Open Reduction & Plating of Lesser Metatarsal Fractures
Key Takeaway
Open reduction and internal fixation (ORIF) of lesser metatarsal fractures is indicated for displaced acute fractures or recalcitrant stress fractures. Surgical management requires meticulous soft-tissue handling, precise restoration of the sagittal plane to prevent transfer metatarsalgia, and rigid low-profile plating. This guide details the comprehensive operative approach, including neurovascular protection, fracture site preparation, autologous bone grafting, and postoperative rehabilitation protocols to optimize patient outcomes and minimize hardware complications.
BIOMECHANICS AND PATHOPHYSIOLOGY OF METATARSAL FRACTURES
The metatarsals are the primary weight-bearing conduits of the forefoot, playing an essential role in the biomechanics of the human gait cycle. During the terminal stance and preswing phases of gait, the forefoot is subjected to immense ground reaction forces. The first metatarsal is the most robust, supporting approximately one-third of the total weight-bearing forces transmitted across the forefoot. Consequently, the lesser metatarsals (second through fifth) share the remaining two-thirds of the load.
The second metatarsal is uniquely susceptible to stress fractures (historically termed "march fractures") due to its rigid articulation within the mortise of the cuneiforms at the Lisfranc joint. This rigid proximal fixation, combined with a relatively long lever arm, creates a significant bending moment across the diaphysis. When repetitive submaximal loading outpaces the bone's physiological remodeling capacity, microcracks propagate, leading to a clinical stress fracture. If conservative management fails, or if the fracture progresses to a hypertrophic or atrophic nonunion, surgical intervention via Open Reduction and Internal Fixation (ORIF) becomes necessary.
Acute high-energy fractures of the central metatarsals present a different clinical challenge. These injuries are often associated with severe soft tissue compromise, crush injuries, and multiplanar displacement.
Clinical Pearl: Sagittal plane displacement is the most critical factor in metatarsal fracture outcomes. Even mild plantarflexion or dorsiflexion of the metatarsal head alters the weight-bearing mechanics of the forefoot. Plantar displacement leads to intractable plantar keratosis (IPK) and severe metatarsalgia, while dorsal displacement causes transfer lesions to the adjacent metatarsal heads.
INDICATIONS FOR SURGICAL INTERVENTION
While minimally displaced lesser metatarsal fractures are routinely managed nonoperatively with stiff-soled shoes, walking boots, or elasticized bandages, operative treatment is strictly indicated in the following scenarios:
- Recalcitrant Stress Fractures: Symptomatic nonunions or delayed unions of the lesser metatarsals that have failed prolonged conservative management (immobilization, bone stimulators, orthotics).
- Sagittal Plane Displacement: Any fracture resulting in dorsal or plantar translation/angulation of the metatarsal head.
- Significant Shortening: Shortening greater than 2 to 3 mm disrupts the metatarsal parabola, leading to transfer metatarsalgia.
- Multiple Metatarsal Fractures: "Floating forefoot" injuries where the stabilizing architecture of the foot is lost.
- Intra-articular Extension: Displaced fractures extending into the metatarsophalangeal (MTP) or tarsometatarsal (TMT) joints.
PREOPERATIVE PLANNING AND IMAGING
Standard weight-bearing radiographs (Anteroposterior, Lateral, and Oblique views) are mandatory for evaluating the fracture pattern, degree of displacement, and the overall metatarsal cascade.

Preoperative anteroposterior (AP) radiograph demonstrating a lesser metatarsal fracture requiring operative intervention.

Preoperative oblique radiograph providing a secondary orthogonal view to assess coronal and sagittal plane displacement.
In cases of chronic stress fractures, a CT scan may be utilized to assess the extent of sclerosis, the presence of a fibrous nonunion cleft, and the volume of bone graft that may be required. Advanced imaging is also highly beneficial in high-energy trauma to rule out subtle Lisfranc joint instability.
SURGICAL ANATOMY AND NEUROVASCULAR CONSIDERATIONS
A thorough understanding of the dorsal forefoot anatomy is critical to prevent iatrogenic injury during the surgical approach. The dorsal skin is thin, and the neurovascular structures are superficial.
- Superficial Peroneal Nerve: Divides into the medial dorsal cutaneous nerve and the intermediate dorsal cutaneous nerve. These branches supply the majority of the dorsal forefoot and must be identified and retracted.
- Sural Nerve: Supplies the lateral aspect of the fifth ray and must be protected during approaches to the fifth metatarsal.
- Deep Peroneal Nerve and Dorsalis Pedis Artery: This critical neurovascular bundle courses distally in the first intermetatarsal space, lying just medial to the base of the second metatarsal.
Surgical Warning: When exposing fractures at the base of the second metatarsal, aggressive medial retraction or deep dissection can easily injure the deep peroneal nerve or the dorsalis pedis artery. Meticulous blunt dissection and the use of vessel loops are mandatory in this zone.
SURGICAL TECHNIQUE: OPEN REDUCTION AND PLATING
1. Anesthesia and Positioning
The procedure is performed under regional anesthesia (popliteal block) or general anesthesia. The patient is positioned supine on the operating table. A well-padded calf or ankle tourniquet is applied to ensure a bloodless surgical field, which is vital for identifying the delicate dorsal cutaneous nerves.
2. Surgical Approach and Exposure
Make a longitudinal incision directly over the dorsal aspect of the fractured metatarsal. The length of the incision should allow for adequate exposure of the fracture site and sufficient room for plate application (typically 3 to 5 cm).
Carefully dissect through the subcutaneous tissues. Identify and mobilize the branches of the superficial peroneal nerve (dorsal medial and dorsal intermediate) or the sural nerve (for lateral fractures). Retract these nerves using silastic vessel loops.

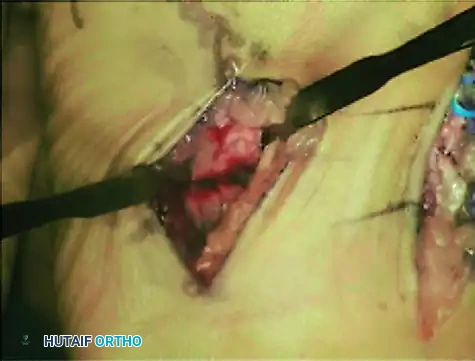
Intraoperative photograph demonstrating curettage and preparation of the second metatarsal. Note the blue vessel loop carefully retracting the dorsalis pedis artery and deep peroneal nerve away from the surgical field.
Incise the extensor retinaculum and retract the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) tendons to expose the underlying periosteum.
3. Fracture Preparation
Gently elevate the periosteum using a Freer elevator to expose the fracture site. In the setting of a chronic stress fracture or nonunion, the fracture gap will often be filled with dense, avascular fibrous tissue.
Use a small curette to meticulously remove all interposed fibrous tissue until healthy, bleeding bone is encountered. To stimulate osteogenesis, prepare and "freshen" the sclerotic fracture ends using a small drill bit (e.g., 1.5 mm or 2.0 mm) to perform multiple osteostixis (drilling) passes into the medullary canal.
4. Bone Grafting
If a significant cortical defect exists after debridement, or if treating an atrophic nonunion, autologous bone grafting is highly recommended. Approximately 3 to 5 cm³ of cancellous bone graft can be harvested from the ipsilateral calcaneus (via a small lateral approach) or the distal tibia. Pack the osteoconductive and osteoinductive graft tightly into the fracture defect prior to final plate fixation.
5. Plate Selection and Application
Select a low-profile small fragment system (typically 2.0 mm or 2.4 mm plates). Because the dorsal soft tissue envelope is extremely thin, bulky implants will lead to postoperative hardware prominence and shoe-wear irritation.
Locking plates are generally not required for diaphyseal metatarsal fractures in young, healthy patients with good bone stock. Standard non-locking cortical screws provide excellent compression and stability.
Intraoperative view of the second metatarsal following the application of a low-profile dorsal plate. Note the flush seating of the plate against the diaphyseal bone.
While the dorsal surfaces of the second and third metatarsals are relatively straight and rarely require plate contouring, the lateral metatarsals present a different anatomical challenge. Fractures of the fourth or fifth metatarsals often require precise plate contouring to match the natural lateral bow of the bone, especially in patients with underlying metatarsus adductus.

Exposure and plating of the fourth metatarsal. Notice the slight contouring of the plate required to accommodate the anatomical curvature of the lateral forefoot.
Reduce the fracture, ensuring absolute restoration of length and sagittal alignment. Temporarily hold the reduction with reduction forceps or smooth Kirschner wires. Apply the plate dorsally. The biomechanical goal is to achieve a minimum of four cortices of purchase (two bicortical screws) on each side of the fracture line.
6. Closure
Once rigid fixation is achieved and confirmed via intraoperative fluoroscopy, irrigate the wound copiously. Attempt to close the periosteum over the plate using fine absorbable sutures (e.g., 4-0 Vicryl) to provide a soft tissue buffer between the hardware and the extensor tendons.
Close the subcutaneous layer, followed by skin closure using 4-0 or 5-0 nylon sutures in a simple interrupted or horizontal mattress fashion.
POSTOPERATIVE CARE AND REHABILITATION
Immediate postoperative care involves placing the patient in a well-padded, bulky sterile dressing supported by a posterior splint or a short-leg cast. The limb should be strictly elevated for the first 48 to 72 hours to mitigate forefoot edema, which can severely compromise wound healing.
- 0 to 2 Weeks: Non-weight-bearing (NWB). Sutures are removed at 10 to 14 days postoperatively, provided the incision is fully epithelialized.
- 2 to 6 Weeks: The patient is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing status is dictated by the surgeon's intraoperative assessment of fracture stability and bone quality. For rigid fixations of acute fractures, progressive heel-touch weight-bearing may be initiated. For stress fractures or grafted nonunions, strict NWB may be extended to 4 to 6 weeks.
- Adjunctive Therapy: For high-risk fractures—such as those at the base of the fourth or fifth metatarsal, or in patients with compromised healing potential (smokers, diabetics, systemic illness)—the use of a pulsing electromagnetic field (PEMF) or low-intensity pulsed ultrasound (LIPUS) bone stimulator is highly recommended to accelerate osteogenesis.

Postoperative anteroposterior radiograph demonstrating anatomic alignment and rigid internal fixation of the lesser metatarsals with low-profile plates and screws.

Postoperative lateral radiograph confirming the restoration of the sagittal plane. The metatarsal heads are perfectly aligned, preventing postoperative transfer metatarsalgia.
COMPLICATIONS AND MANAGEMENT
Prominent Hardware
The most frequent complication following open reduction and dorsal plating of the metatarsals is painful, prominent hardware. The lack of subcutaneous fat over the dorsum of the foot makes shoe wear uncomfortable.
Pitfall: Do not rush to remove hardware. Plate removal should generally not be performed earlier than 12 months postoperatively to ensure complete cortical remodeling. Furthermore, the underlying mechanical issues that contributed to the initial stress fracture (e.g., cavus foot, tight Achilles tendon) must be addressed with orthotics or physical therapy prior to hardware removal.
Nonunion
Nonunion can occur despite adequate surgical fixation. If a nonunion develops, the surgeon must systematically evaluate and treat all contributing factors. This includes aggressive smoking cessation protocols, nutritional optimization (Vitamin D and Calcium levels), modification of improper shoe gear, and the implementation of custom orthotic management to offload the affected ray. Revision surgery may require larger structural grafting and revision plating.
SPECIAL CONSIDERATIONS: ACUTE HIGH-ENERGY METATARSAL FRACTURES
The literature highlights that high-energy fractures of the central metatarsals carry a guarded prognosis. Studies indicate that only approximately 32% of patients obtain a "good" or "excellent" functional result, regardless of whether they are treated operatively or nonoperatively.
The primary factors contributing to poor outcomes in acute trauma include:
1. Severe Soft Tissue Injury: Crush injuries compromise the microvascular supply, increasing the risk of infection, wound dehiscence, and delayed union.
2. Open Fractures: Require immediate aggressive debridement and often necessitate delayed definitive fixation.
3. Sagittal Plane Displacement: As previously emphasized, uncorrected plantarflexion or dorsiflexion of the metatarsal head is poorly tolerated.
While mild coronal (lateral) plane displacement may be functionally tolerated, sagittal plane displacement or excessive shortening inevitably leads to chronic forefoot pain.
For acute, highly displaced central metatarsal fractures, closed reduction and percutaneous pinning (CRPP) with smooth K-wires driven antegrade or retrograde from a dorsal approach is often the first-line recommendation. This minimizes further soft tissue stripping. However, if closed reduction fails to restore the sagittal alignment—assessed intraoperatively by palpating the plantar aspect of the metatarsal heads to ensure they lie in the exact same plane—formal ORIF with plating is absolutely required to restore the functional anatomy of the forefoot.
You Might Also Like
