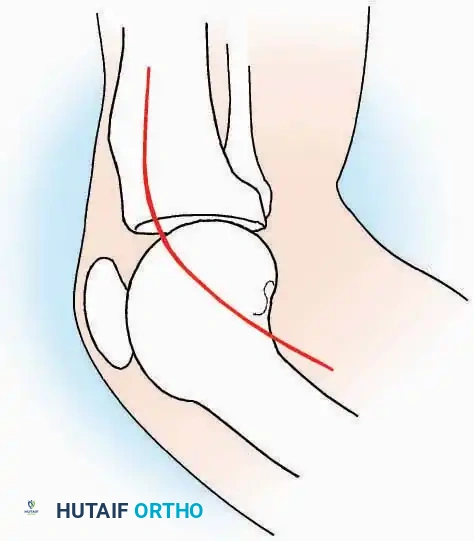
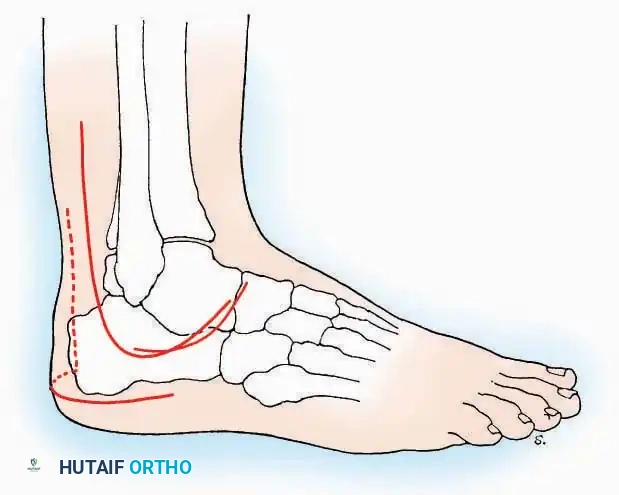
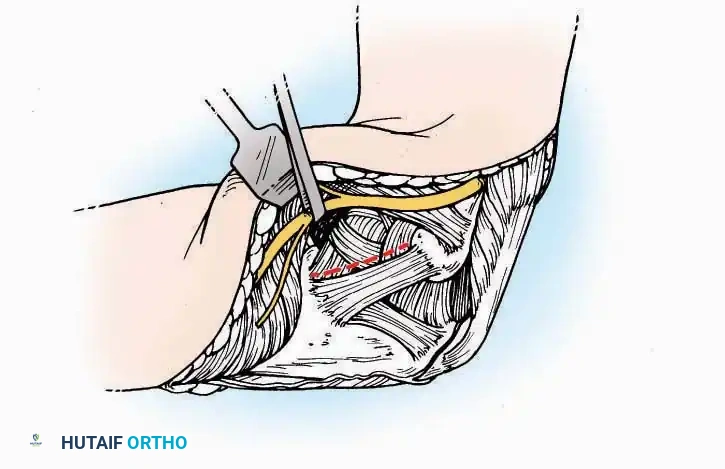
* Incision: Begin the incision on the lateral margin of the Achilles tendon near its insertion. Extend it distally to a point 4 cm inferior and 2.5 cm anterior to the lateral malleolus. (For trauma, a classic L-shaped extensile incision is often used, dropping straight down anterior to the Achilles, then curving gently toward the base of the 5th metatarsal).
* Superficial Dissection: Divide the superficial and deep fasciae. It is imperative to create a "full-thickness" flap containing skin, subcutaneous fat, and periosteum to prevent flap necrosis.
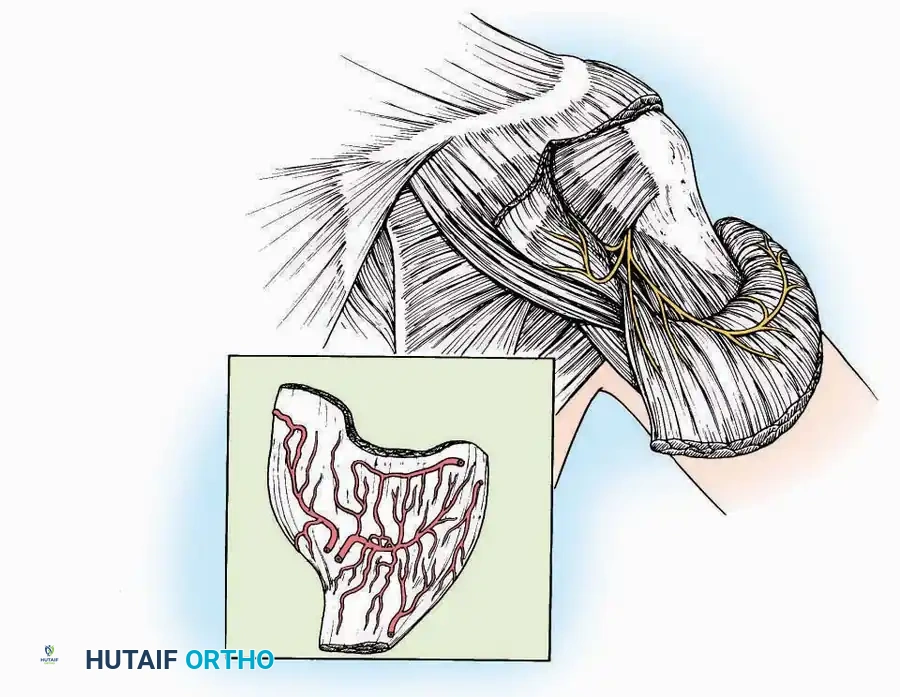
* Nerve Protection: The sural nerve crosses the proximal and distal limbs of this approach. It must be identified and protected within the anterior flap.
* Deep Dissection: Isolate the peroneal tendons (longus and brevis). Incise and elevate the periosteum below the tendons to expose the lateral wall of the calcaneus.
* Tendon Management: If severe deformity or infection is present, the peroneal tendons may be divided via Z-plasty and repaired at the conclusion of the case, though this is rarely necessary in modern fracture care.
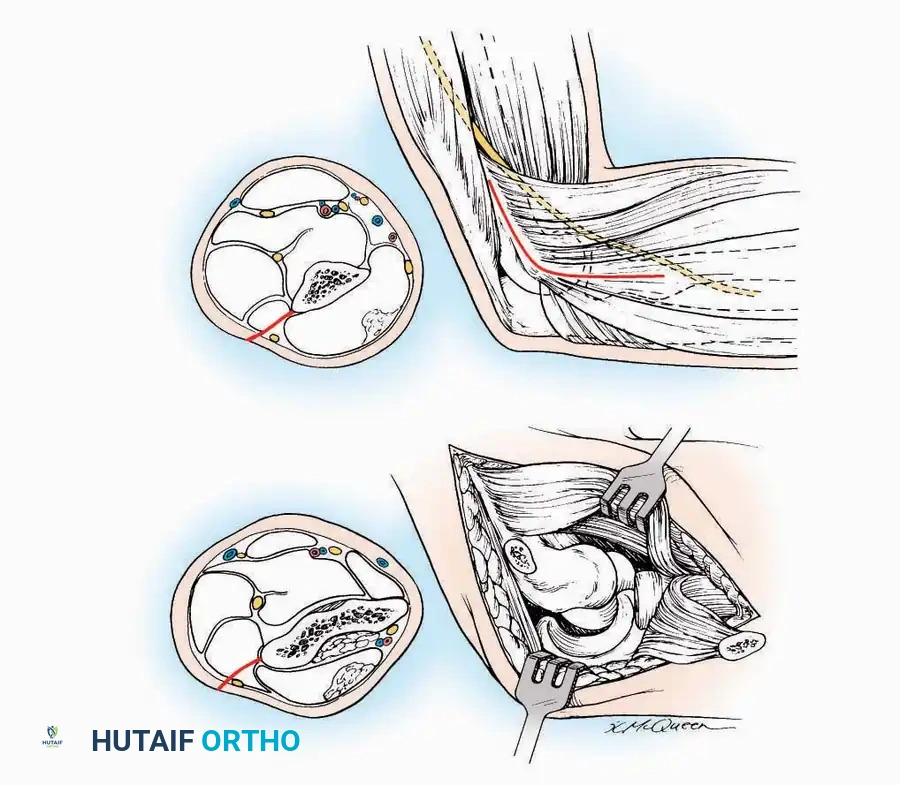
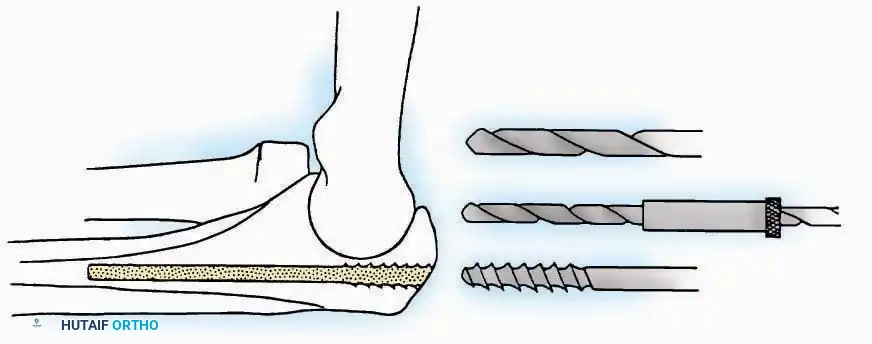
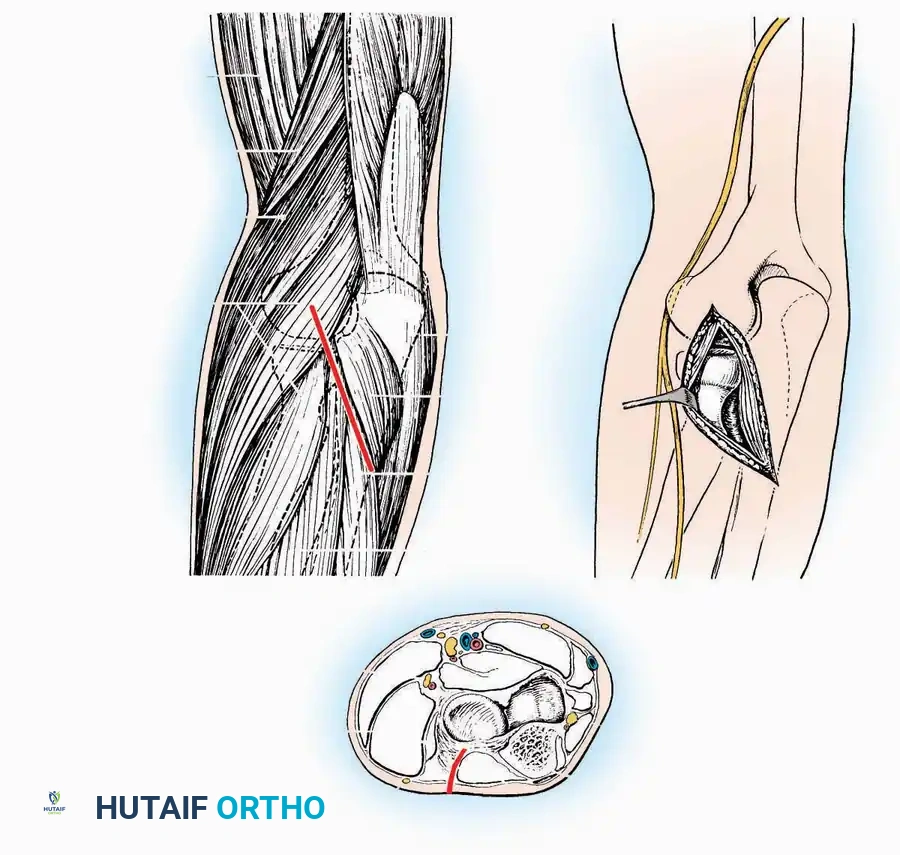
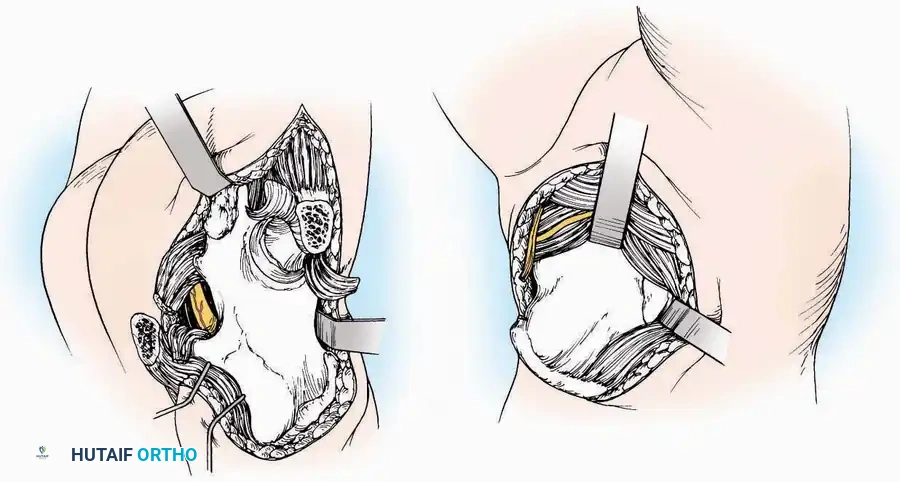
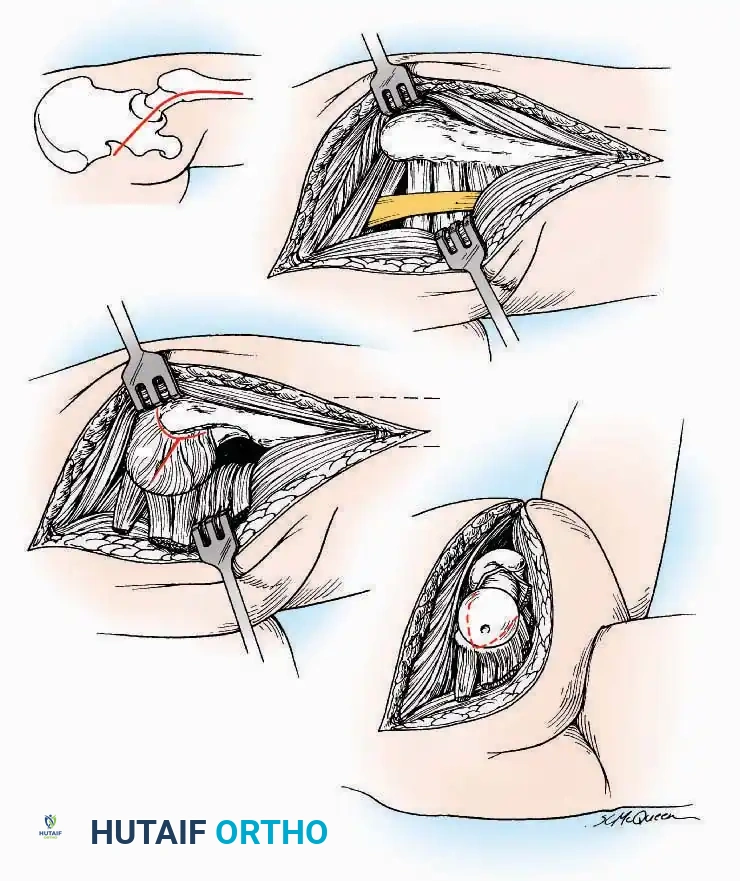
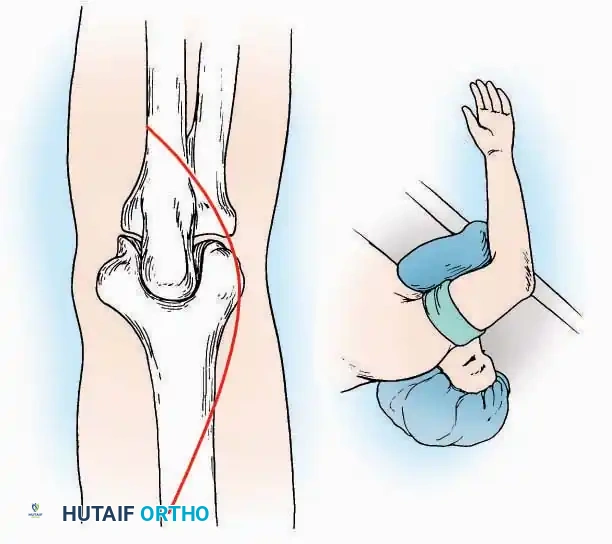
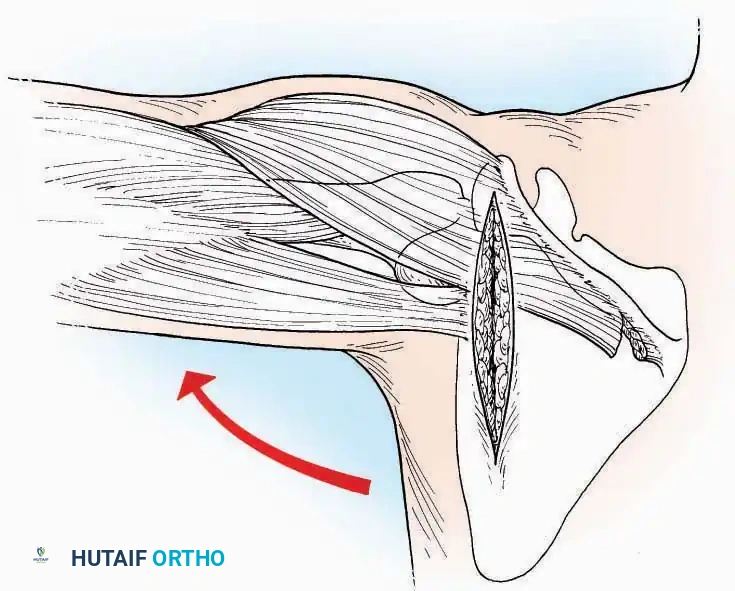
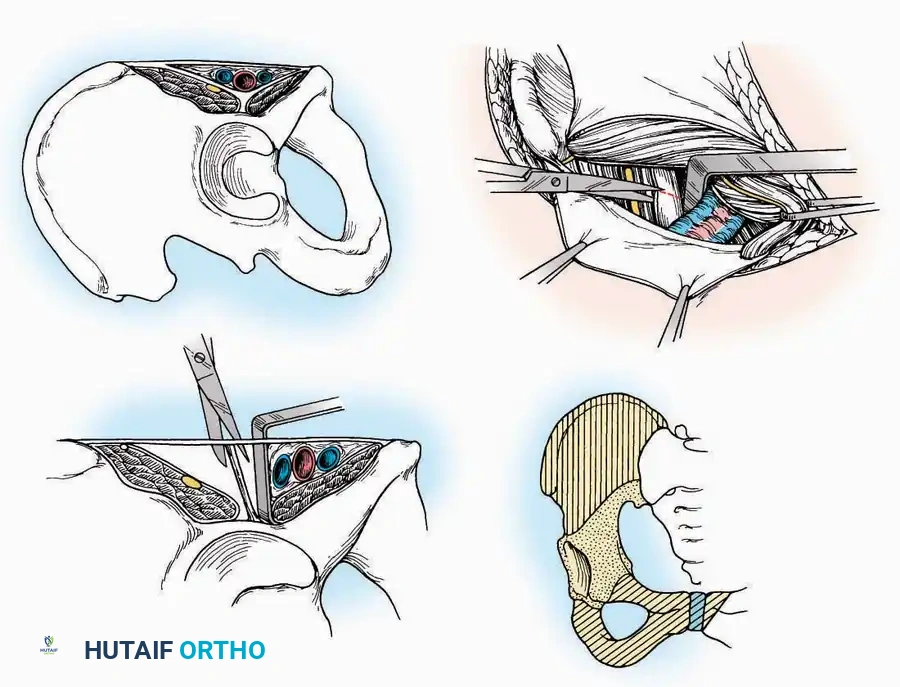
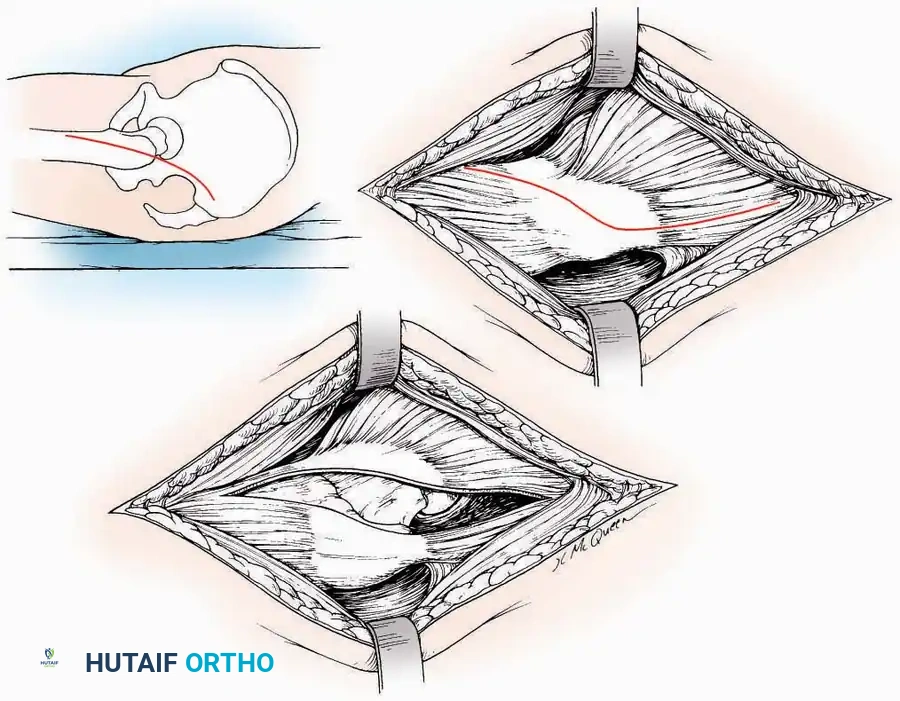
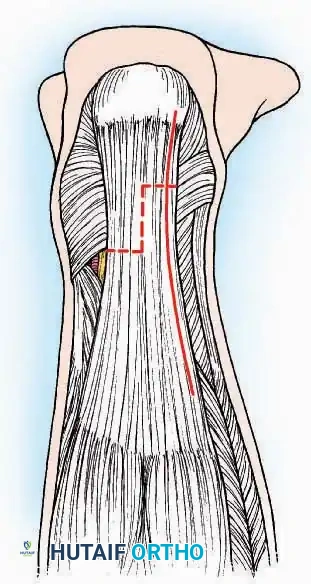
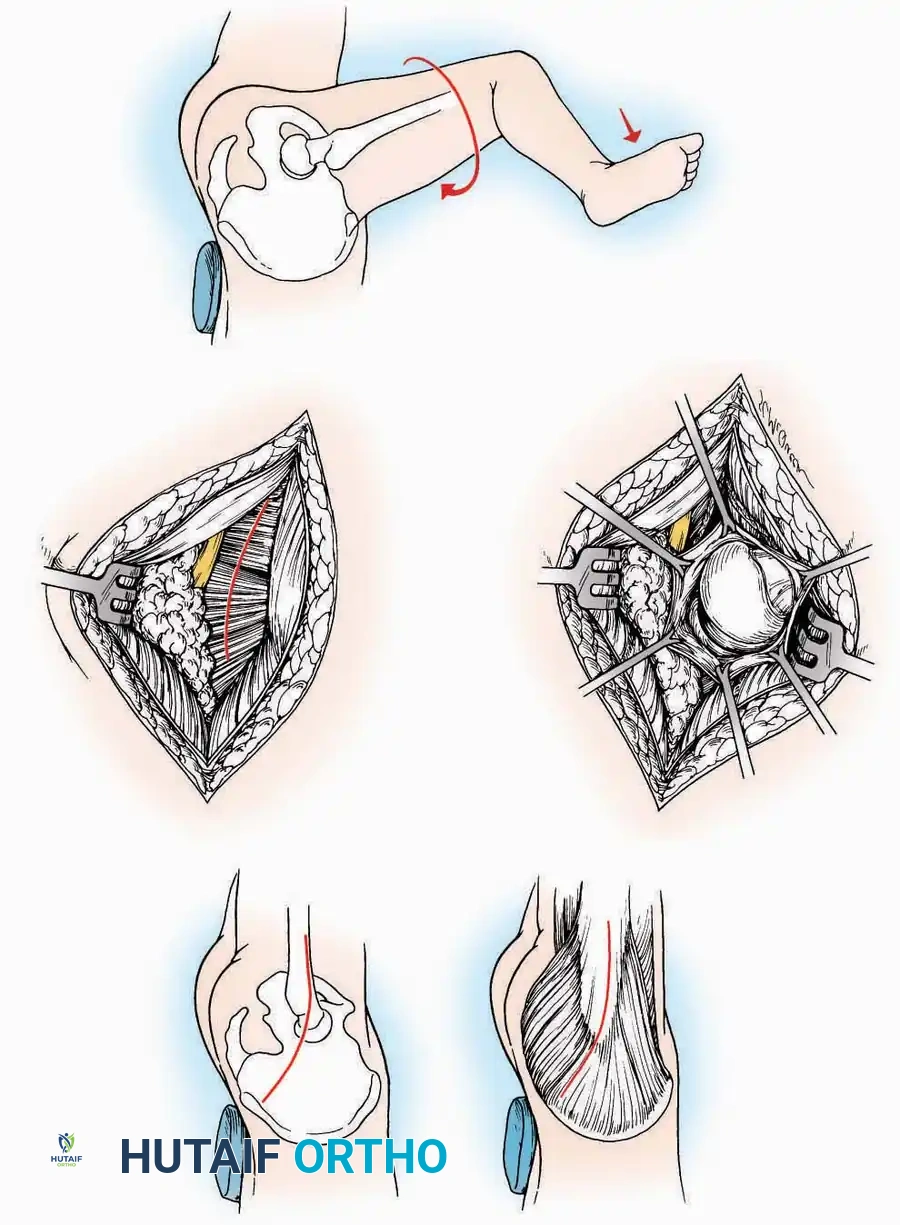
Medial Approach
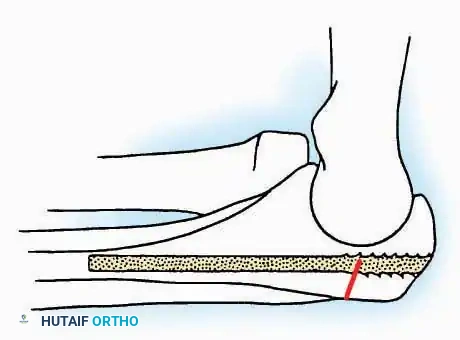
Indications: Fixation of sustentaculum tali fractures, medial process fractures, or excision of medial tarsal coalitions.
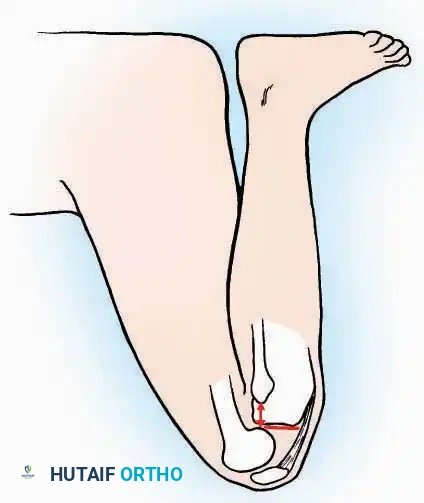
Positioning: Supine with the hip externally rotated and knee flexed (figure-of-four position).
Surgical Technique:
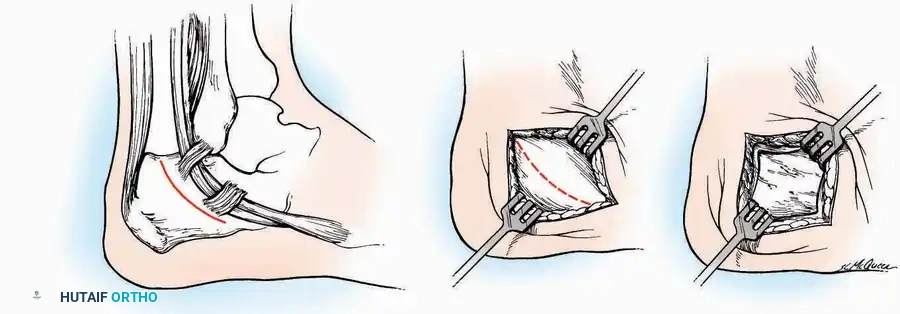
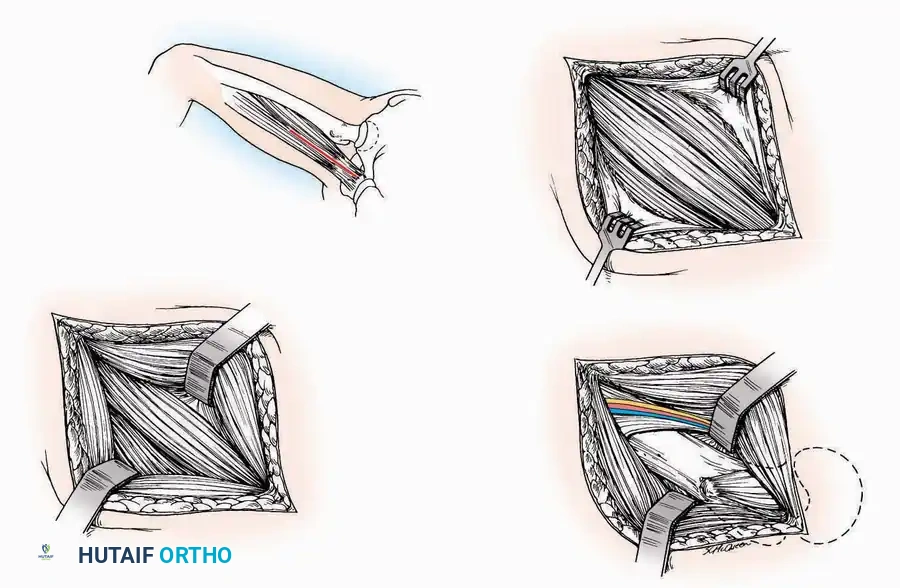
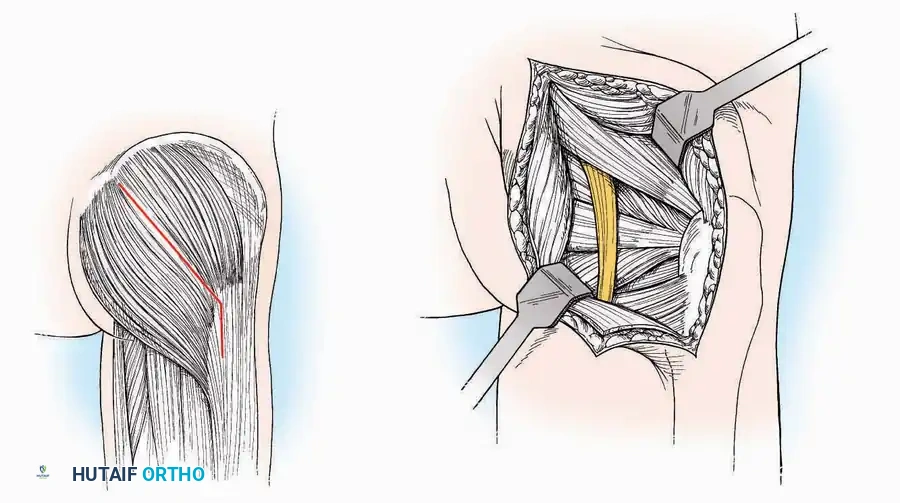
* Incision: Begin 2.5 cm anterior and 4 cm inferior to the medial malleolus. Carry it posteriorly along the medial surface of the foot toward the Achilles tendon.
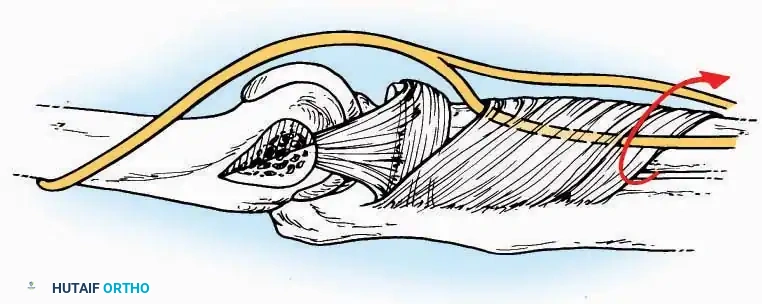
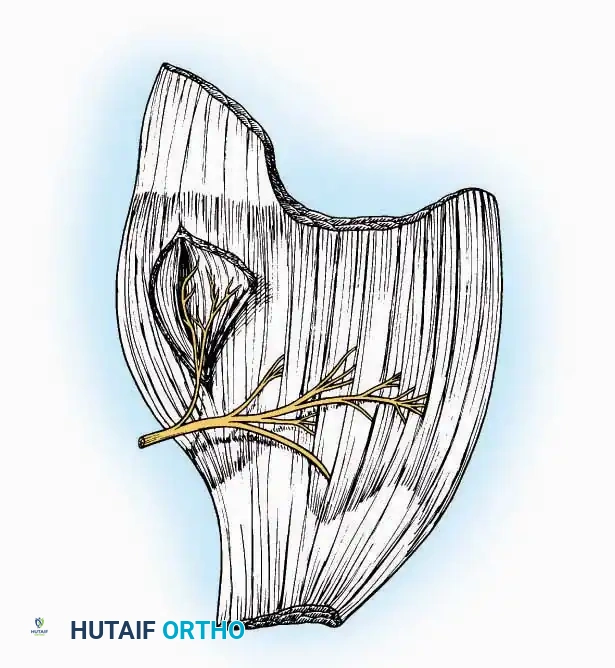
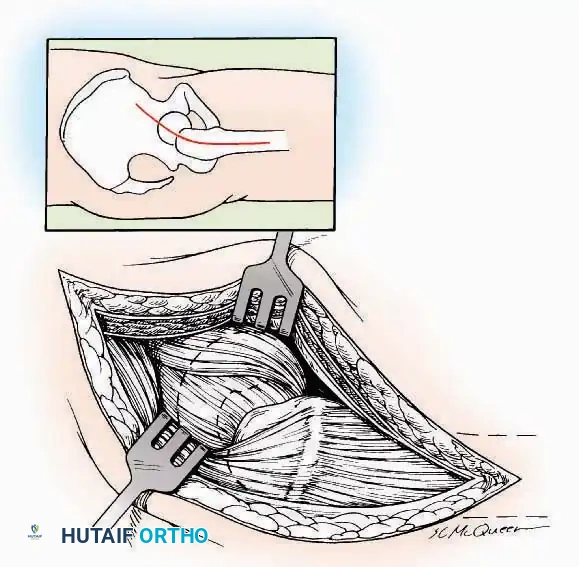
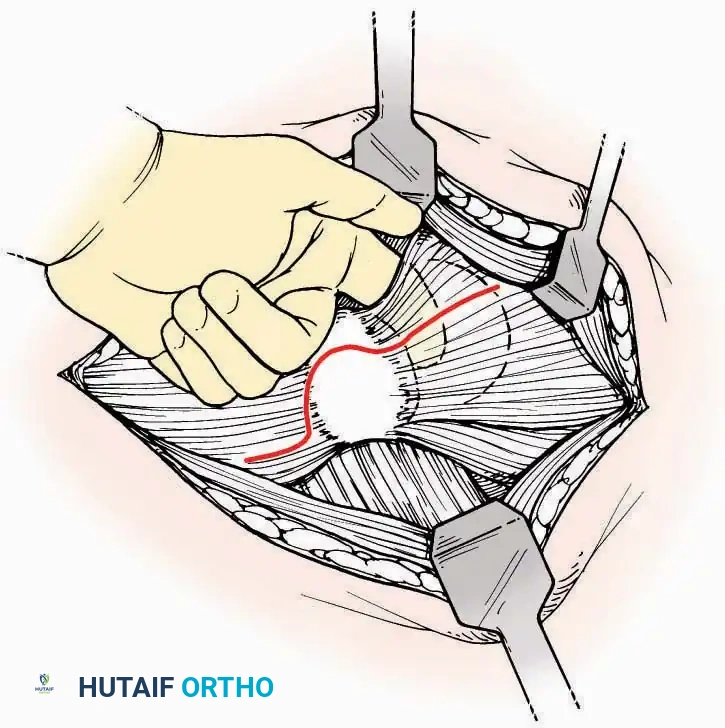
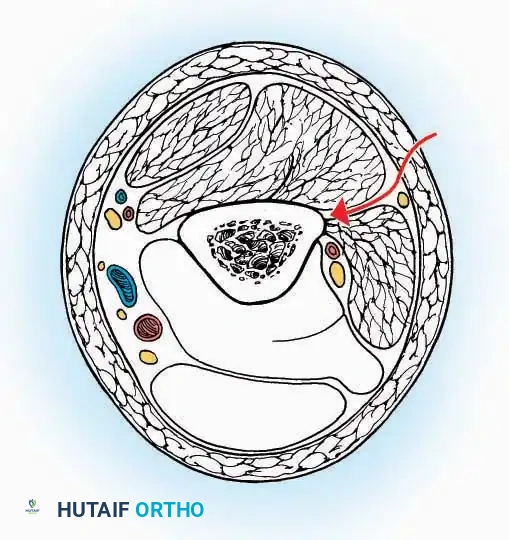
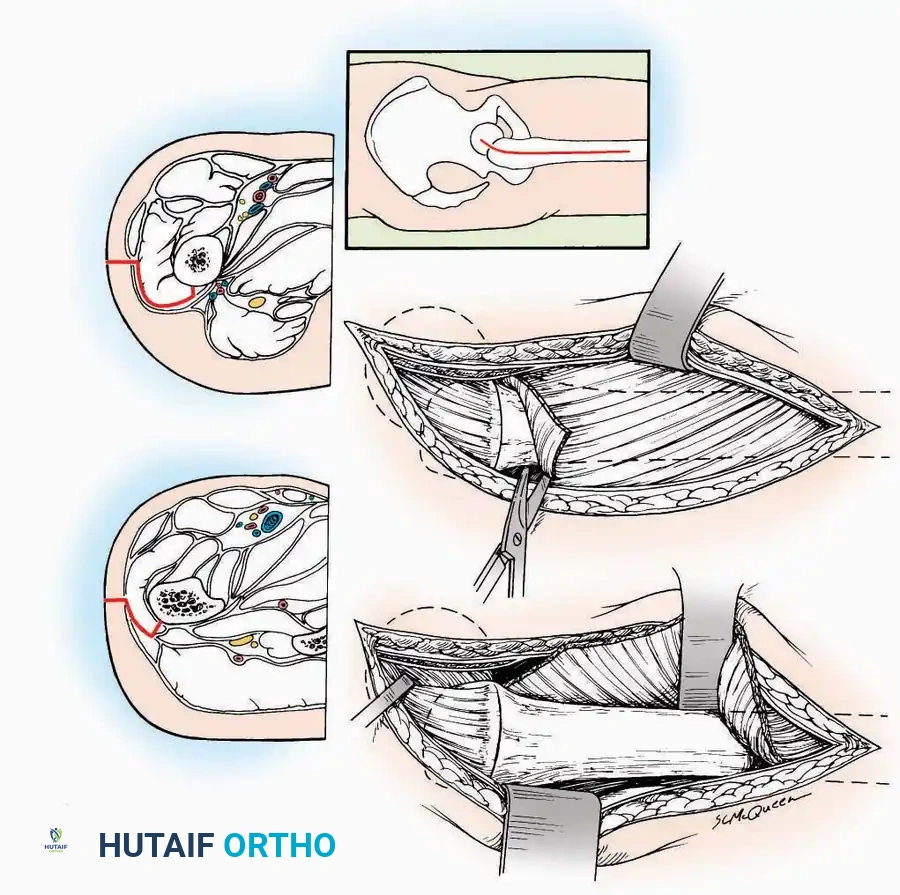
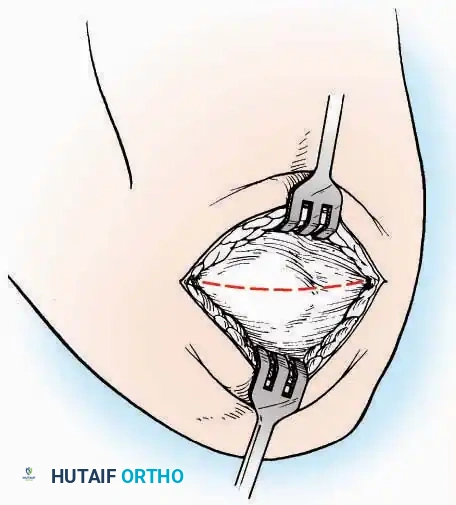
* Superficial Dissection: Divide the fat and fascia to define the inferior margin of the abductor hallucis muscle.
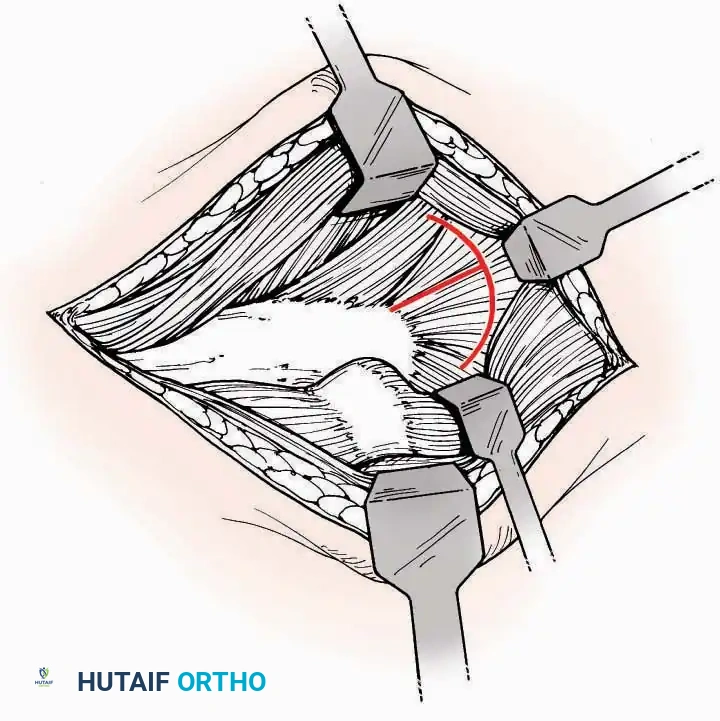
* Deep Dissection: Mobilize the abductor hallucis muscle belly and retract it dorsally to expose the medial and inferomedial aspects of the calcaneal body.
* Plantar Exposure: Continue distally by dividing the plantar aponeurosis and the muscular attachments to the calcaneus, or strip them subperiosteally with an osteotome.
* Neurovascular Warning: Meticulously identify and protect the medial calcaneal nerve and the nerve to the abductor digiti minimi (first branch of the lateral plantar nerve), which are highly vulnerable during inferior retraction.
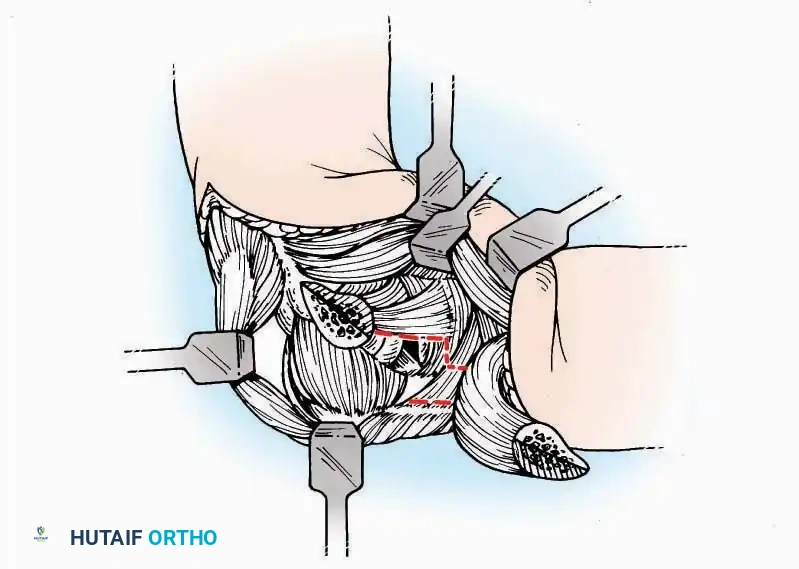
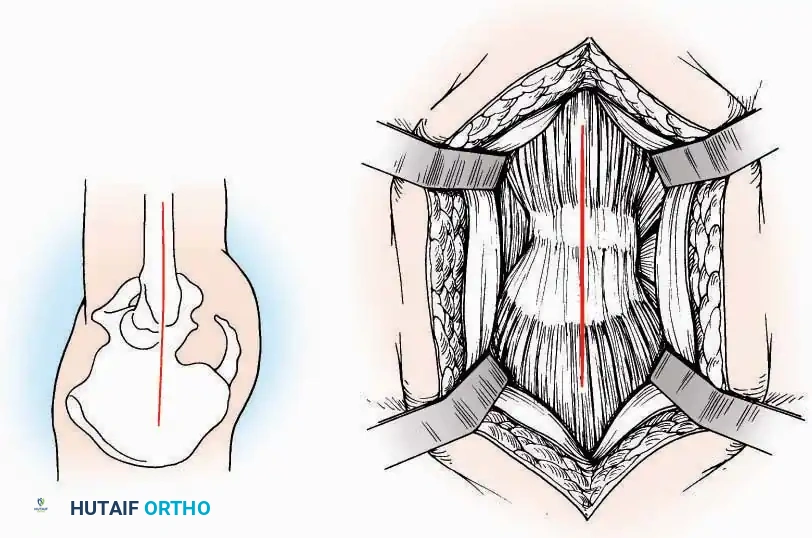
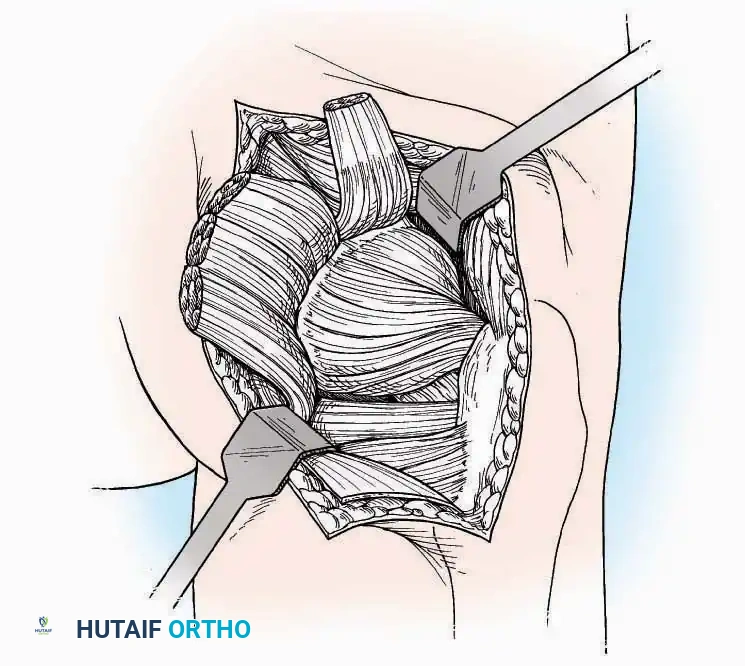
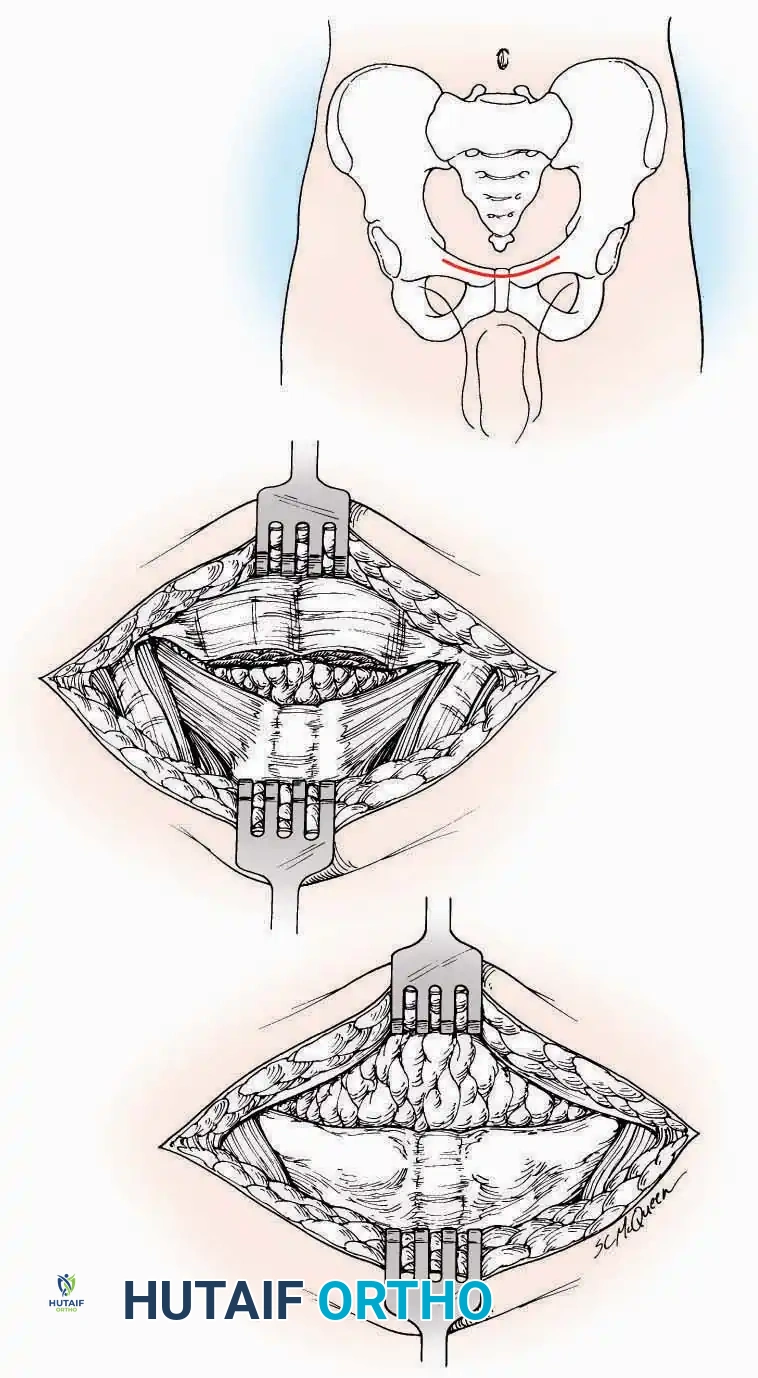
U Approach
Indications: Extensive plantar fasciotomy, radical tumor resection, or complex osteomyelitis debridement requiring access to the entire plantar surface of the calcaneus.
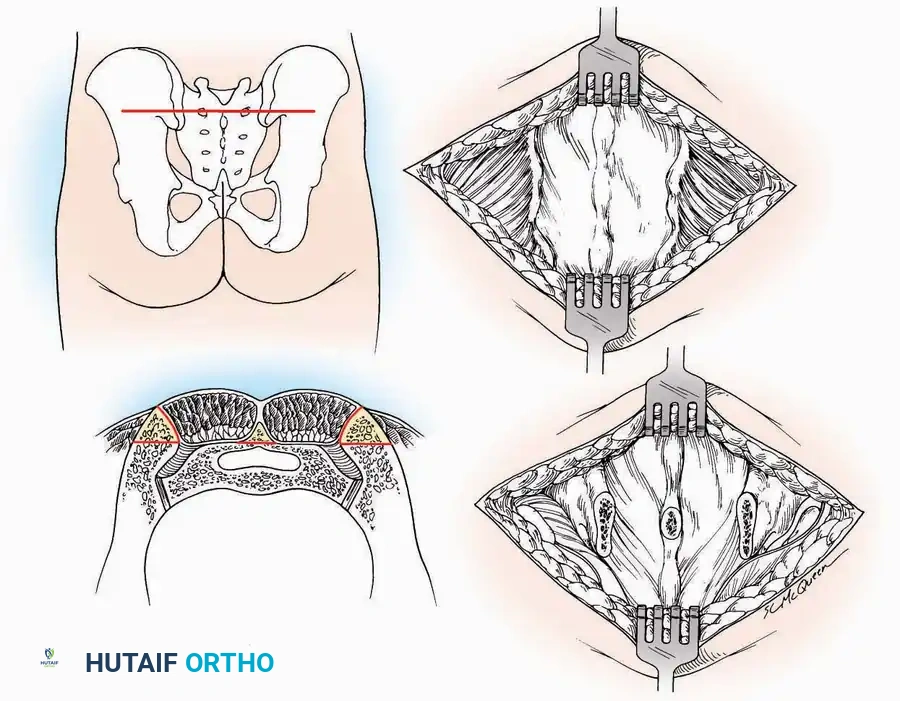
Positioning: Prone, with the leg supported on a large sandbag.
Surgical Technique:
* Incision: Join the medial and lateral approaches described above to form a large, continuous U-shaped incision around the posterior four-fifths of the calcaneus.
* Flap Elevation: Deepen the incision directly to bone. Elevate a massive plantar flap consisting of skin, the specialized fatty heel pad, and the plantar fascia. Retract this flap distally to expose the entire plantar calcaneal tuberosity.
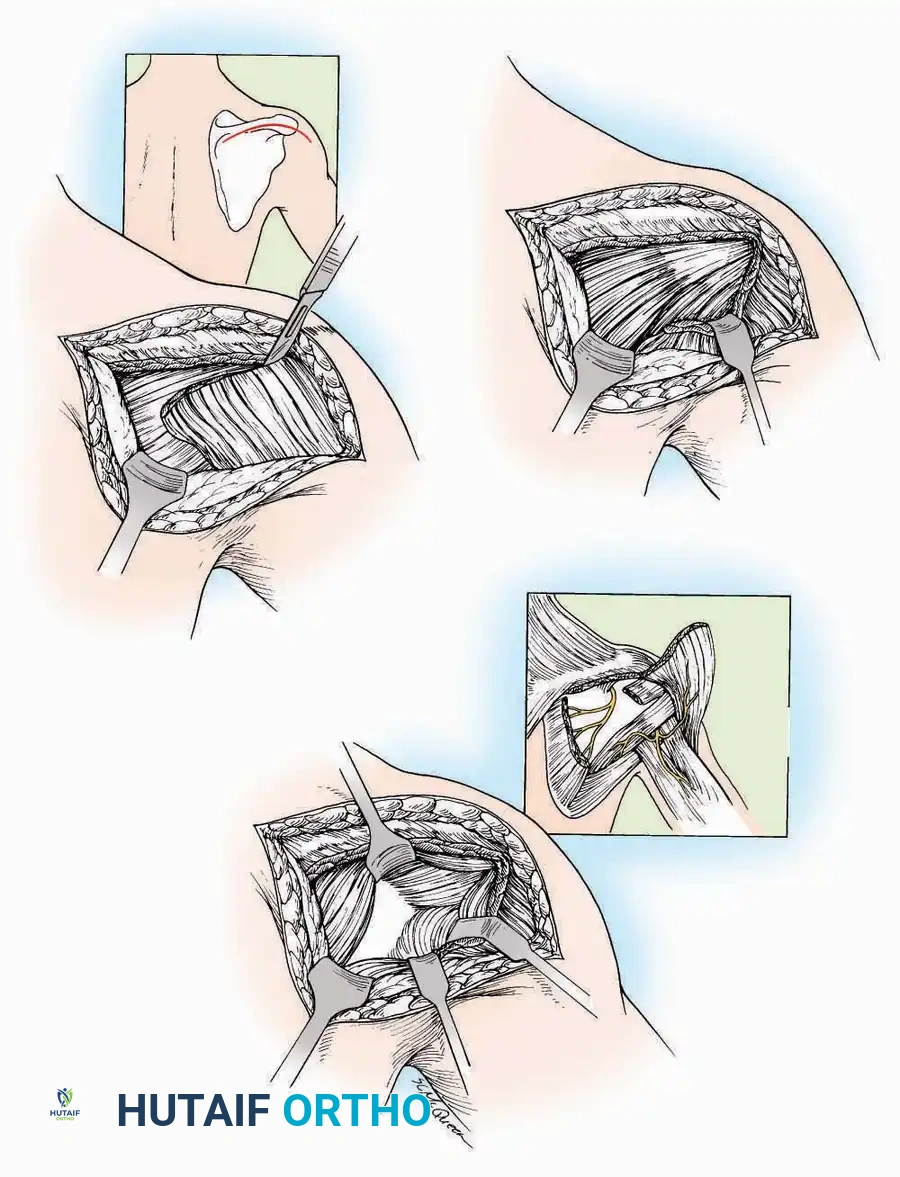
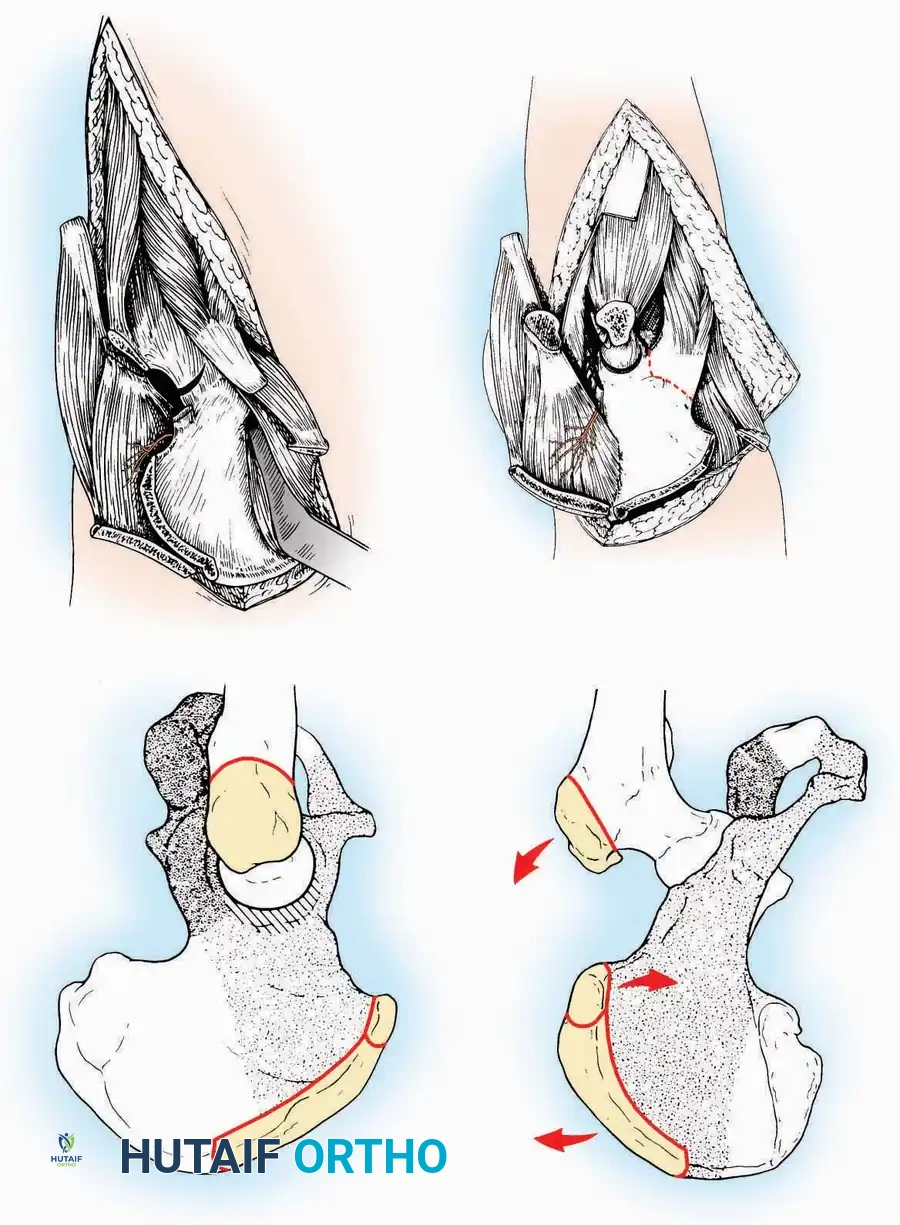
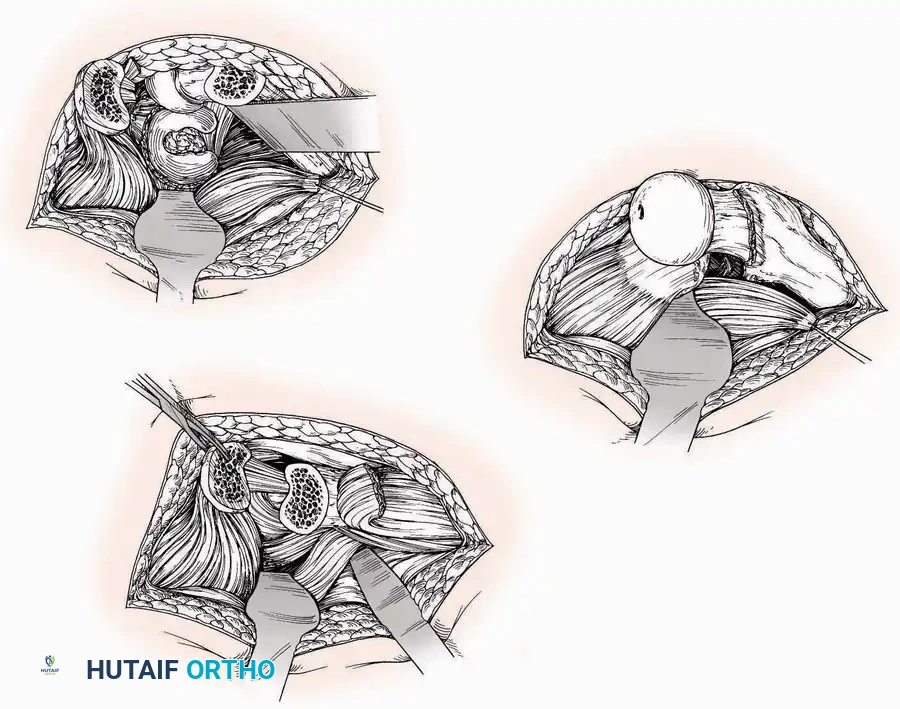
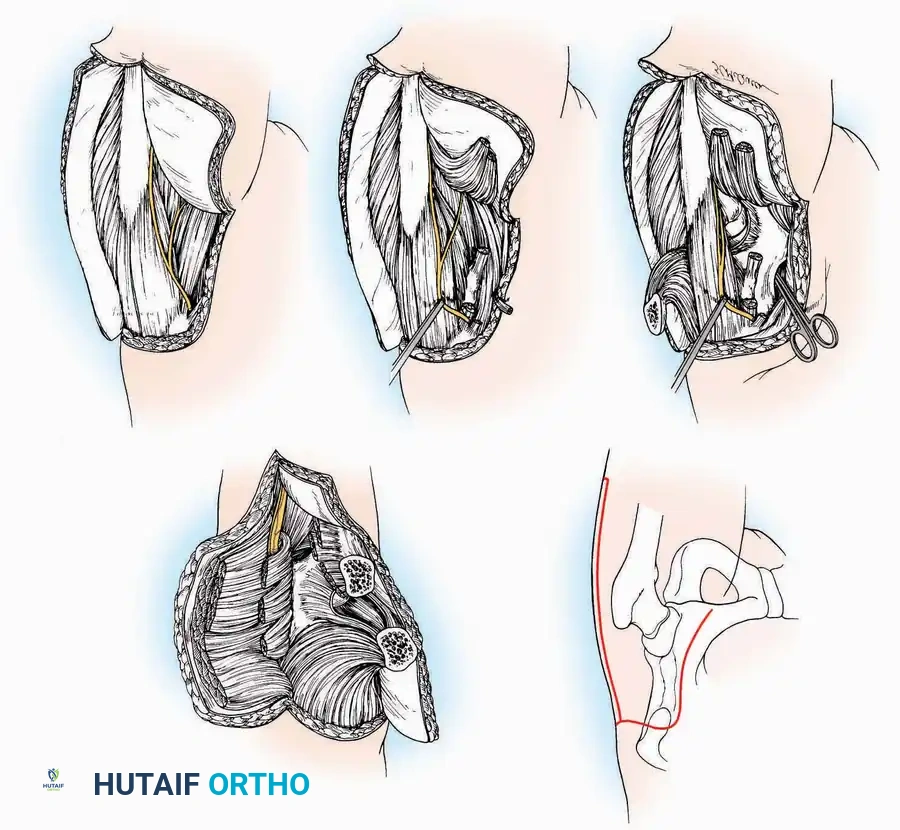
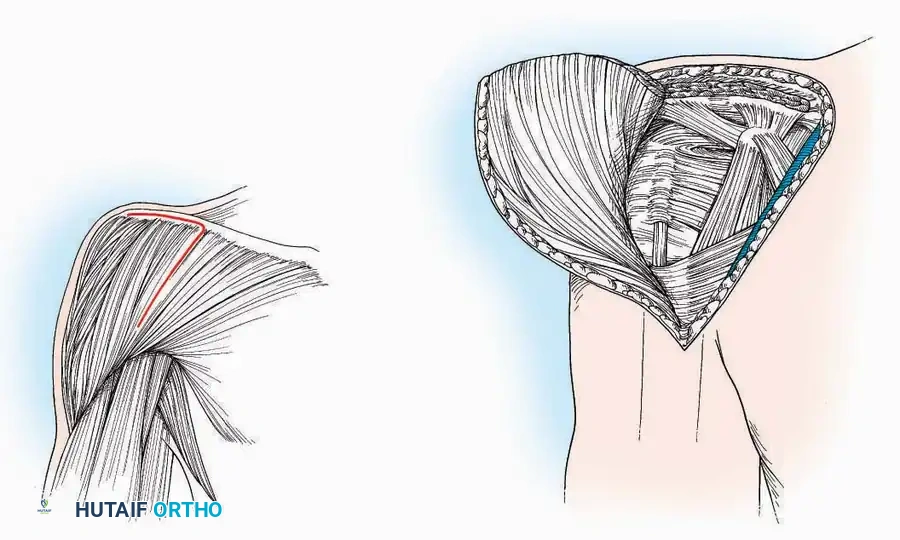
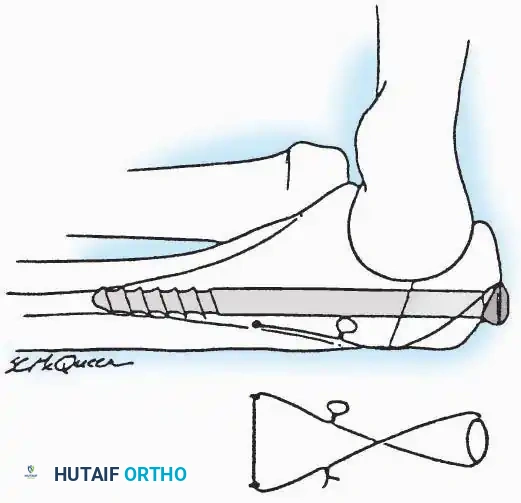
Kocher Approach (Curved L)
Indications: Complete excision of the calcaneus (calcanectomy) for malignant tumors or recalcitrant osteomyelitis.
Surgical Technique:
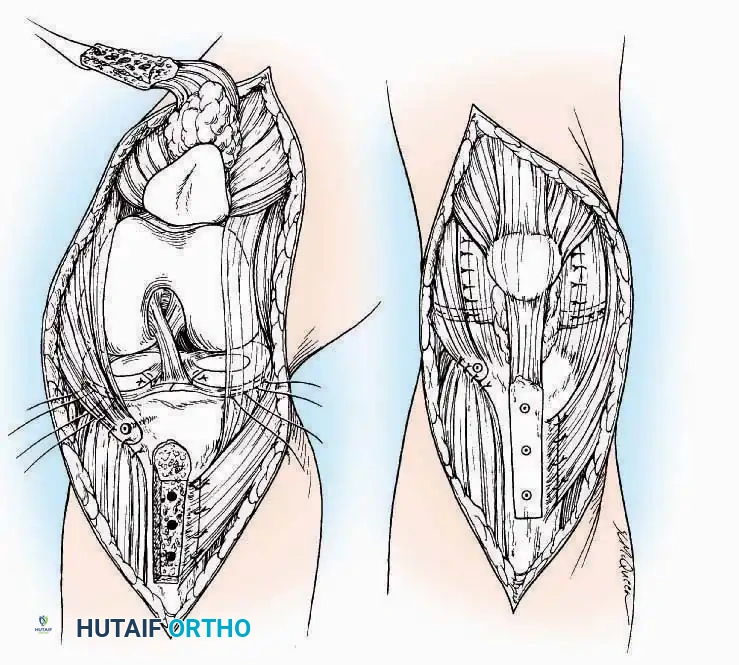
* Incision: Incise the skin over the medial border of the Achilles tendon, starting 7.5 cm proximal to the calcaneal tuberosity. Extend it distally to the inferoposterior aspect of the tuberosity, curve it transversely around the posterior heel, and continue distally along the lateral surface of the foot to the tuberosity of the fifth metatarsal.
* Deep Dissection: Divide the Achilles tendon directly at its insertion and carry the dissection down to the bone.
* Enucleation: To reach the superior surface, free all tissues beneath the severed Achilles tendon. The calcaneus can then be enucleated subperiosteally or extraperiosteally depending on the oncologic or infectious margins required.
SURGICAL APPROACHES TO THE TARSUS AND ANKLE
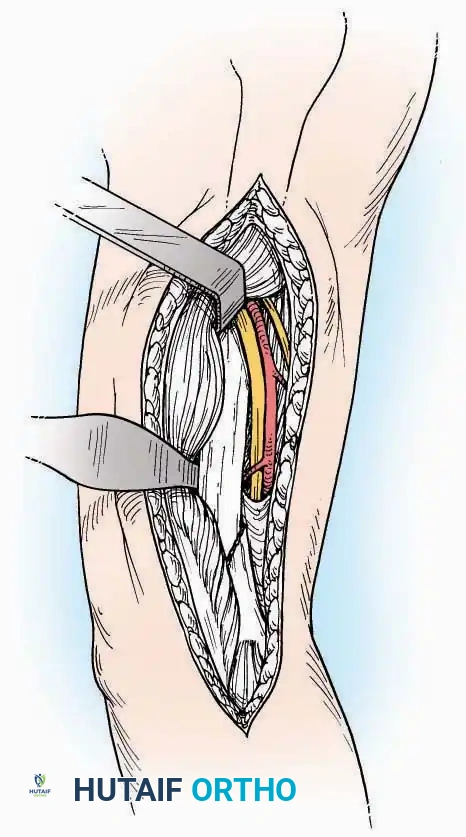
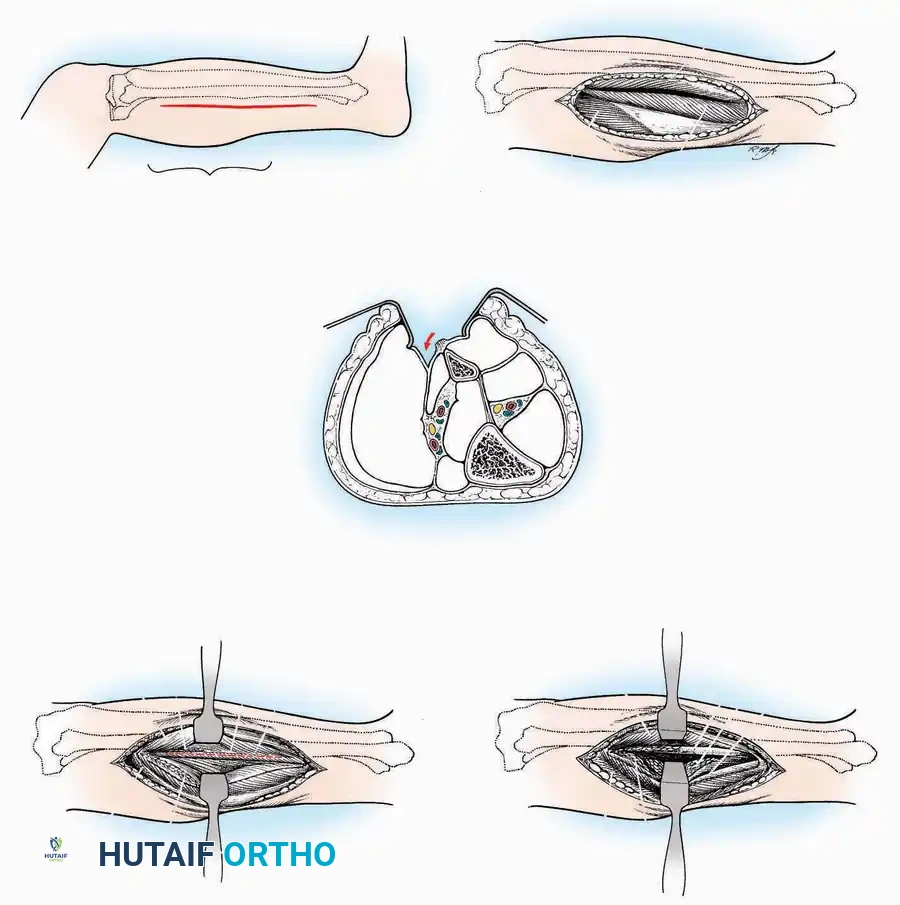
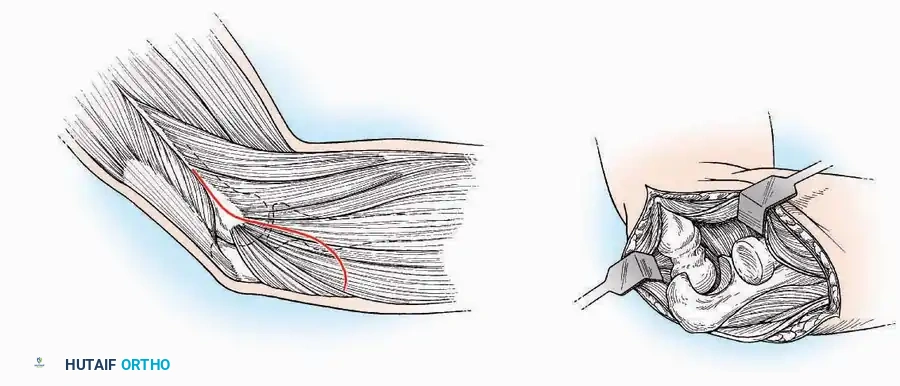
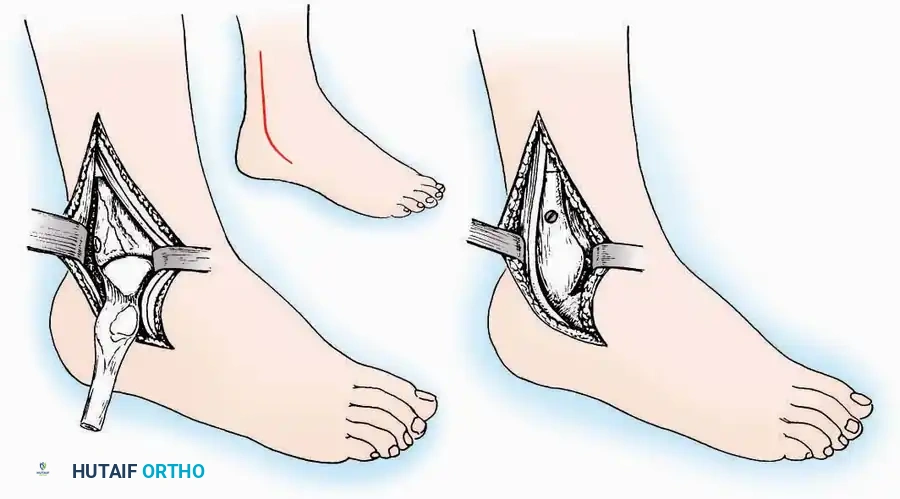
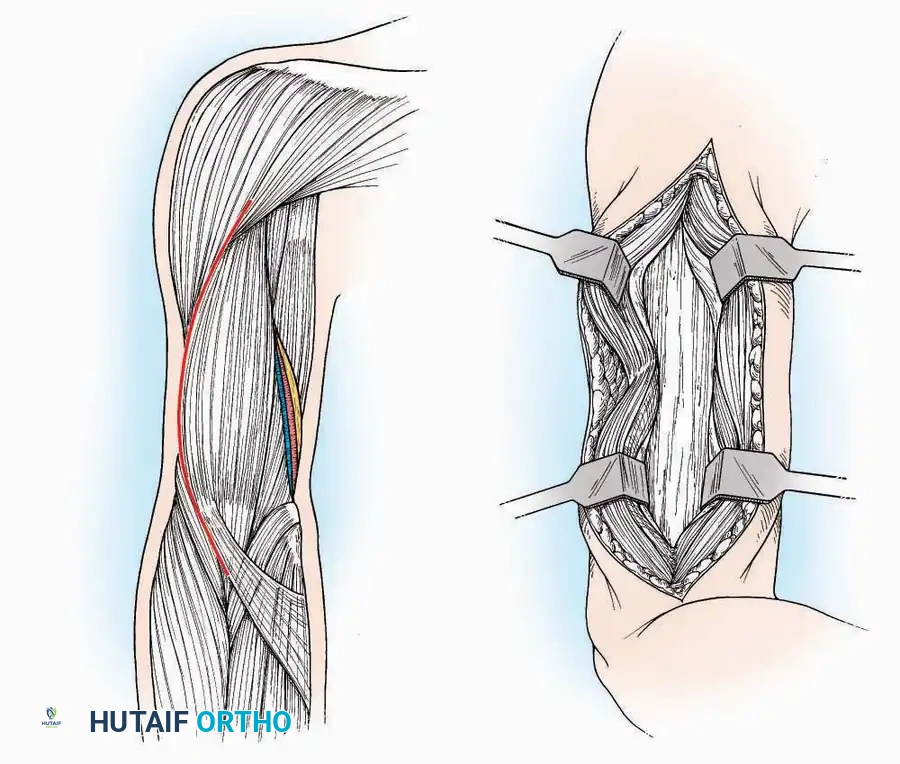
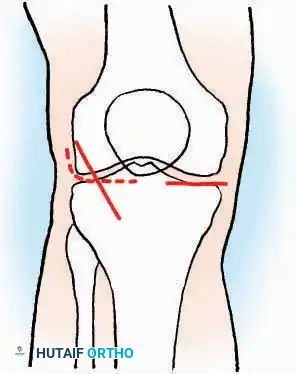
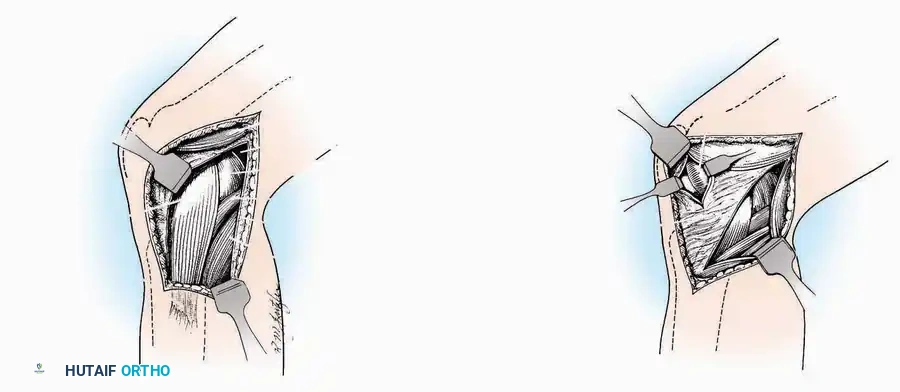
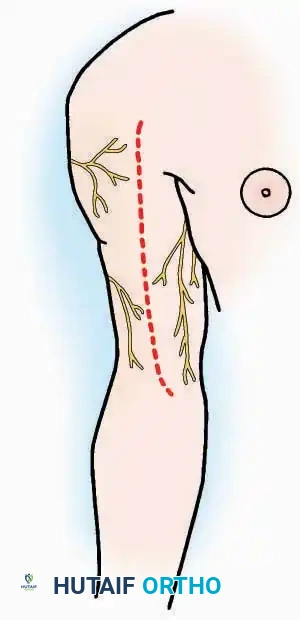
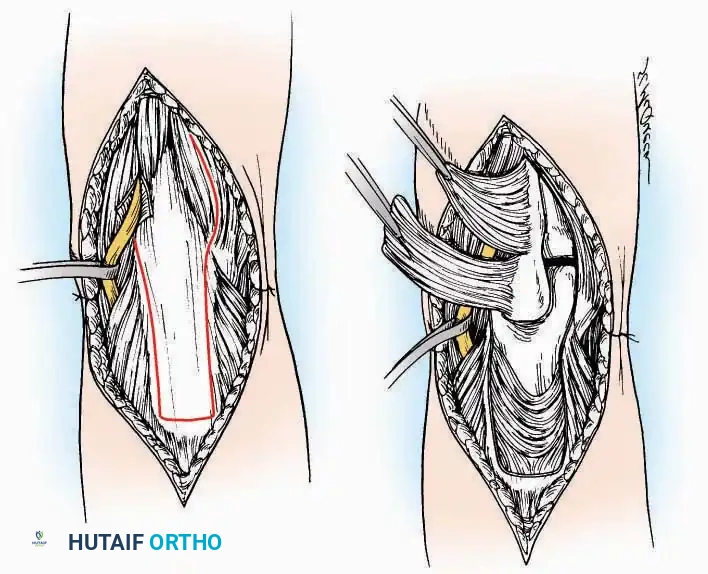
Anterolateral Approach
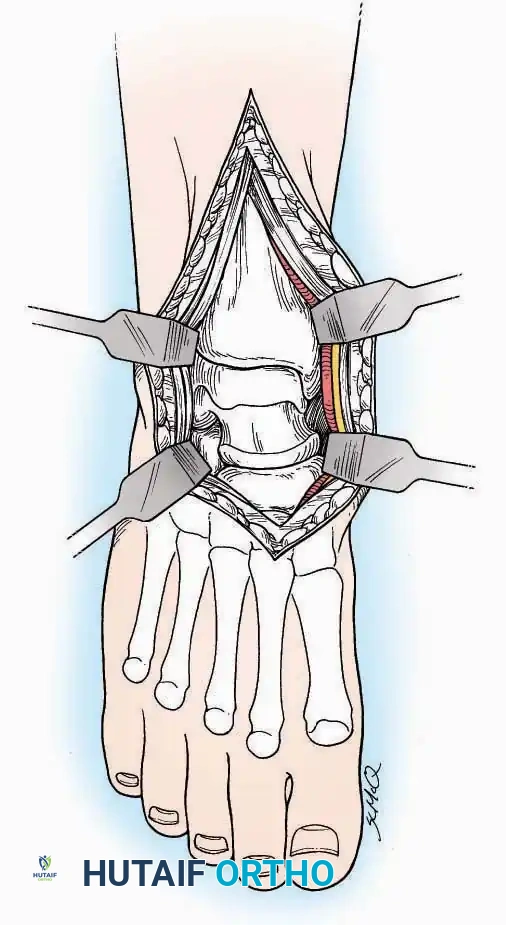
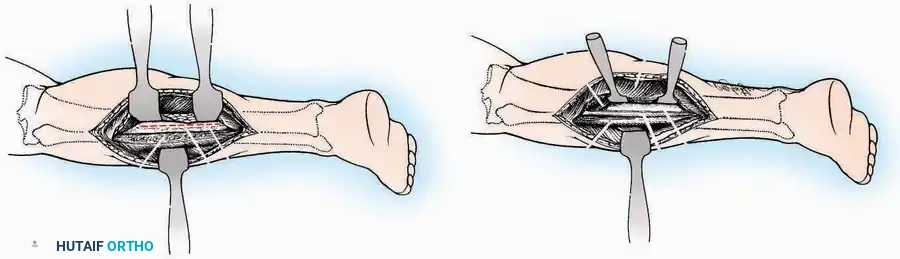
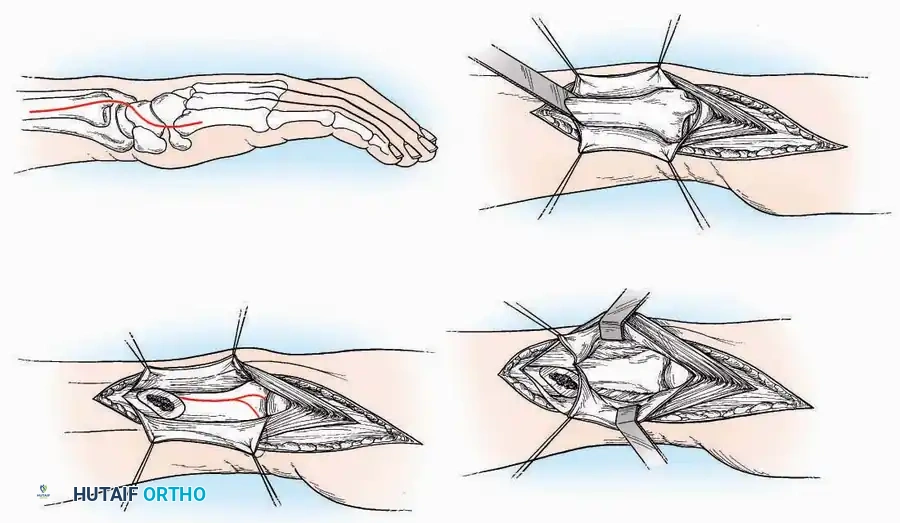
The anterolateral approach is widely considered the "universal incision" for the foot and ankle. It provides unparalleled access to the ankle joint, the talus, and the majority of the tarsal articulations, while safely avoiding the major anterior neurovascular bundle. The only tarsal joints inaccessible via this route are the naviculocuneiform joints (specifically the medial and intermediate).
Indications: Total talectomy, triple arthrodesis, ankle arthrodesis, and open reduction of complex talar neck fractures.
Surgical Technique:
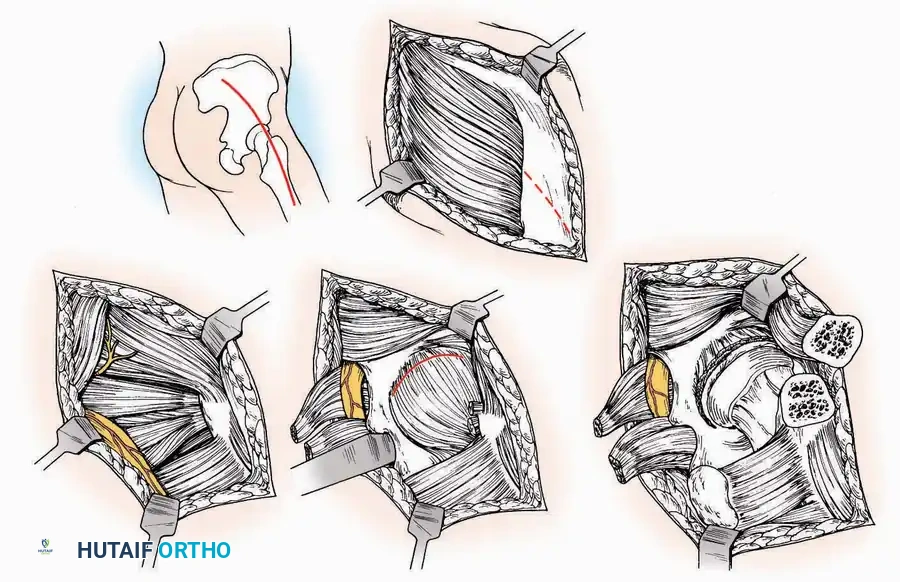
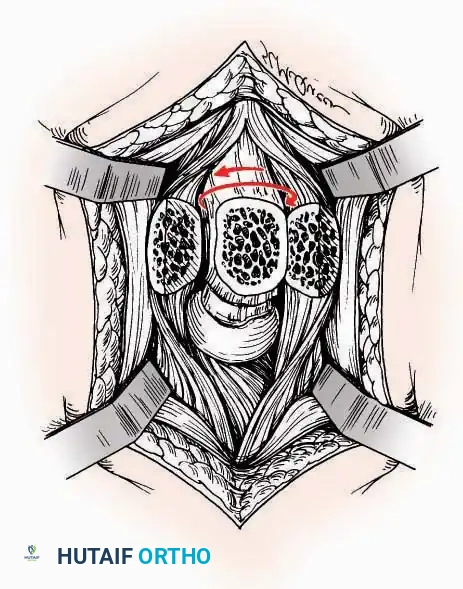
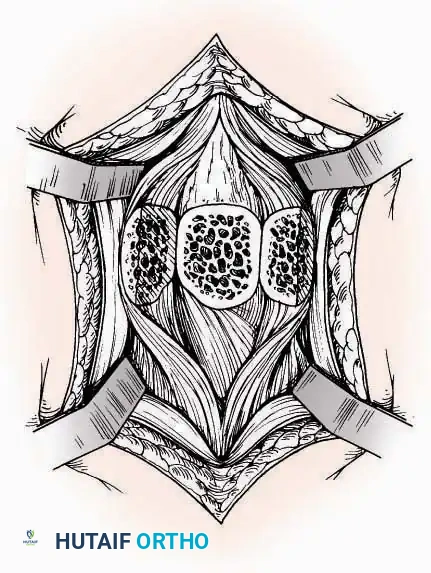
* Incision: Begin over the anterolateral aspect of the leg, medial to the fibula and 5 cm proximal to the ankle joint line. Carry it distally over the joint, crossing the anterolateral aspect of the talar body and the calcaneocuboid joint, terminating at the base of the fourth metatarsal.
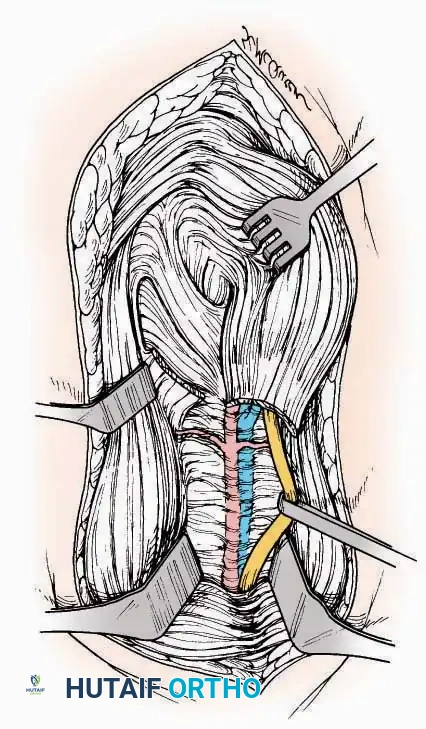
* Superficial Dissection: Incise the superficial fascia and the superior and inferior extensor retinacula down to the periosteum of the tibia and the ankle joint capsule.
* Vascular Ligation: This trajectory usually requires the identification and ligation of the anterolateral malleolar and lateral tarsal arteries.
* Nerve Protection: Retract the skin edges carefully. Identify and protect the intermediate dorsal cutaneous branches of the superficial peroneal nerve (SPN), which frequently cross the distal aspect of this incision.
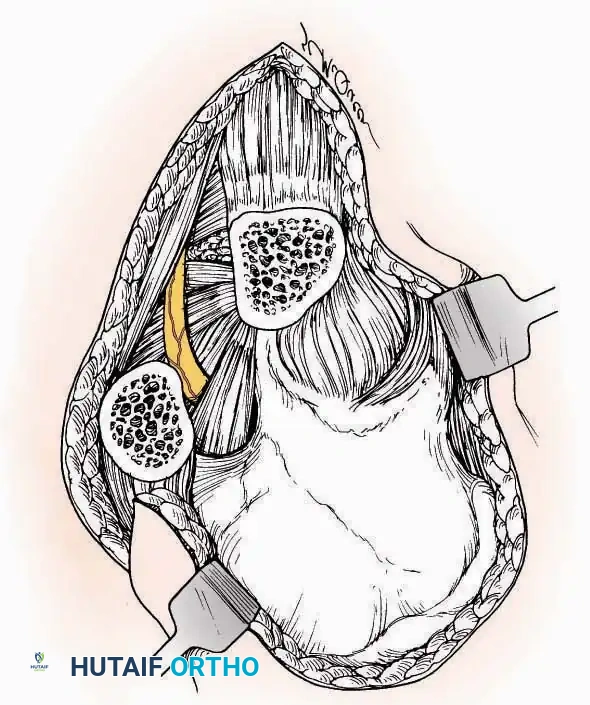
* Muscle Management: Identify the origin of the extensor digitorum brevis (EDB) muscle on the lateral calcaneus. Divide it in the direction of its fibers, or detach its origin entirely and reflect it distally to expose the subtalar and calcaneocuboid joints.
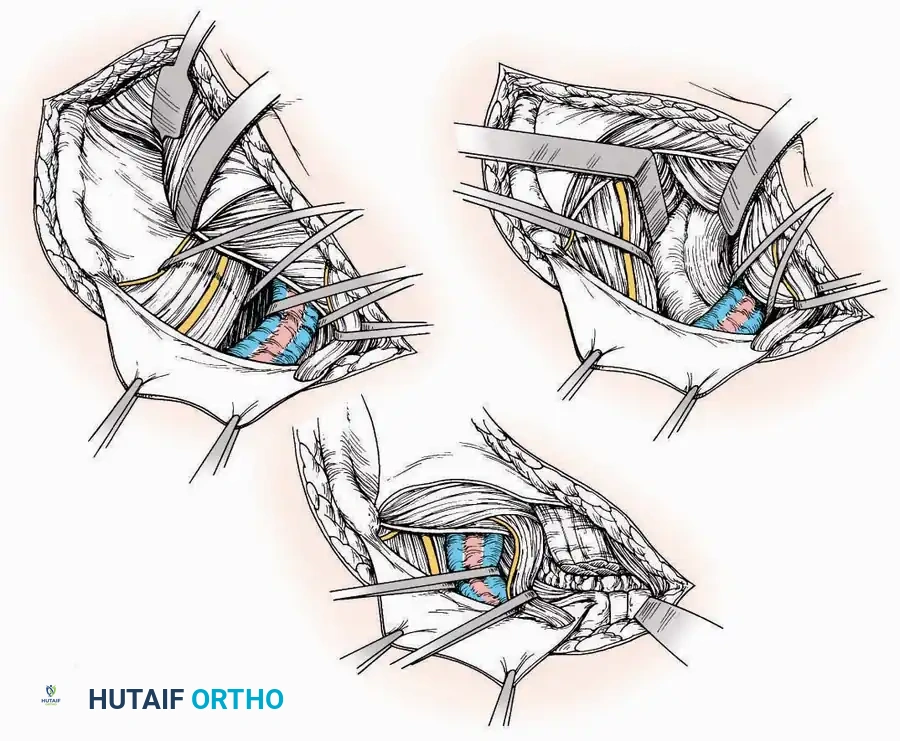
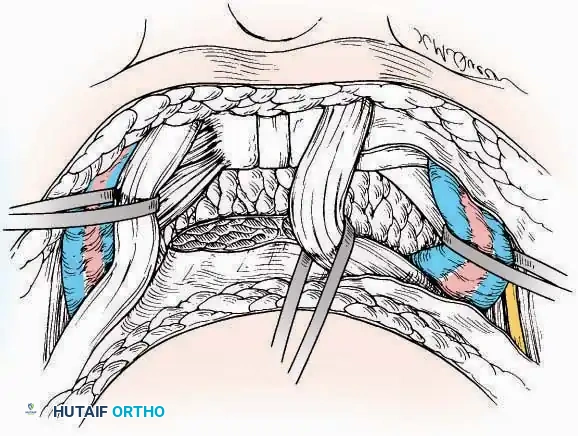
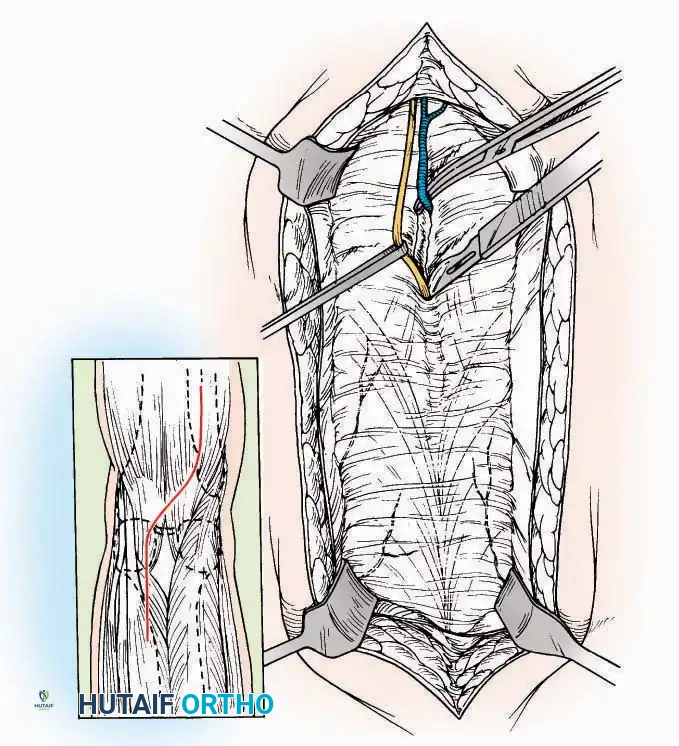
* Deep Exposure: Retract the extensor digitorum longus (EDL) tendons, the dorsalis pedis artery, and the deep peroneal nerve (DPN) medially. Incise the anterior ankle capsule to expose the tibiotalar joint.
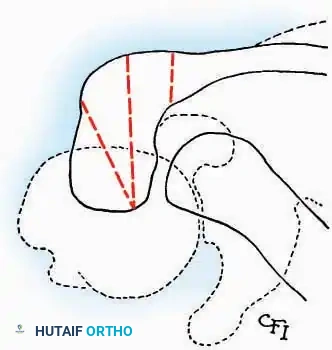
* Tarsal Exposure: Expose the talonavicular joint by dissecting deep to the extensor tendons and incising its capsule transversely. Continue laterally through the capsule of the calcaneocuboid joint. By excising the fat pad within the sinus tarsi (lateral and inferior to the talar neck), the posterior facet of the subtalar joint is brought into direct view.
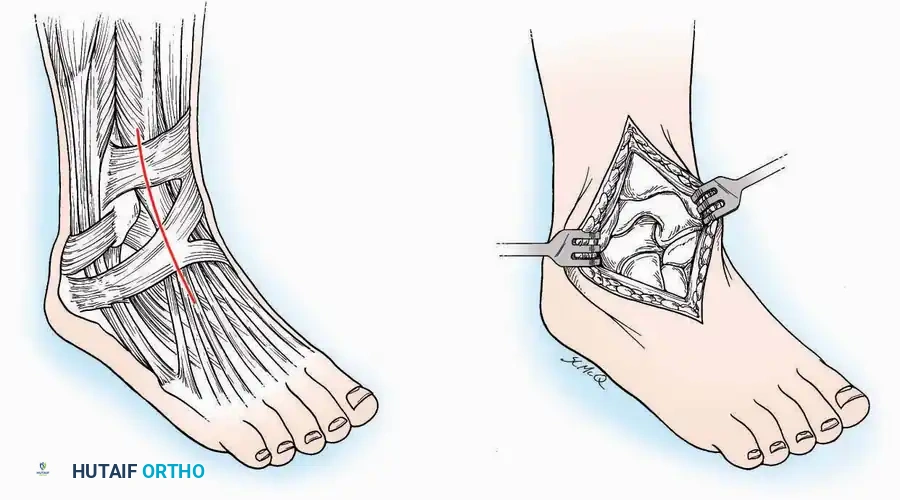
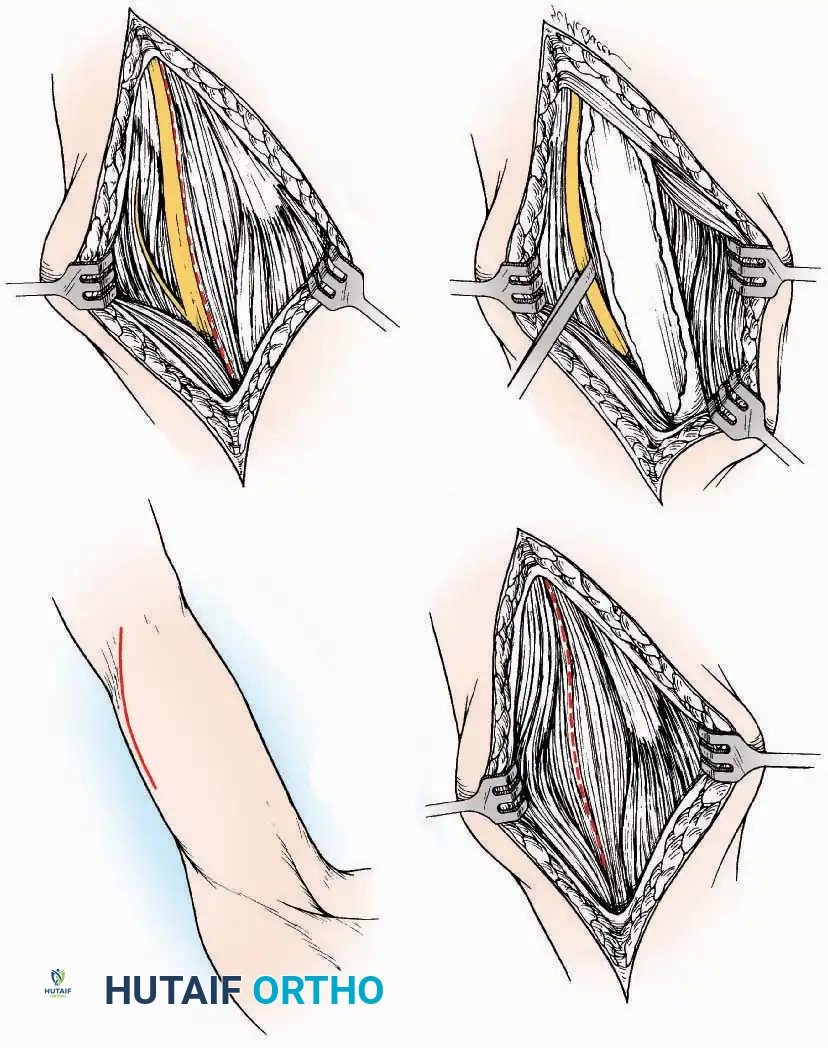
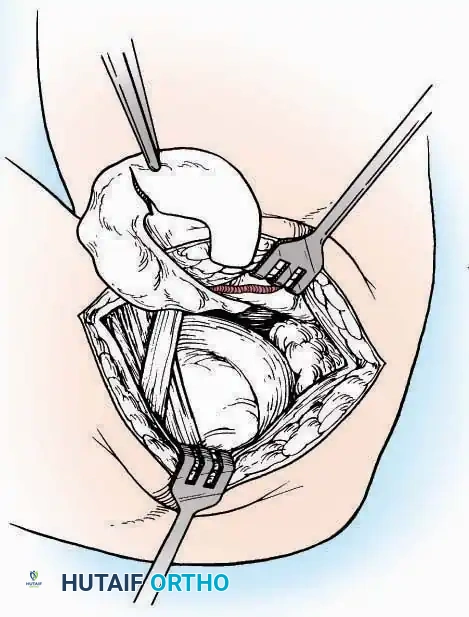
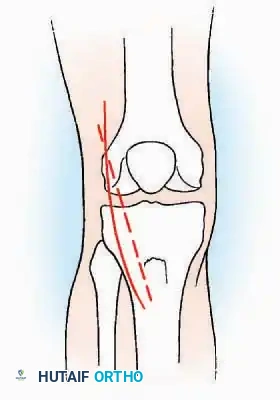
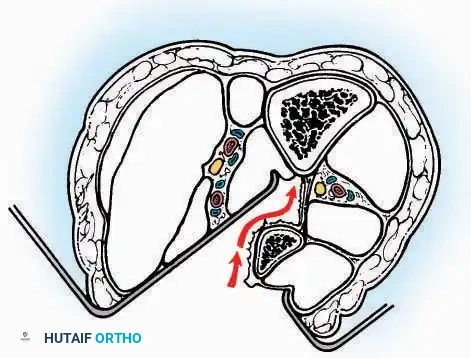
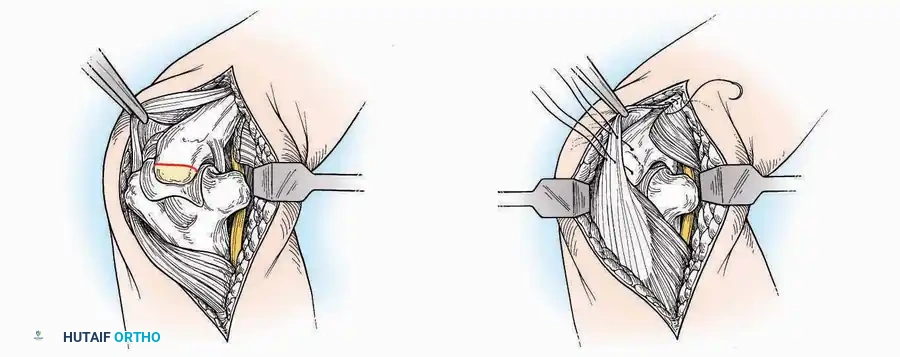
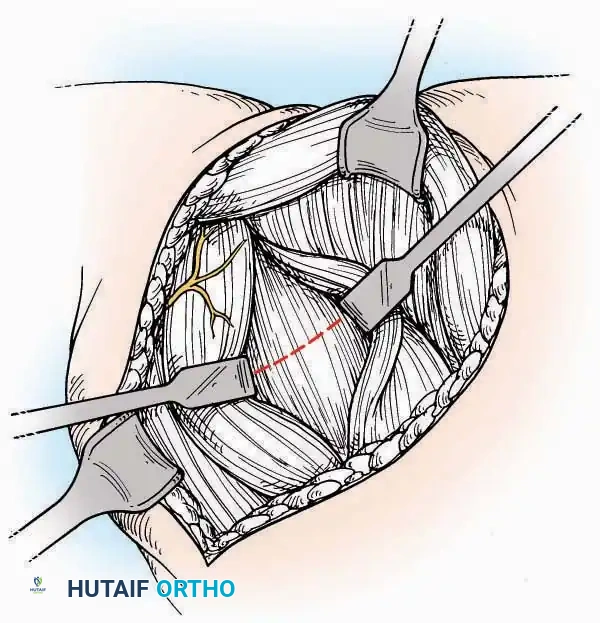
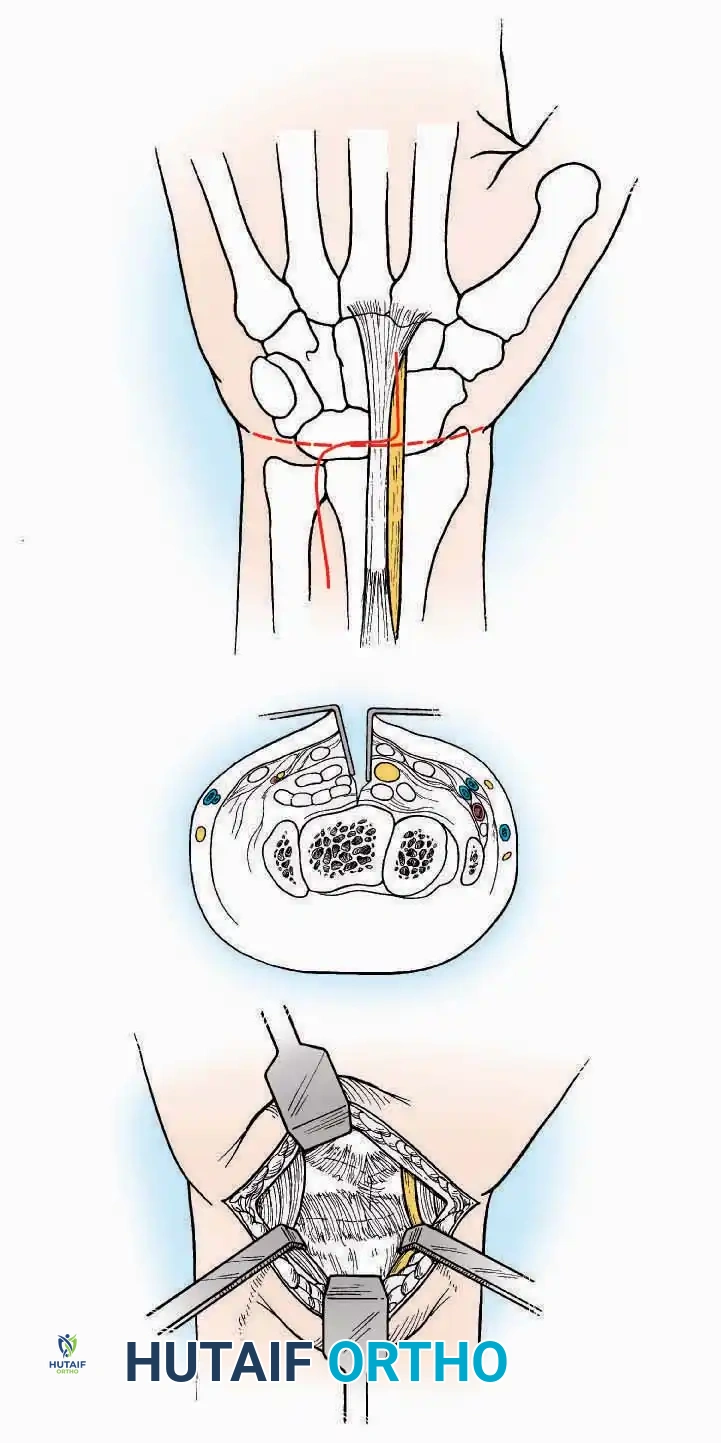
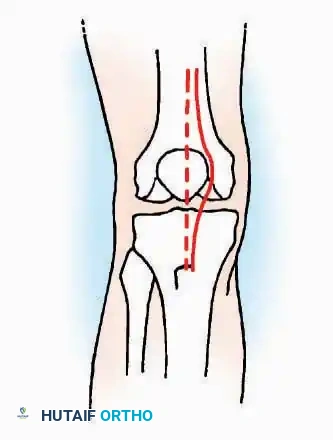
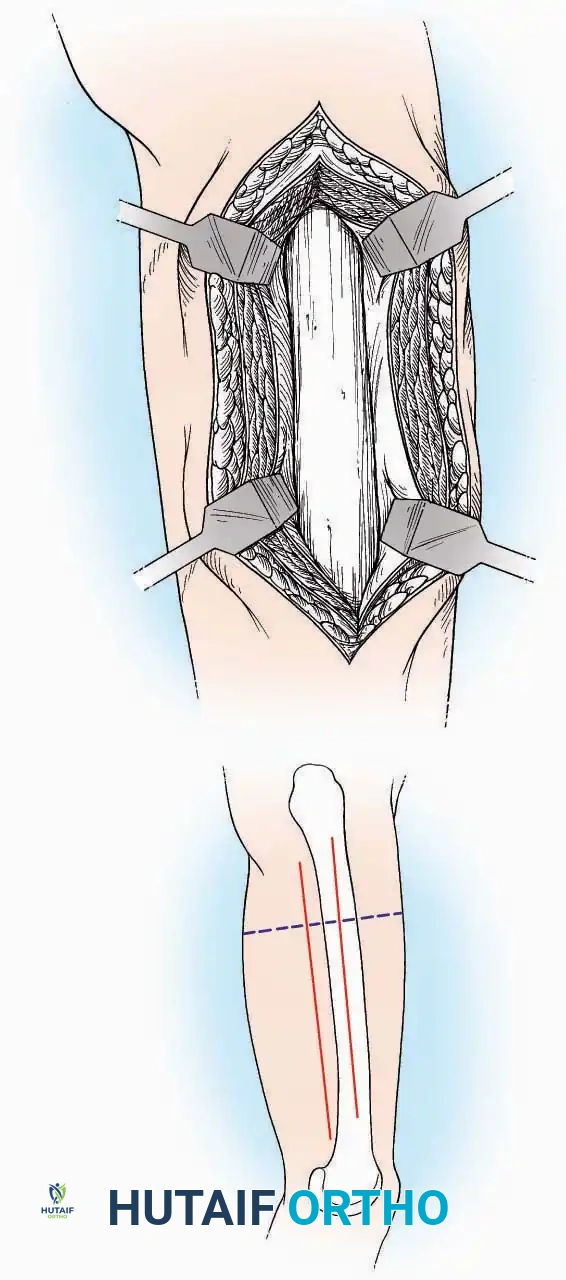
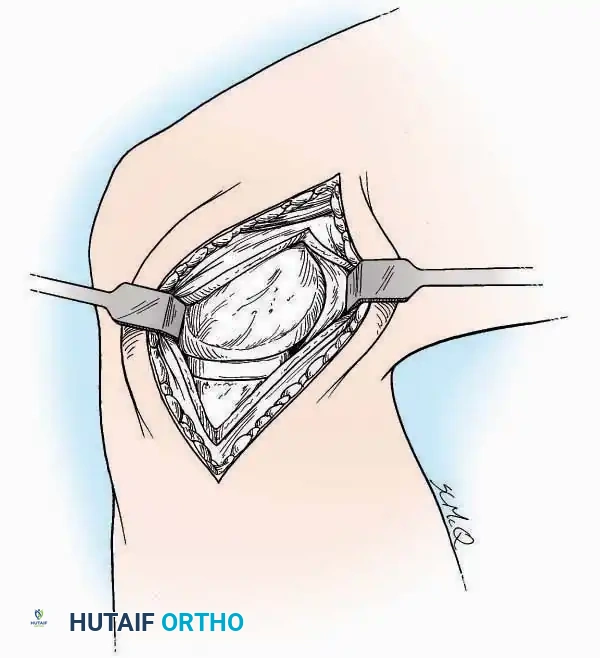
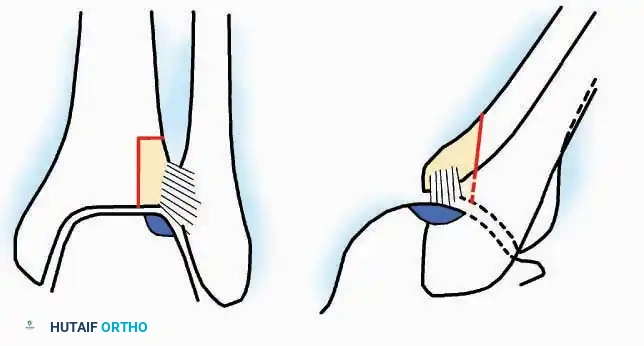
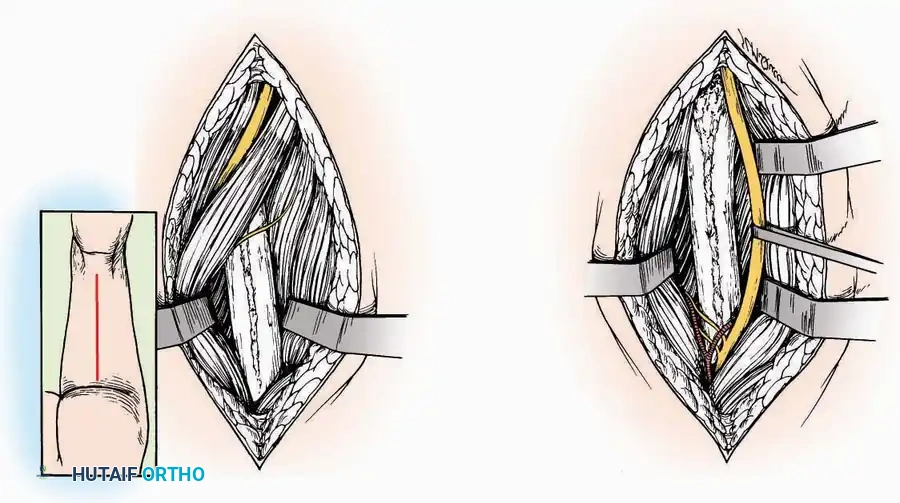
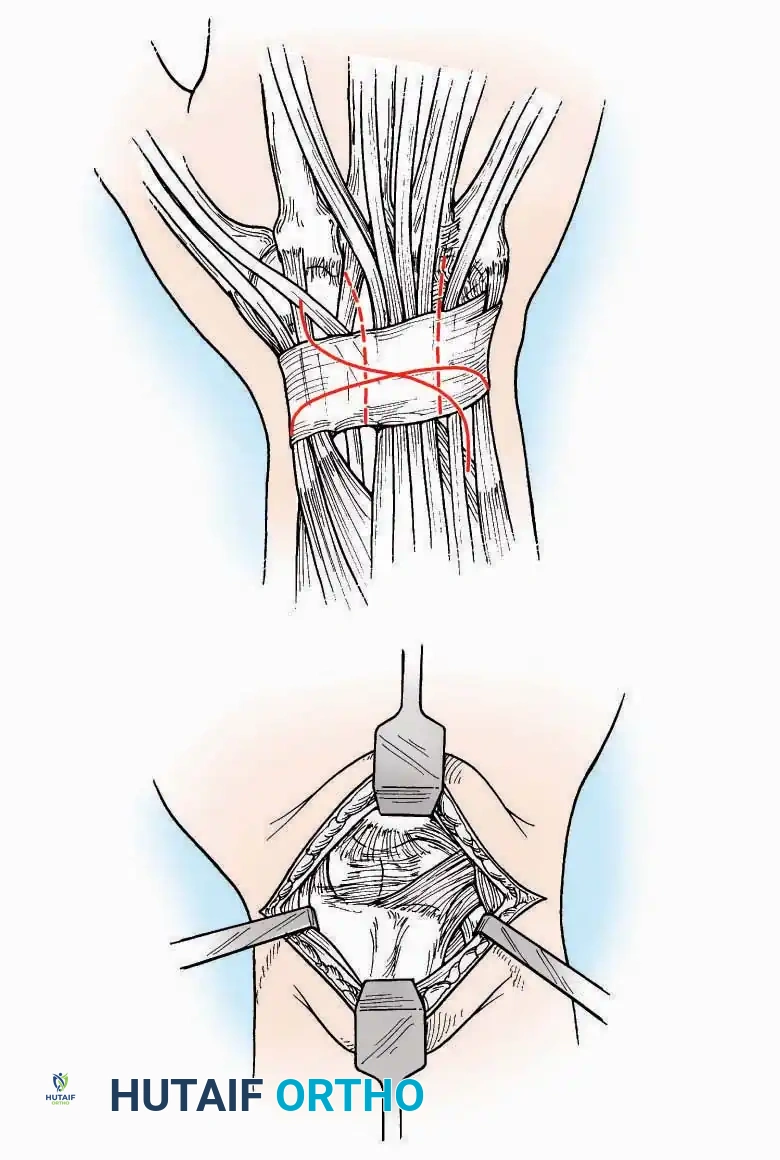
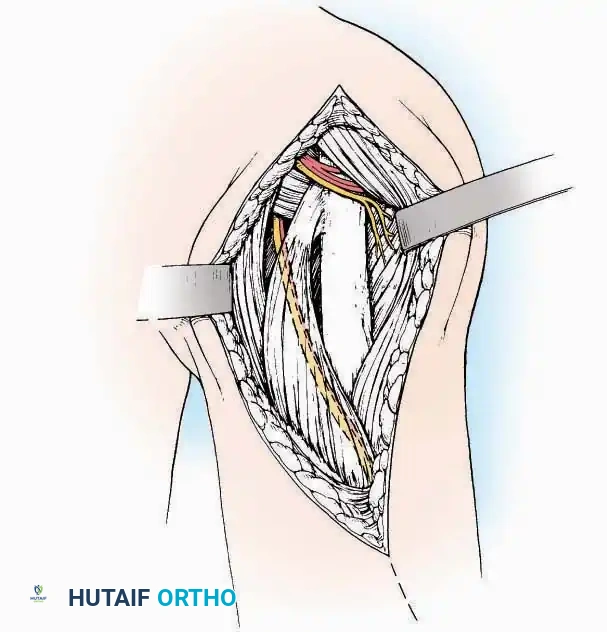
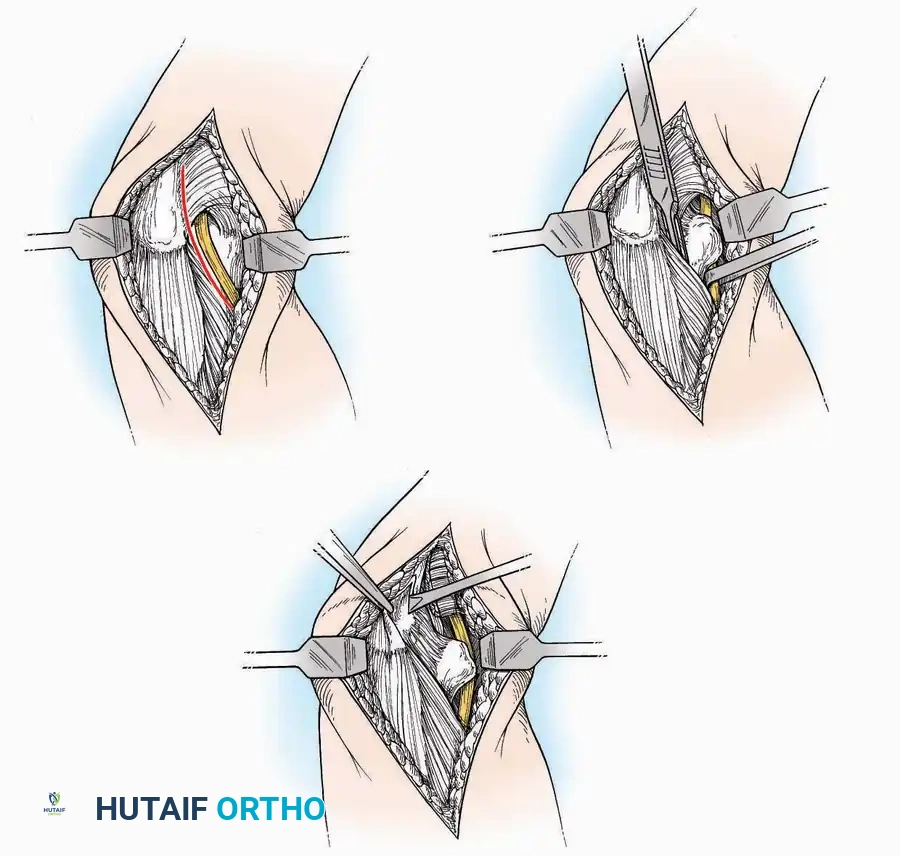
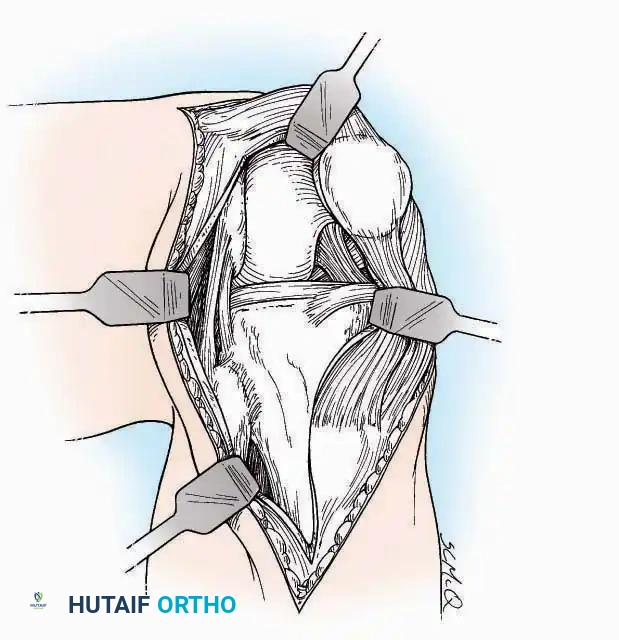
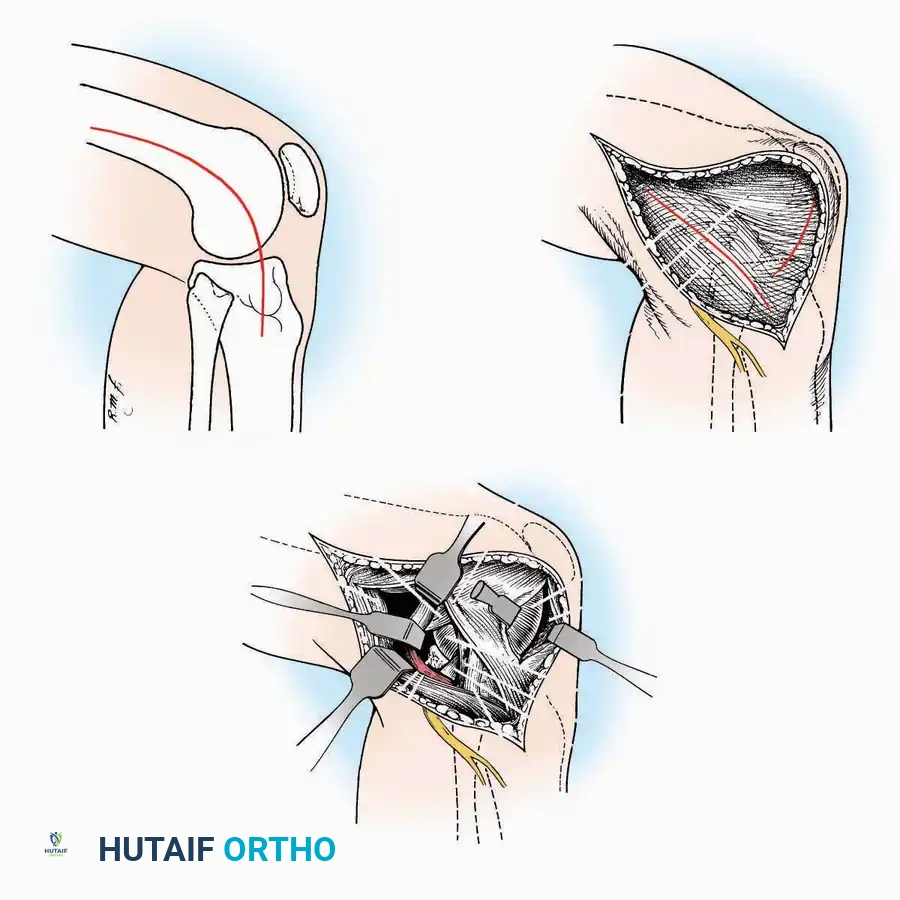
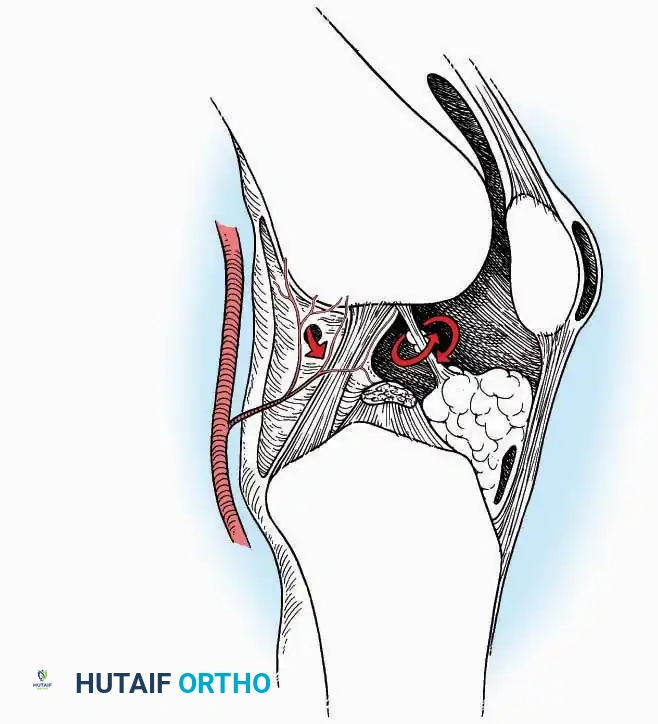
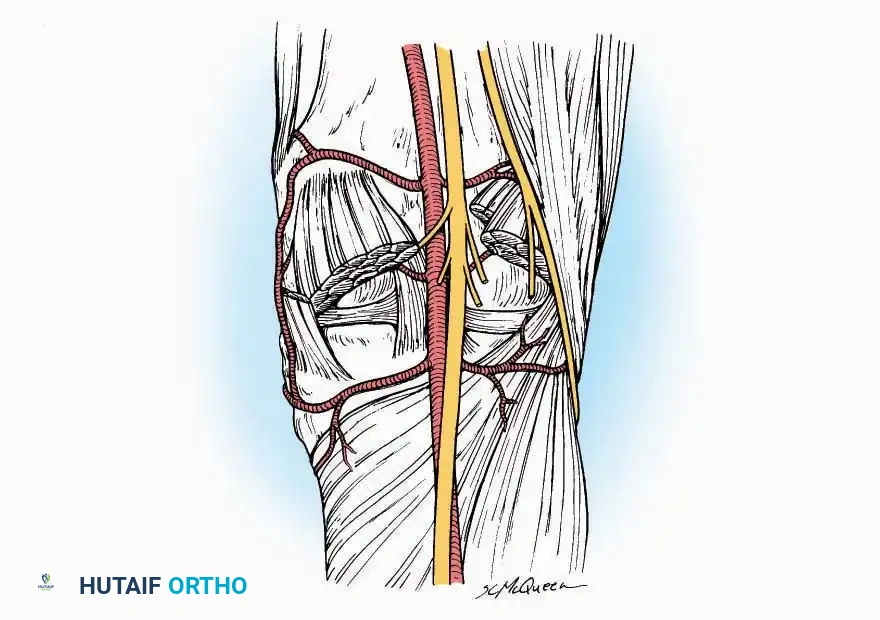
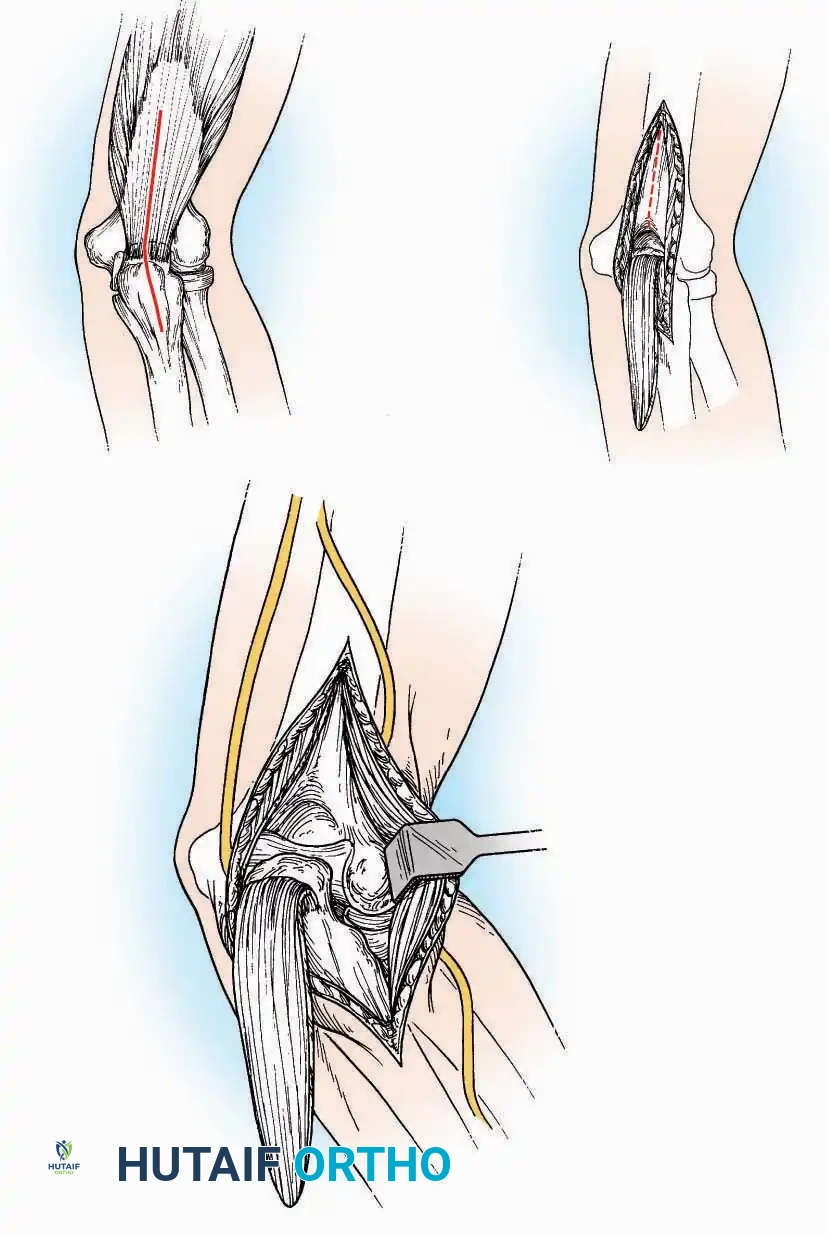
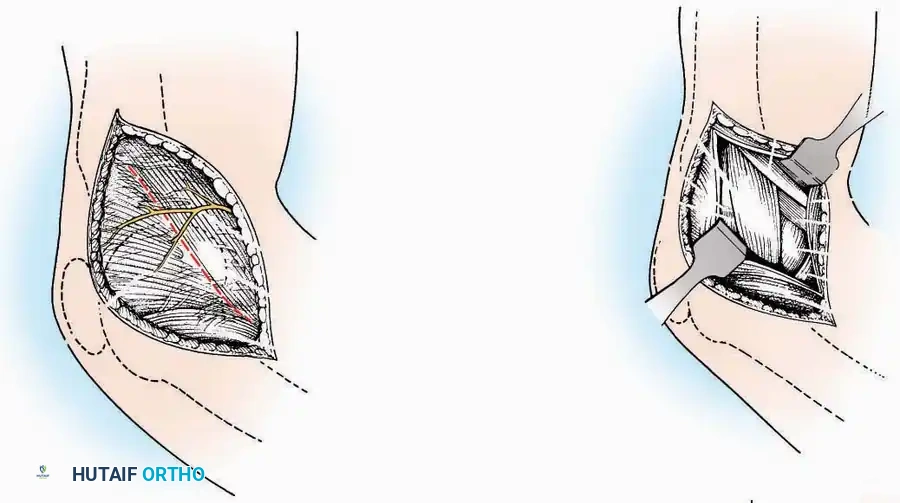
Anterior Approach
Indications: Total ankle arthroplasty (TAA), anterior ankle arthrodesis, and excision of anterior tibial/talar osteophytes (anterior impingement).
💡 Clinical Pearl
Gaining access to the medial gutter (the articulation between the medial malleolus and the medial articular facet of the talus) can be challenging through a pure anterior approach. Meticulous medial subperiosteal dissection of the joint capsule is required to avoid excessive traction on the anterior neurovascular bundle.
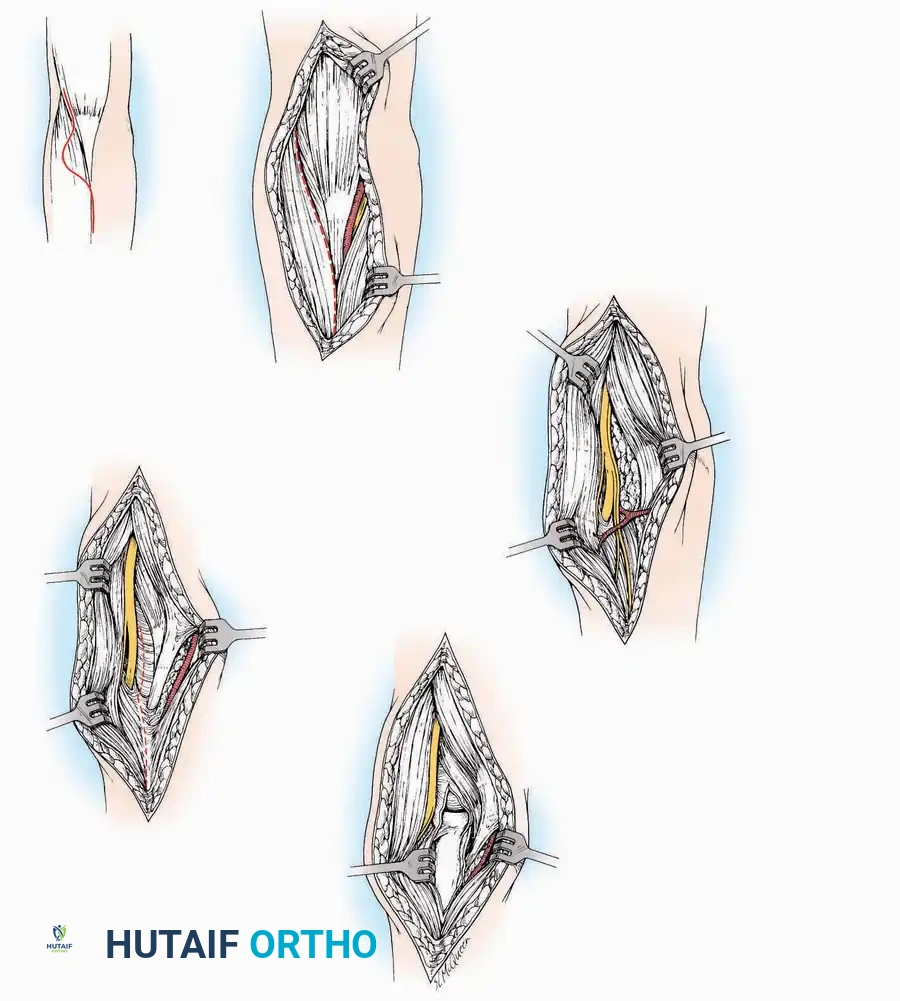
Surgical Technique:
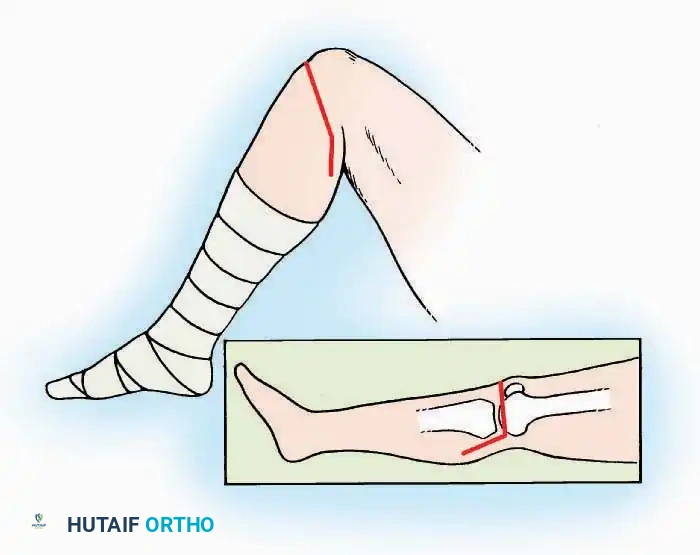
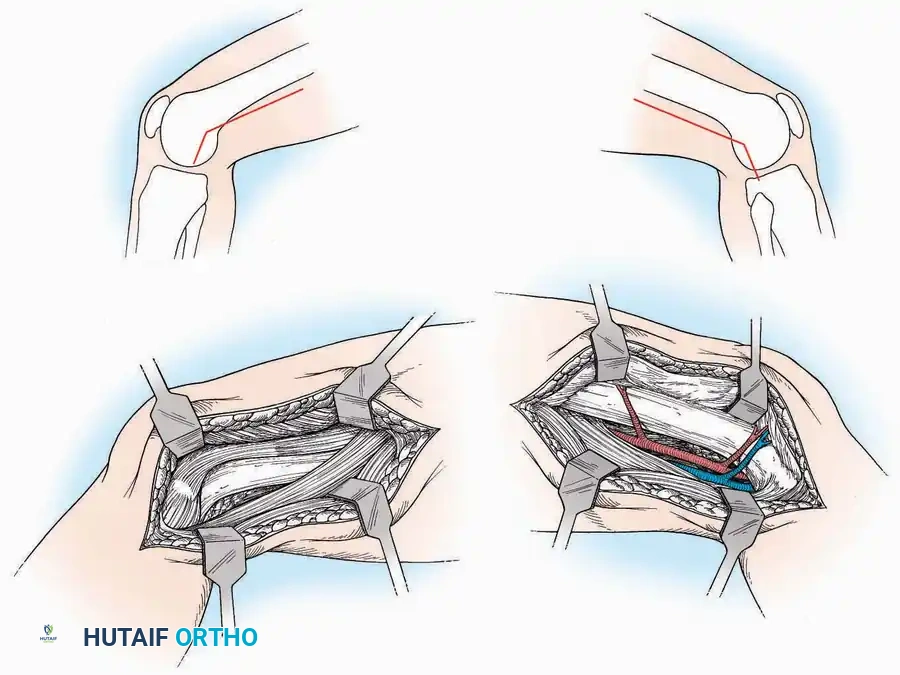
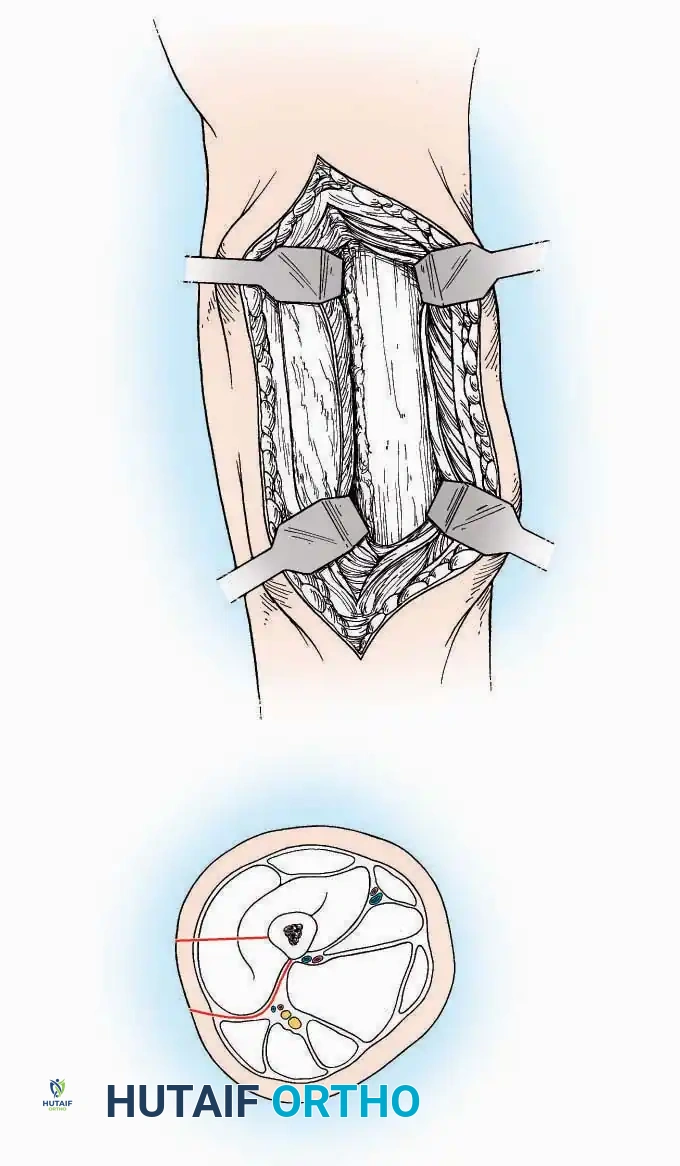
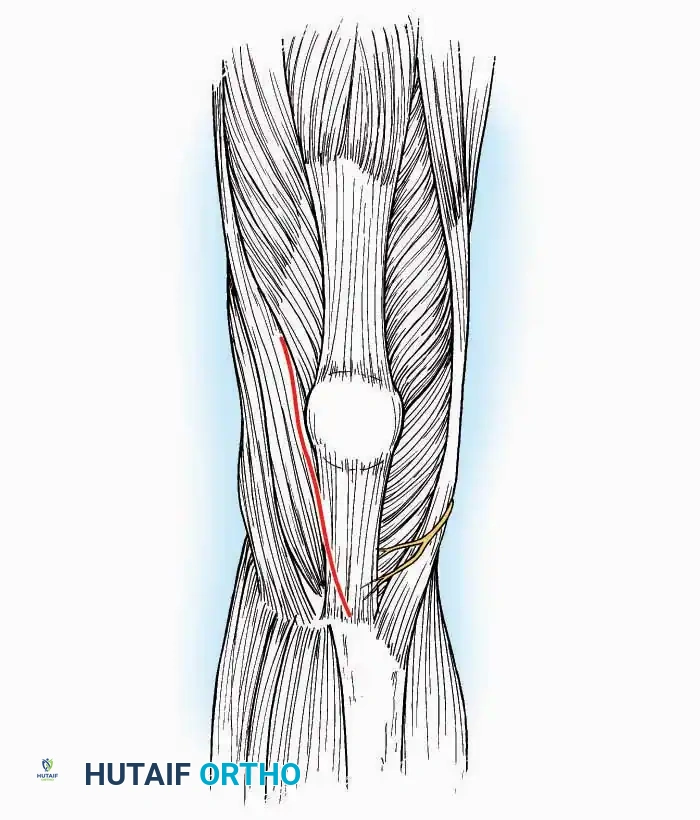
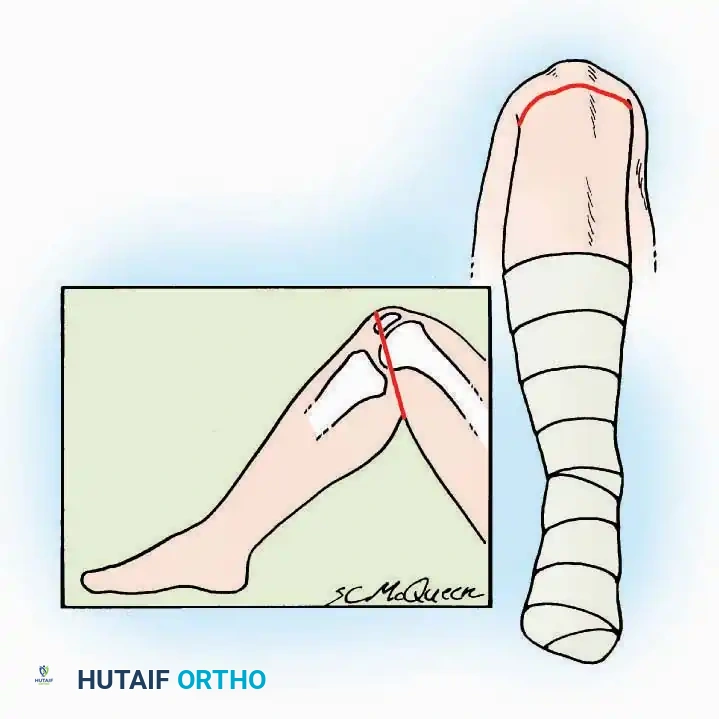
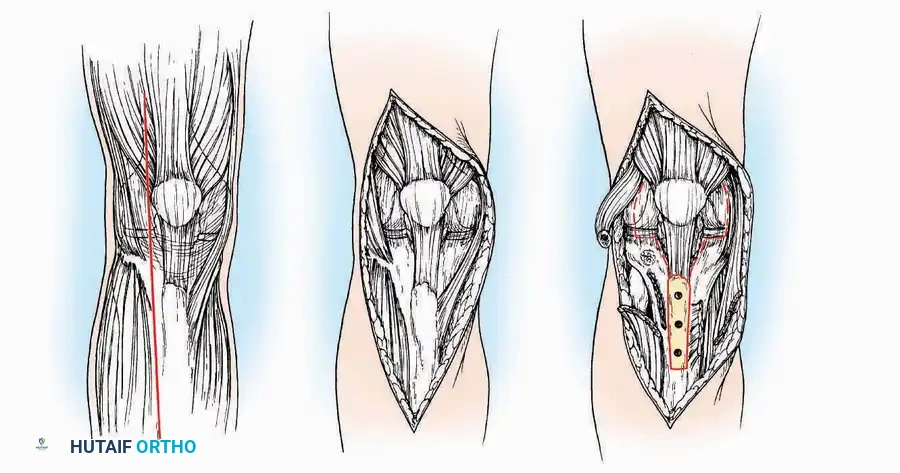
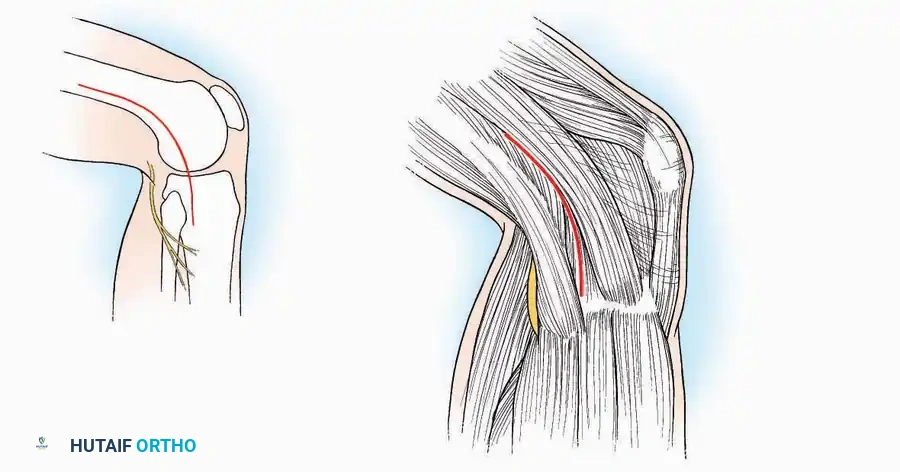
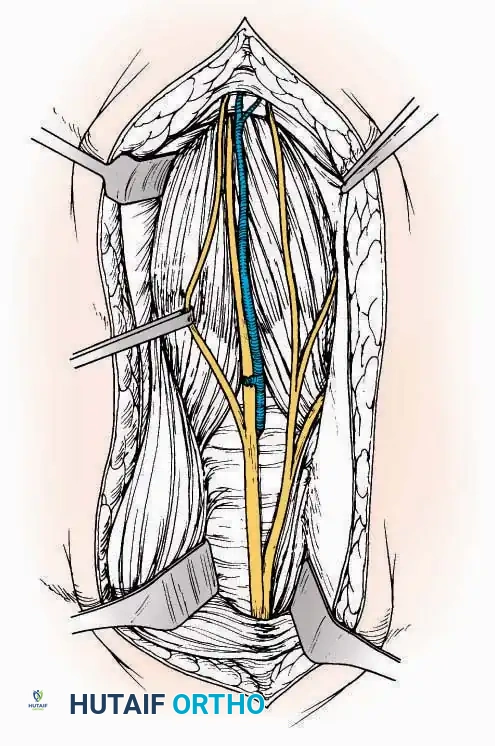
* Incision: Make a 10 to 15 cm longitudinal incision over the anterior aspect of the ankle, centered exactly midway between the medial and lateral malleoli.
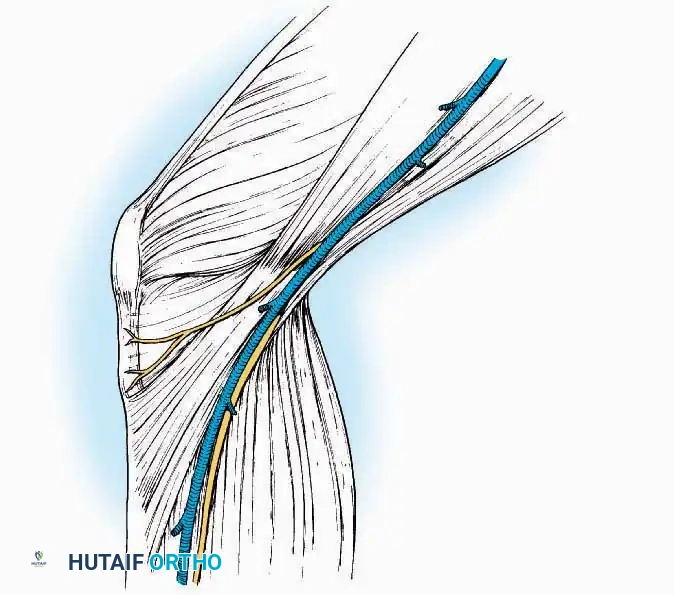
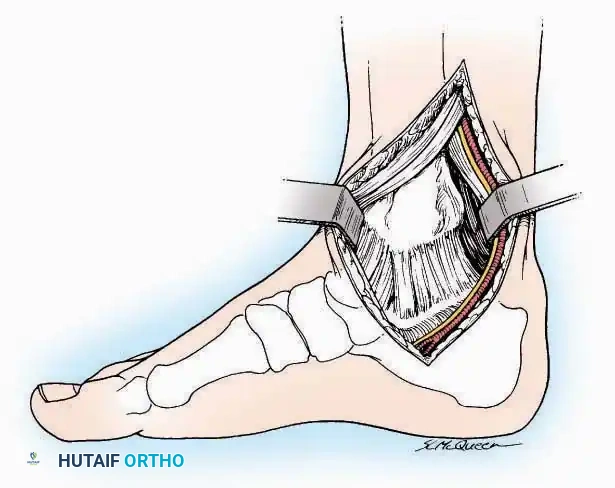
* Superficial Dissection: Incise the superficial fascia. Identify and protect the superficial peroneal nerve branches laterally and the saphenous nerve medially.
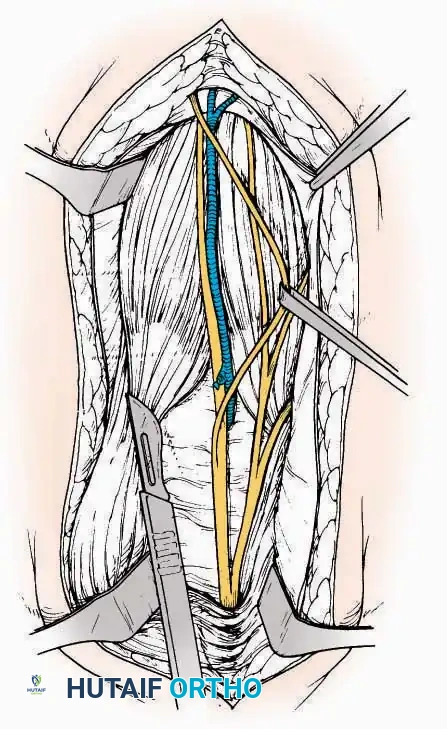
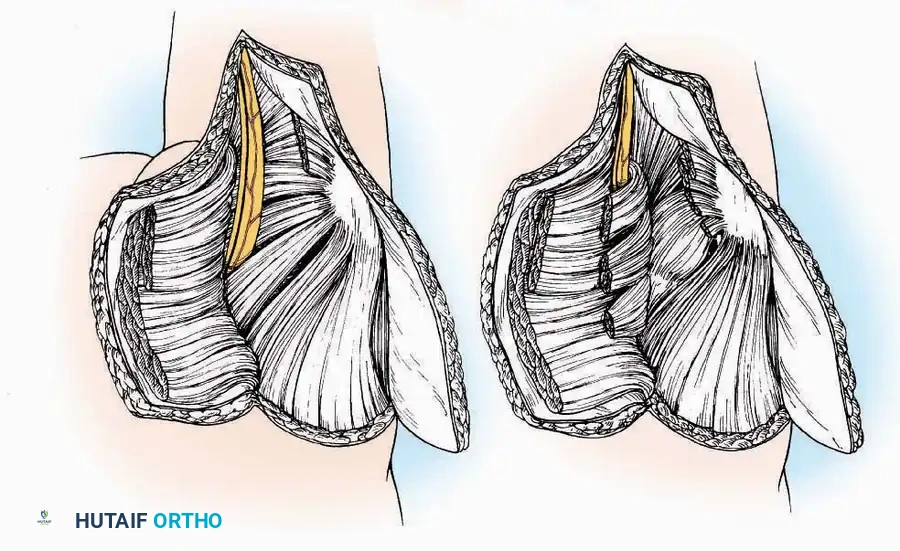
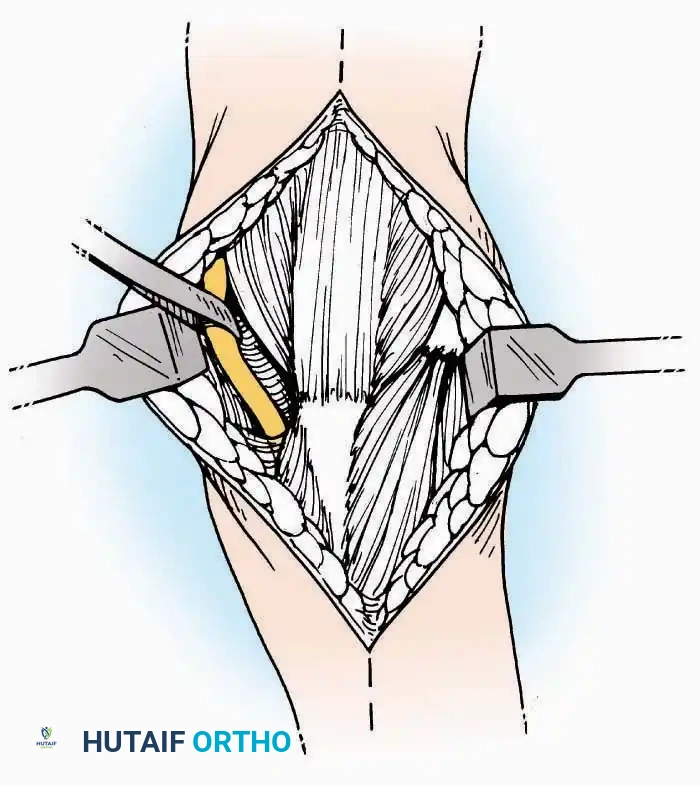
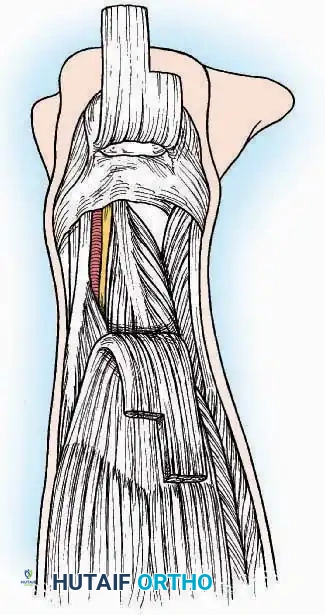
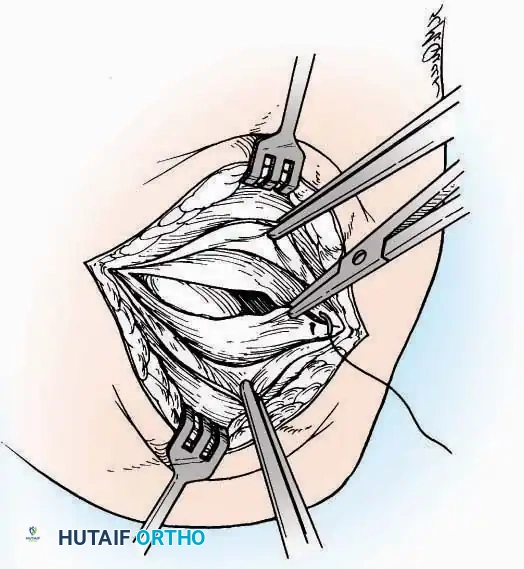
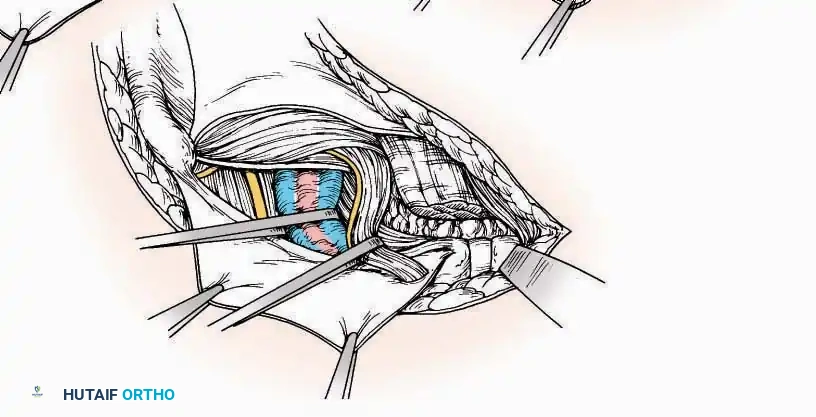
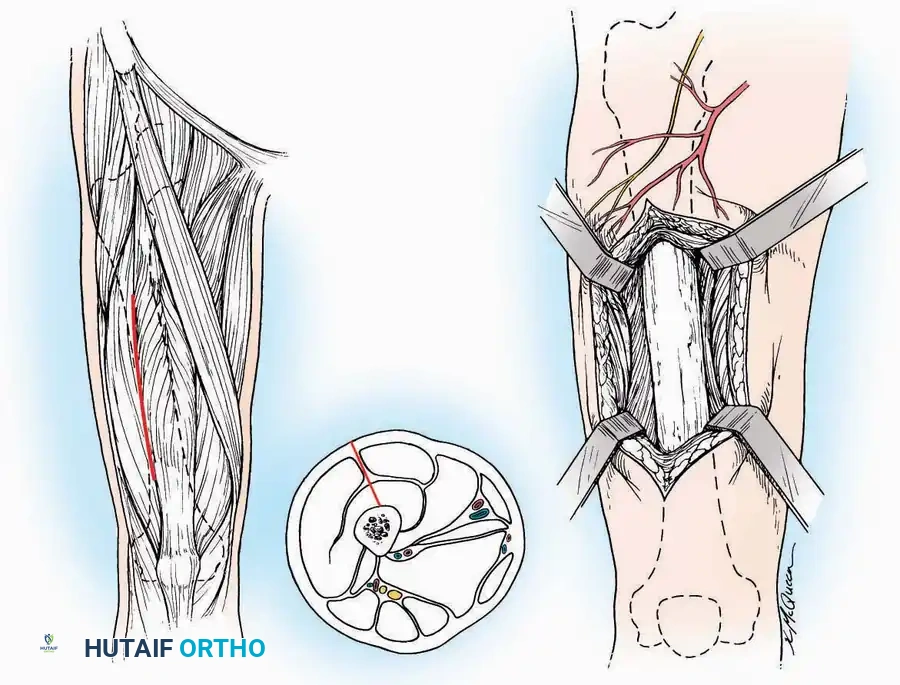
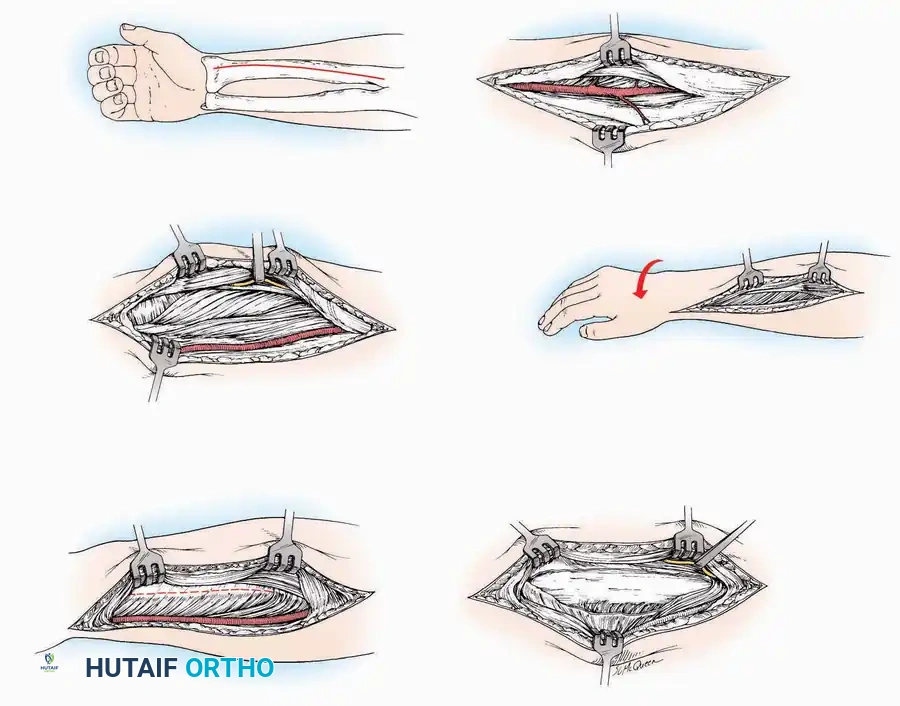
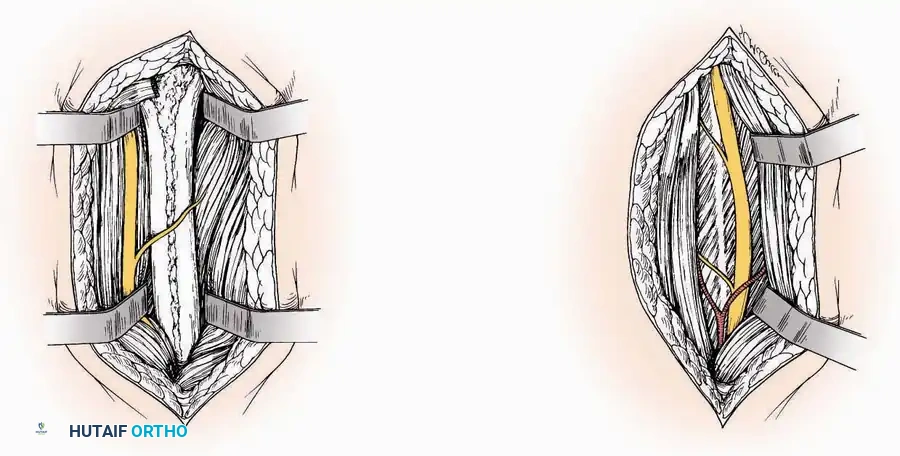
* Internervous Plane: The deep dissection exploits the plane between the Extensor Hallucis Longus (EHL) tendon (innervated by the deep peroneal nerve) and the Extensor Digitorum Longus (EDL) tendons (also innervated by the deep peroneal nerve).
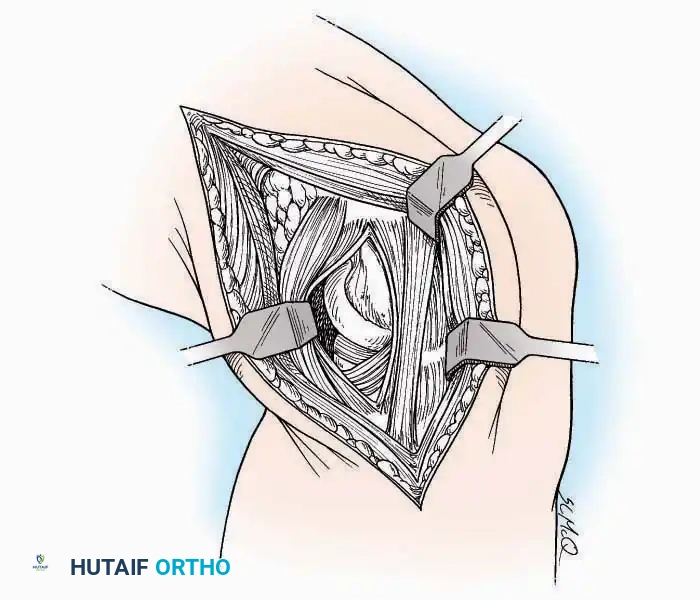
* Neurovascular Bundle: Incise the extensor retinaculum. Carefully identify the anterior tibial artery and the deep peroneal nerve, which typically lie between the EHL and EDL, or directly deep to the EHL. Retract the neurovascular bundle laterally with the EDL, or medially with the EHL, depending on the specific anatomical variant encountered (lateral retraction is most common).
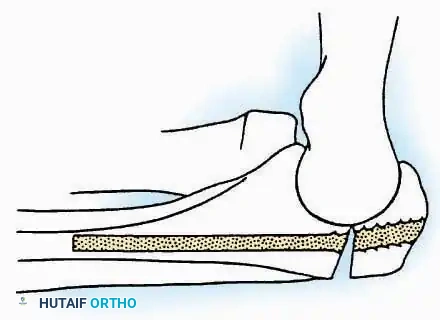
* Capsulotomy: Incise the anterior joint capsule longitudinally. Elevate the capsule subperiosteally from the anterior tibia and the talar neck to expose the entire tibiotalar articulation.
Postoperative Protocol Considerations
Regardless of the approach utilized, meticulous layered closure is mandatory to eliminate dead space and prevent hematoma. The extensor retinaculum should be repaired when possible to prevent tendon bowstringing. Postoperatively, the limb must be immobilized in a bulky, well-padded posterior splint in a neutral position, accompanied by strict elevation to minimize edema and protect the vascularity of the surgical flaps. Suture removal is typically delayed until 14-21 days in foot and ankle surgery due to the tenuous nature of distal extremity perfusion.
Associated Surgical & Radiographic Imaging



You Might Also Like