Operative Management of Onychocryptosis: Nail Fold Reduction
Key Takeaway
Nail fold removal or reduction is a definitive surgical intervention for recalcitrant onychocryptosis. By resecting a wedge of hypertrophic tissue or the lateral nail matrix, surgeons can decompress the nail fold and prevent recurrent impingement. This guide details the Watson-Cheyne wedge resection, soft tissue reduction, and Bartlett procedures, providing step-by-step instructions, anatomical considerations, and postoperative protocols to optimize patient outcomes and minimize recurrence.
INTRODUCTION TO NAIL FOLD REMOVAL AND REDUCTION
Onychocryptosis, commonly known as an ingrown toenail, is a pervasive orthopedic and podiatric condition characterized by the painful impingement of the lateral or medial nail plate into the adjacent periungual skin (the nail fold). When conservative measures—such as proper nail trimming, footwear modification, and cotton-wick elevation—fail, surgical intervention becomes necessary.
Nail fold removal or reduction procedures are designed to definitively resolve the mechanical conflict between the nail plate and the hypertrophic nail fold. These procedures consist of either the removal of the nail fold alongside a small border of normal tissue, or the resection of a wedge of normal tissue, the nail plate, and the lateral nail fold. While some surgeons may have limited initial experience with specific variations of these procedures, they are universally based on sound biomechanical and anatomical reasoning.
Clinical Pearl: Preoperative patient counseling is paramount. The patient must explicitly understand that a part or all of the nail may regrow and could be mildly deformed. Provided this is understood, nail fold reduction remains a highly acceptable and definitive treatment modality.
SURGICAL ANATOMY AND BIOMECHANICS
A thorough understanding of the perionychium is essential for successful surgical outcomes. The perionychium consists of the nail bed (sterile matrix and germinal matrix) and the surrounding paronychium (lateral nail folds, eponychium, and hyponychium).
- The Germinal Matrix: Located proximally, extending beneath the eponychium to the lunula. It is responsible for 90% of nail plate generation. Failure to completely excise the lateral horn of the germinal matrix during wedge resection is the primary cause of recurrent nail spicules.
- The Sterile Matrix: Extends from the lunula to the hyponychium. It provides adherence for the nail plate and contributes slightly to nail thickness.
- The Lateral Nail Fold: The soft tissue boundary that often becomes hypertrophic, inflamed, and infected in chronic onychocryptosis.
- Neurovascular Supply: The digital nerves and arteries run plantomedially and plantolaterally. Surgical incisions, particularly in the Bartlett procedure, must be carefully planned to avoid iatrogenic injury to the plantar digital nerve.
PREOPERATIVE PREPARATION
Clinical Evaluation and Microbiology
Patients typically present with pain, erythema, edema, and hypergranulation tissue at the affected nail fold. In cases of chronic or severe onychocryptosis, seropurulent drainage is common.
Surgical Warning: In patients presenting with active seropurulent drainage, it is highly recommended to collect cultures of the material prior to surgery. Staphylococcus aureus is the most common organism identified, though polymicrobial infections involving Gram-negative rods or anaerobes can occur in diabetic or immunocompromised patients.
Anesthesia and Positioning
- Positioning: The patient is placed in the supine position. The foot is prepped and draped in a standard sterile fashion.
- Anesthesia: A digital block is performed using 1% lidocaine or 0.5% bupivacaine. The use of epinephrine is generally avoided in digits with compromised vascularity, though modern literature supports its judicious use in healthy patients to aid hemostasis.
- Hemostasis: A digital tourniquet (e.g., a sterile Penrose drain or a commercial digital ring) is applied to the base of the toe to provide a bloodless surgical field. This is critical for visualizing the subtle color differences between the germinal and sterile matrices.
SURGICAL TECHNIQUE 87-6: WEDGE RESECTION OF NAIL, NAIL BED, AND NAIL FOLD (WATSON-CHEYNE)
The Watson-Cheyne and Burghard technique (also described by O’Donoghue and Mogensen) involves a comprehensive wedge resection that removes the offending nail plate, the underlying matrix, and the hypertrophic nail fold.
Step-by-Step Procedure
- Nail Plate Elevation: Begin by removing the lateral fourth of the nail plate. Use a small, flat dissector (such as a Freer elevator) to lift the nail plate from its underlying bed. Ensure the dissector reaches the most proximal end of the nail root beneath the eponychium.
- Nail Plate Resection: Using straight, heavy tissue scissors or an English anvil nail splitter, longitudinally divide the nail plate and remove the lateral portion.
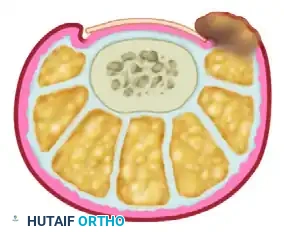
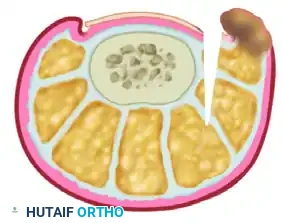
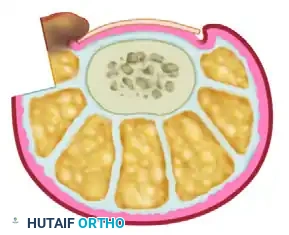
- Primary Incision: With a #15 scalpel blade, make a linear incision parallel to the lateral nail fold. This incision should extend from 1 cm proximal to the lunula down to the distal hyponychium. Carry this incision sharply down to the bone.
- Secondary Incision (Wedge Creation): Begin the second incision 2 to 3 mm lateral to the inner edge of the lateral nail fold. Curve this incision obliquely at a 45-degree angle toward the initial incision to reach the most lateral margin of the germinal matrix.
- Matrix Excision: Exposure and complete removal of this proximal corner of the germinal matrix is the most critical step of the operation.
- Visual Cue: The whitish hue of the germinal matrix usually contrasts sharply with the reddish color of the sterile matrix. This color demarcation helps delineate the lateral border of the entire nail bed.
- Deep Tissue Removal: Remove the periosteum along with the matrix. Expose the fat and subcutaneous tissue in the proximal corner to definitively ensure the complete removal of the germinal matrix. Failure to do so will result in the recurrence of painful nail spicules.

Pitfall: Incomplete excision of the germinal matrix lateral horn is the leading cause of surgical failure. The images below demonstrate the clinical presentation of recurrent nail spicules following an inadequate wedge resection.

- Closure and Dressing: Once the wedge of nail plate, matrix, and nail fold is removed en bloc, the wound is typically left open to heal by secondary intention or loosely approximated. Cover the wound with a nonadherent dressing (e.g., Adaptic or Xeroform) followed by a sterile compression wrap.
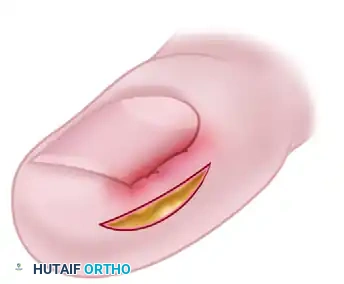
SURGICAL TECHNIQUE 87-7: SOFT TISSUE WEDGE RESECTION (PERSICHETTI ET AL. / CHAPESKIE)
This technique focuses on reducing the soft tissue volume of the nail fold at a distance from the involved nail margin. By closing a laterally based wedge, the hypertrophic nail fold is physically pulled away from the lateral nail border. This allows for free drainage if an infection is present, or reduces the source of mechanical irritation if the part is only inflamed.
Furthermore, it is assumed that with the reduction in the size of the nail wall, unobstructed forward growth of the nail is permitted. By reducing the convexity of the nail fold and displacing it laterally, the nail plate grows over its underlying bed rather than penetrating the lateral fold.
Step-by-Step Procedure
- Preoperative Cultures: As noted, collect cultures of any seropurulent material prior to the surgical prep.
- Incision Marking: Mark an ellipse of skin beginning exactly 4 mm lateral to the nail fold. Maintaining this 4 mm bridge is crucial to ensure the vascular viability of the remaining nail fold.
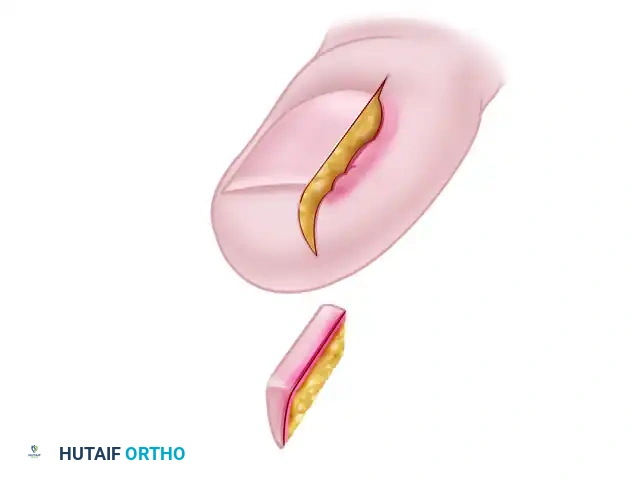
- Debridement: Completely remove the offending lateral nail plate and aggressively debride all associated hypergranulation tissue from the nail groove.
- Wedge Excision: Excise the outlined wedge-shaped ellipse of skin and subcutaneous tissue. The apex of this wedge must reach deep into the subcutaneous fat layer to ensure adequate tissue mobilization.


- Wound Approximation: Approximate the margins of the resulting defect using nonabsorbable sutures (e.g., 3-0 or 4-0 nylon). As the sutures are tied, the nail fold will evert, significantly reducing its convexity.
- Surgical Note: The width of the initial ellipse, and consequently the extent of the final eversion, must be tailored to the size and hypertrophy of the individual patient's nail fold.



- Suture Management: The sutures are left in place longer than standard skin closures to ensure the tissue heals in its new, everted position. Remove the sutures at 10 to 15 days after surgery.
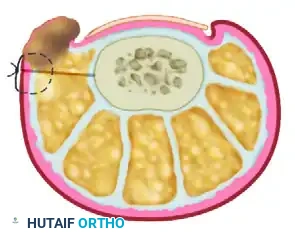
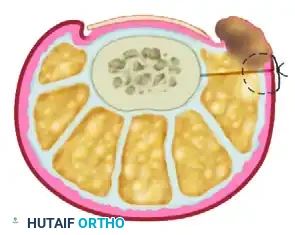
SURGICAL TECHNIQUE 87-8: NAIL FOLD REMOVAL (BARTLETT PROCEDURE)
The Bartlett procedure is a highly effective soft-tissue reduction technique that avoids direct trauma to the nail matrix. Instead, it relies on the excision of a substantial elliptical wedge of tissue from the lateral aspect of the toe to mechanically retract the nail fold away from the nail plate.
Step-by-Step Procedure
- Incision Planning: Begin the marking 4 to 5 mm from the lateral nail margin, near the midlateral line of the digit.
- Wedge Excision: Remove a wedge of tissue through an elliptical skin incision. The widest diameter of the ellipse of tissue should be 4 to 5 mm.
- Crucial Requirement: This incision must be placed in normal, noninflamed, and noninfected tissue to ensure proper healing and suture retention.
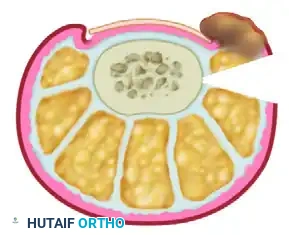
- Depth of Dissection: Take the incision down to the bone, both dorsally and plantarward.
- Anatomical Warning: When the plantar half of the elliptical incision is made, meticulous dissection is required to avoid iatrogenic transection or damage to the plantar digital nerve.
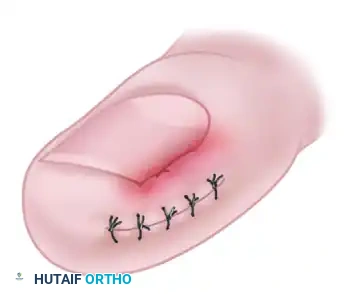
- Wound Closure: Use interrupted nonabsorbable sutures (e.g., 3-0 nylon) to close the defect. As the sutures are tightened, the mechanical force will pull the hypertrophic nail fold away from the nail margin, decompressing the impingement.
- Adjunctive Nail Resection: If necessary, the lateral 2 to 3 mm of the nail edge might be removed after the nail fold is retracted to provide immediate relief, though matrixectomy is not the primary goal of this specific technique.
- Dressing: Apply a sterile, non-adherent compressive dressing.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is critical for preventing infection, minimizing edema, and ensuring optimal wound healing across all nail fold reduction techniques.
Immediate Postoperative Phase (0-48 Hours)
- Elevation: The foot must be strictly elevated above the level of the heart for the first 48 hours after surgery to minimize throbbing pain, edema, and postoperative bleeding.
- Analgesia: Pain is typically managed with over-the-counter NSAIDs or acetaminophen. Severe pain may warrant a short course of prescribed analgesics, though this is rarely necessary if elevation is maintained.
- Dressing Maintenance: The initial bulky compressive dressing should remain intact, clean, and dry.
Subacute Phase (48 Hours to 2 Weeks)
- Dressing Removal: The primary dressing is removed at 48 hours.
- Hydrotherapy: Warm water soaks (often with Epsom salts or dilute povidone-iodine) for 10 to 15 minutes, several times a day, are begun. This helps gently debride exudate, prevents crusting, and promotes secondary intention healing in open wedge resections.
- Topical Care: Following each soak, a topical antibiotic ointment or sterile emollient is applied, and the toe is covered with a simple adhesive bandage.
- Footwear: Patients should wear open-toed shoes or wide-toe-box surgical sandals to prevent mechanical pressure on the healing surgical site.
Suture Removal and Long-Term Follow-Up
- For techniques utilizing primary closure (Persichetti, Bartlett), sutures are removed between 10 to 15 days postoperatively.
- Patients are educated on proper nail trimming techniques (cutting straight across, avoiding aggressive rounding of the corners) to prevent future occurrences of onychocryptosis.
COMPLICATIONS AND PITFALLS
While nail fold reduction procedures are highly successful, complications can arise, primarily due to technical errors during the operation.
- Recurrence of Nail Spicules: As previously highlighted, failure to completely excise the proximal lateral horn of the germinal matrix during a Watson-Cheyne procedure will result in a sharp, painful spicule of nail regrowing into the lateral fold. This often requires revision surgery.
- Infection: Postoperative infections can occur, particularly if preoperative hypergranulation tissue and seropurulent exudate were not adequately managed. Broad-spectrum oral antibiotics may be required if cellulitis develops.
- Nerve Injury: Deep wedge excisions, particularly in the Bartlett procedure, place the plantar digital nerve at risk. Surgeons must maintain a clear surgical field and respect the plantar neurovascular bundle.
- Cosmetic Deformity: Patients must be preoperatively counseled that the nail plate will be permanently narrower, and the lateral nail fold may have a slightly altered contour. Setting appropriate cosmetic expectations is vital for postoperative patient satisfaction.
You Might Also Like

