Management of Neuropathic Foot Ulcers | Operative Orthopaedics

Key Takeaway
Neuropathic foot ulcers require a multidisciplinary approach centered on aggressive local debridement, strict offloading, and optimization of vascular supply. Total contact casting remains the gold standard for localized forefoot and midfoot lesions. Surgical intervention, including the resection of underlying bony prominences and targeted antibiotic therapy, is indicated for deep abscesses, osteomyelitis, or recalcitrant ulcers failing conservative management.
INTRODUCTION TO NEUROPATHIC ULCERS
The management of the neuropathic foot ulcer represents one of the most challenging and critical domains within operative orthopaedics and limb salvage surgery. Primarily affecting patients with long-standing diabetes mellitus, these lesions arise from a complex triad of peripheral sensory neuropathy, foot deformity (often secondary to motor neuropathy and intrinsic muscle wasting), and repetitive microtrauma.
If the ulcer is primarily neurotrophic in etiology—meaning it is driven by the loss of protective sensation rather than primary severe ischemia—the cornerstone of management relies on aggressive local débridement and strict mechanical offloading. The overarching goal is to convert a chronic, non-healing wound into an acute healing wound by removing necrotic tissue, eradicating biofilm, and eliminating the abnormal shear and vertical pressure forces that perpetuate tissue breakdown.
Clinical Pearl: The presence of a neuropathic ulcer is a harbinger of potential limb loss. A localized forefoot ulcer measuring 3 cm or less in diameter, in the presence of palpable pedal pulses or a normal ankle-brachial index (ABI), has an excellent prognosis if treated aggressively with an occlusive healing cast.
CLINICAL EVALUATION AND DIAGNOSTIC PITFALLS
Before initiating any treatment protocol, a comprehensive evaluation of the patient's vascular, neurologic, and musculoskeletal status is mandatory.
Vascular Assessment
Healing potential is directly proportional to tissue perfusion. Palpation of the dorsalis pedis and posterior tibial pulses is the first step. However, in diabetic patients with medial arterial calcification (Mönckeberg's arteriosclerosis), non-invasive vascular studies such as toe-brachial indices (TBI) or transcutaneous oxygen measurements (TcPO2) are required to accurately assess microvascular perfusion. An absolute toe pressure greater than 40 mm Hg or a TcPO2 greater than 30 mm Hg generally indicates sufficient perfusion for wound healing.
Neurologic and Musculoskeletal Assessment
Loss of protective sensation (LOPS) is assessed using a 10-gram Semmes-Weinstein monofilament. Motor neuropathy leads to intrinsic minus foot deformities (claw toes, prominent metatarsal heads), which create focal areas of high plantar pressure.
Diagnostic Pitfalls: Thermal Injuries vs. Gangrene
Patients with profound sensory dysesthesia often resort to dangerous methods to warm their perceived "cold" feet. This can result in severe thermal injuries that mimic ischemic gangrene.
Fig. 82-12: "Gangrenous" changes at the tips of the toes. These were, in fact, deep burns secondary to a "cold" dysesthetic foot being placed too close to a space heater for warmth. These wounds eventually healed with conservative care and do not represent a true example of a Wagner grade 4 ischemic lesion.
Surgical Warning: Always take a meticulous history regarding the use of heating pads, hot water soaks, or space heaters in patients presenting with acute, black, eschar-covered lesions on the digits. Misdiagnosing a thermal burn as dry gangrene can lead to unnecessary and premature amputation.
PRINCIPLES OF NON-OPERATIVE MANAGEMENT: OFFLOADING
The fundamental principle of treating a plantar neuropathic ulcer is the elimination of pressure. While many off-the-shelf products (such as removable cast walkers, half-shoes, and specialized orthotics) are available to unload the diabetic foot, they are universally plagued by a critical flaw: patient non-compliance.
The Total Contact Cast (TCC)
Total contact casts have been unequivocally shown in the literature to be more effective in healing ulcers, and in a shorter timeframe, than removable off-the-shelf products. The TCC works by redistributing plantar pressures over the entire surface area of the foot and transferring load directly to the conical shape of the lower leg, thereby bypassing the ulcerated area.
Indications for TCC:
* Superficial, localized plantar ulcers (Wagner Grade 1 or 2).
* Ulcers $\le$ 3 cm in diameter.
* Adequate vascularity (palpable pulses or TBI > 0.45).
* Even localized osteomyelitis, if confined to a small area of a single bone adjacent to the ulcer, can be successfully managed with cast techniques provided the patient is closely monitored.
Contraindications for TCC:
* Active deep space infection, abscess, or tracking cellulitis.
* Severe peripheral arterial disease (ischemia).
* Profound fluctuating edema.
* Patient non-compliance with follow-up.
TCC Application Technique
- Débridement: The ulcer must be sharply débrided. All surrounding hyperkeratotic tissue (callus) must be removed down to healthy, bleeding tissue. The callus acts as a foreign body, increasing local pressure by up to 30%.
- Wound Dressing: A thin, non-adherent primary dressing is applied to the ulcer bed.
- Padding: Minimal padding is used to ensure "total contact." Felt pads are placed over the malleoli, the tibial crest, and the navicular prominence. Foam padding is placed over the toes to protect them from the hard cast shell.
- Casting: A layer of plaster of Paris is meticulously molded to the contours of the foot, particularly the longitudinal arch, to ensure load sharing. This is followed by a rigid fiberglass outer layer.
- Positioning: The ankle must be held in neutral (90 degrees) during application to prevent equinus contracture, which would paradoxically increase forefoot pressures.
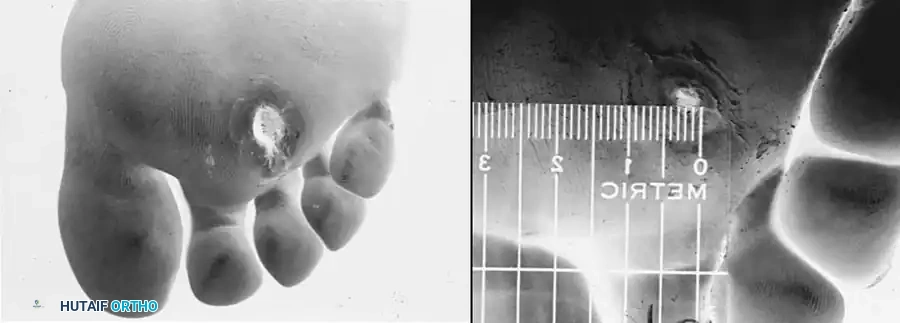
Fig. 82-13: (A) A Grade 2 localized neurotrophic ulcer treated with an occlusive weight-bearing cast after aggressive local débridement. Note the removal of the surrounding callus. (B) The same ulcer demonstrating near-complete closure after 4 weeks of continuous casting. No antibiotics were utilized, as the lesion was localized without surrounding cellulitis.
Weight-Bearing Considerations in Casting
Although having the patient remain strictly non-weight bearing would be the ideal biomechanical scenario to fully off-load the ulcer, the reality is that many patients are unable or unwilling to do so. Fortunately, biomechanical studies have shown that for forefoot and midfoot ulcers, protected weight-bearing in a well-molded total contact cast does not negatively affect ulcer healing, provided the ambulation is not excessive.
Management of Heel Ulcers
Heel ulcers present a distinct and formidable challenge. The heel pad has a unique, specialized fat-chamber anatomy designed for shock absorption; once violated, it is highly prone to avascular necrosis and chronic infection. Furthermore, the calcaneus is superficial, making osteomyelitis a rapid complication.
An ulcer on the heel may be massive and may initially appear untreatable by casting techniques. Although the treatment of heel ulcers is statistically not as successful as the treatment of forefoot ulcers—and the healing time is significantly prolonged—an occlusive cast may still be successful if adequate vascularity is present (defined by a palpable or strong Doppler posterior tibial pulse).

Fig. 82-14 A: A large, deep heel ulcer in a diabetic patient. The patient lacked palpable pedal pulses but demonstrated an encouraging ischemic index on non-invasive vascular testing.

Fig. 82-14 B: The same heel ulcer after 4 weeks of strict casting and intermittent local surgical débridement, demonstrating excellent granulation tissue and wound contracture.
Surgical Warning: Unlike forefoot ulcers, weight-bearing ambulation in a cast for a heel ulcer is strongly discouraged. If ambulation is absolutely necessary, it must be markedly limited, and the cast must be modified (e.g., with a Bohler iron or specialized heel-suspension modifications) to completely unweight the posterior calcaneus.
SURGICAL MANAGEMENT: DÉBRIDEMENT AND BONY RESECTION
When conservative offloading fails, or when the ulcer is driven by a rigid, non-reducible bony prominence, surgical intervention is mandated. The goal of surgery is to alter the biomechanics of the foot to permanently remove the internal pressure source.
Indications for Surgery
- Recalcitrant ulcers failing 6 weeks of optimal TCC therapy.
- Deep abscess formation or necrotizing soft tissue infection.
- Clinical or radiographic evidence of progressive osteomyelitis.
- Prominent plantar exostoses (e.g., Charcot midfoot rocker-bottom deformity).
Management of Diabetic Abscesses
Deep space infections in the neuropathic foot can spread rapidly along fascial planes, often with minimal systemic signs of infection due to an impaired neuro-inflammatory response.
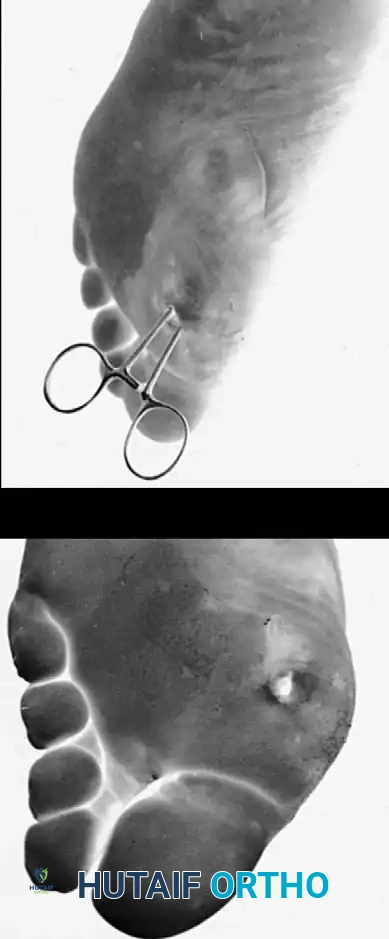
Fig. 82-11: Diabetic abscess. (A) Note the subtle discoloration and swelling proximal to the primary ulceration beneath the first metatarsal head, indicating deep tracking of the infection. (B) Intraoperative view demonstrating the remarkable depth of the abscess cavity, requiring extensive surgical exploration and débridement.
Surgical Approach to Deep Abscesses:
1. Positioning: The patient is positioned supine. A thigh tourniquet is applied but inflated only if necessary, as ischemic preconditioning is poor in these patients.
2. Incision: Generous incisions are made, often incorporating the ulcer itself. Plantar incisions should be placed parallel to the weight-bearing axis or in non-weight-bearing zones when possible.
3. Débridement: All necrotic fascia, tendon, and infected bone must be radically excised. "When in doubt, cut it out." The margins of resection must extend to healthy, bleeding tissue.
4. Irrigation: High-volume, low-pressure pulsatile lavage is utilized.
5. Closure: These wounds are never closed primarily. They are packed open or managed with Negative Pressure Wound Therapy (NPWT) to encourage secondary intention healing or to prepare the bed for delayed primary closure or skin grafting.
Prophylactic and Curative Exostectomy
Removal of bony prominences followed by casting is frequently required to achieve long-term ulcer resolution.
* Metatarsal Head Resection: For recalcitrant plantar ulcers under the metatarsal heads, a dorsal approach is preferred to resect the offending metatarsal head (often the 3rd or 4th), allowing the plantar ulcer to heal without a surgical incision through the weight-bearing surface.
* Midfoot Exostectomy: In Charcot neuroarthropathy, a massive plantar-medial or plantar-lateral bony prominence often develops. Through a medial or lateral approach, the exostosis is resected flush with the surrounding functional arch.
* Achilles Tendon Lengthening (ATL): A percutaneous triple hemisection (Hoke technique) of the Achilles tendon is a powerful adjunct. By releasing the equinus contracture, forefoot plantar pressures are dramatically reduced, significantly accelerating the healing of forefoot ulcers and reducing recurrence rates.
ANTIBIOTIC THERAPY PROTOCOLS
The use of antibiotics in the management of diabetic neuropathic ulcers requires strict adherence to evidence-based infectious disease principles. A common and dangerous pitfall is the over-prescription of antibiotics for colonized, non-infected ulcers.
Indications for Antibiotic Therapy
Antibiotics may or may not be indicated depending on the clinical presentation.
* Not Indicated: Localized ulcers without clinical signs of cellulitis, abscess, osteomyelitis, or pyarthrosis do not require antibiotic therapy. These wounds will heal in an occlusive weight-bearing cast or with prolonged non-weight bearing, provided adequate vascularity is present.
* Indicated: Antibiotics are strictly indicated if an abscess is drained, if spreading cellulitis is present, or in conjunction with the surgical débridement of an area of osteomyelitis or pyarthrosis.
Clinical Pearl: Even small, contiguous, localized areas of osteomyelitis involving a single bone (e.g., the tip of a distal phalanx) may heal by immobilizing the part, removing shear stress, and utilizing targeted oral antibiotics, avoiding the need for immediate amputation.
Microbiological Considerations and Drug Selection
All clinically infected diabetic foot ulcers should be considered polymicrobial until proven otherwise.
1. Cultures: Superficial swab cultures are useless and merely reflect skin flora colonization. Deep aerobic and anaerobic tissue cultures, or bone biopsies, must be obtained surgically before the initiation of antibiotic treatment.
2. Empiric Therapy: A broad-spectrum intravenous antibiotic regimen is initiated immediately after cultures are obtained. This must cover Gram-positive cocci (including MRSA), Gram-negative rods (including Pseudomonas aeruginosa in severe or water-exposed cases), and strict anaerobes. Common empiric regimens include Vancomycin combined with Piperacillin-Tazobactam or a Carbapenem.
3. Targeted Therapy: Once sensitivities return (typically 48-72 hours), the regimen is de-escalated to narrow-spectrum, appropriate antibiotic choices.
4. Consultation: An infectious disease consultation, if available, is highly recommended to assist with drug dosing, monitoring of renal function, and managing prolonged outpatient parenteral antibiotic therapy (OPAT).
Duration of Therapy
The length of treatment is dictated by the depth of tissue involvement and the adequacy of surgical resection:
* Soft Tissue Infection Only: 1 to 2 weeks of targeted therapy.
* Osteomyelitis (Bone completely resected): 2 to 5 days post-amputation/resection.
* Osteomyelitis (Infected bone retained or marginally resected): 4 to 6 weeks of targeted intravenous or highly bioavailable oral therapy.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Healing the neuropathic ulcer is only the first phase of management; preventing recurrence is a lifelong endeavor. Once the ulcer is fully epithelialized, the skin remains fragile and possesses only a fraction of its original tensile strength.
- Transition Phase: Upon removal of the final total contact cast, the patient is transitioned into a customized removable cast walker or a Charcot Restraint Orthotic Walker (CROW) boot for 2 to 4 weeks to allow the new skin to mature.
- Therapeutic Footwear: The patient must never walk barefoot. Custom-molded, extra-depth diabetic shoes with rigid rocker-bottom soles and plastazote inserts are prescribed. The rocker-bottom sole mechanically substitutes for ankle and metatarsophalangeal joint motion, reducing plantar pressures during the toe-off phase of the gait cycle.
- Surveillance: Routine follow-up every 2 to 3 months is mandatory for callus debridement, nail care, and inspection of footwear for wear patterns. Patient education regarding daily foot inspection remains the most cost-effective tool in preventing future ulceration and subsequent amputation.
📚 Medical References
- Neuropathic foot ulceration in patients with myelodysplasia, J Pediatr Orthop 12:786, 1992.
- Mazur J, Menelaus MB, Dickens DRV, et al: Effi cacy of surgical management for scoliosis in myelomeningocele: correction of deformity and alteration of functional status, J Pediatr Orthop 6:568, 1986.
- Mazur JM, Menelaus MB, Hudson I, et al: Hand function in patients with spina bifi da cystica, J Pediatr Orthop 6:442, 1986.
- Mazur JM, Shurtleff D, Menelaus MB, et al: Orthopaedic management of high-level spina bifi da: early walking compared with early use of a wheelchair, J Bone Joint Surg 71A:56, 1989.
- Mazur JM, Stillwell A, Menelaus M: The signifi cance of spasticity in the upper and lower limbs in myelomeningocele, J Bone Joint Surg 68B:213, 1986.
- McCall RE, Schmidt WT: Clinical experience with the reciprocal gait orthosis in myelodysplasia, J Pediatr Orthop 6:157, 1986.
- McKay DW: McKay hip stabilization in myelomeningocele, Orthop Trans 1:87, 1977.
- McLaughlin TP, Banta JV, Gahm NH, et al: Intraspinal rhizotomy and distal cordectomy in patients with myelomeningocele, J Bone Joint Surg 68A:88, 1986.
- McMaster MJ: Anterior and posterior instrumentation and fusion of thoracolumbar scoliosis due to myelomeningocele, J Bone Joint Surg 69B:20, 1987.
- McMaster MJ: The long-term results of kyphectomy and spinal stabilization in children with myelomeningocele, Spine 13:417, 1988.
- Menelaus M: The orthopaedic management of spina bifi da cystica, 2nd ed, Edinburgh, 1980, Churchill Livingstone. Menelaus MB: Talectomy for equinovarus deformity in arthrogryposis and spina bifi da, J Bone Joint Surg 53B:468, 1971.
- Menelaus MB: Progress in the management of the paralytic hip in myelomeningocele, Orthop Clin North Am 11:17, 1980.
- Menelaus MB: General principles in orthopaedic management. In Broughton NS, Menelaus MB, eds: The orthopaedic management of spina bifi da cystica, 3rd ed, Philadelphia, 1998, Saunders. Menelaus MB: The knee. In Broughton NS, Menelaus MB, eds: The orthopaedic management of spina bifi da cystica, 3rd ed, Philadelphia, 1998, Saunders. Menelaus MB, Broughton NS: Dislocation of the hip in myelomeningocele. The McKay hip stabilization, J Bone Joint Surg 79A:1750, 1997 (letter). Moe JH, Winter RB, Bradford DS, et al: Scoliosis and other spinal deformities, Philadelphia, 1978, Saunders. Molloy MK: The unstable paralytic hip: treatment by combined pelvic and femoral osteotomy and transiliac psoas transfer, J Pediatr Orthop 6:533, 1986.
- Molto FJL, Garrido IM: Retrospective review of L3 myelomeningocele in three age groups: should posterolateral iliopsoas transfer still be indicated to stabilize the hip, J Pediatr Orthop 14B:177, 2005.
- Mustard WT: Iliopsoas transfer for weakness of the hip abductors, J Bone Joint Surg 34A:647, 1952.
- Nicol RO, Menelaus MB: Correction of combined tibial torsion and valgus deformity of the foot, J Bone Joint Surg 65B:641, 1983.
- Noonan KJ, Didelot WP, Lindseth RE: Care of the pediatric foot in myelodysplasia, Foot Ankle Clin 5:281, 2000.
- Ogston A: A new principle of curing club-foot in severe cases in children a few years old, Br Med J 1:1524, 1902.
- Olney BW, Menelaus MB:
You Might Also Like