Medial Calcaneal Displacement Osteotomy: A Comprehensive Surgical Guide
Key Takeaway
Medial calcaneal displacement osteotomy (MCDO) is a powerful joint-sparing procedure for stage II adult-acquired flatfoot deformity. By medializing the calcaneal tuberosity, it realigns the hindfoot mechanical axis and converts the Achilles tendon into a secondary invertor. This reduces strain on the medial soft tissues and augments flexor digitorum longus transfers. MCDO offers predictable union rates and avoids the calcaneocuboid joint overload frequently associated with lateral column lengthening procedures.
INTRODUCTION AND BIOMECHANICAL RATIONALE
Medial calcaneal displacement osteotomy (MCDO) has become a cornerstone in the joint-sparing surgical management of Stage II adult-acquired flatfoot deformity (AAFD), secondary to posterior tibial tendon dysfunction (PTTD). Popularized by Myerson, this extra-articular osteotomy serves as a highly effective alternative—or adjunct—to lateral column lengthening.
The fundamental goal of the MCDO is to fundamentally alter the biomechanical axis of the hindfoot. In a pathologic pes planovalgus foot, the calcaneus drifts into severe valgus, shifting the insertion of the gastrocsoleus complex lateral to the axis of the subtalar joint. Consequently, the Achilles tendon acts as a deforming force, driving the hindfoot into further eversion during the terminal stance phase of gait.
By performing a transverse osteotomy and translating the posterior calcaneal tuberosity medially, the insertion of the Achilles tendon is physically relocated medial to the subtalar joint axis. This profound structural alteration converts the powerful gastrocsoleus complex from an evertor into an invertor of the hindfoot.
Clinical Pearl: The medialization of the calcaneal tuberosity significantly reduces the mechanical demand placed on the transferred flexor digitorum longus (FDL) tendon and the reconstructed medial ligamentous complex (spring ligament). This synergistic effect is critical for long-term construct survivorship.
Using three-dimensional gait analysis, Brodsky et al. demonstrated that posterior tibial tendon reconstruction—consisting of FDL transfer to the navicular, calcaneonavicular ligament reconstruction, and MCDO—produced objective, statistically significant improvements in walking velocity, hindfoot motion, and push-off power. Furthermore, Rosenfeld et al. utilized postoperative MRI to demonstrate compensatory hypertrophy of the transferred FDL muscle belly, correlating with significant improvements in functional scoring.
INDICATIONS AND PATIENT SELECTION
The primary indication for an MCDO is Stage II PTTD, characterized by a flexible hindfoot valgus deformity, medial pain along the posterior tibial tendon, and an inability to perform a single-limb heel rise.


While lateral column lengthening (e.g., Evans osteotomy) is excellent for correcting severe forefoot abduction, MCDO is particularly advantageous in specific clinical scenarios:
* Heavier Patients: The robust cancellous bone of the calcaneal tuberosity heals predictably, making it safer for patients with higher BMI where graft subsidence in an Evans osteotomy might be a risk.
* Mild to Moderate Midfoot Abduction: In patients where standing anteroposterior radiographs do not demonstrate severe talonavicular uncoverage or midfoot abduction, MCDO provides sufficient correction without the need for lateral lengthening.
* Avoidance of Calcaneocuboid Overload: A known complication of lateral column lengthening is increased contact pressures across the calcaneocuboid joint, leading to lateral column pain or iatrogenic arthrosis. MCDO entirely avoids this complication.


SURGICAL TECHNIQUE: MEDIAL CALCANEAL DISPLACEMENT OSTEOTOMY
The procedure is typically performed in a staged manner during the same anesthetic session, beginning with the calcaneal osteotomy in the lateral decubitus position, followed by repositioning to supine for the medial soft tissue reconstruction.
1. Patient Positioning and Preparation
- Position the patient in the lateral decubitus position on a radiolucent bean bag.
- Ensure all bony prominences are meticulously padded.
- Apply a well-padded thigh tourniquet.
- Prepare and drape the entire lower extremity to allow for intraoperative assessment of hindfoot alignment.
2. Surgical Approach
- Make an oblique incision approximately 4 to 5 cm in length on the lateral aspect of the calcaneus.
- The incision should be positioned inferior and parallel to the peroneal tendons, and posterior and inferior to the expected path of the sural nerve.
- Extend the dissection from the superior border of the calcaneus (anterior to the retrocalcaneal space) down to the inferior border of the calcaneus, deep to the plantar fascia.
Surgical Warning: The sural nerve is highly variable in its branching pattern over the lateral calcaneal wall. Meticulous blunt dissection in the subcutaneous tissues is mandatory to avoid painful postoperative neuromas. Retract the peroneal tendons superiorly and anteriorly to protect them during the saw cut.
3. The Osteotomy
- Carry the dissection sharply down to the periosteum.
- Reflect the periosteum locally at the proposed osteotomy site using a periosteal elevator. Use Hohmann retractors dorsally and plantarly to protect the soft tissues.
- Using a broad oscillating saw blade, initiate a transverse osteotomy in line with the skin incision.
- Orientation of the Cut: The cut must be made at a right angle (90 degrees) to the lateral border of the calcaneus. In the sagittal plane, it should be inclined posteriorly at an angle of approximately 45 degrees to the plantar plane of the foot.

4. Mobilization and Displacement
- Once the lateral cortex, cancellous body, and medial cortex are breached, ensure the osteotomy is completely free.
- Place a toothless lamina spreader or a broad osteotome into the osteotomy site. Gently spread the fragments to stretch and relax the stout medial soft tissue attachments (medial periosteum and retinaculum) to the calcaneus.

- Withdraw the lamina spreader. Using a periosteal elevator or a specialized calcaneal displacement tool, translate the posterior calcaneal tuberosity approximately 10 mm medially.
- Critical Pitfall: Do not shift the tuberosity into varus. The translation must be a pure medial slide. Furthermore, take extreme care to prevent the posterior tuberosity from sliding proximally (dorsally) due to the pull of the Achilles tendon, which would result in a loss of calcaneal pitch and weakness in plantarflexion.

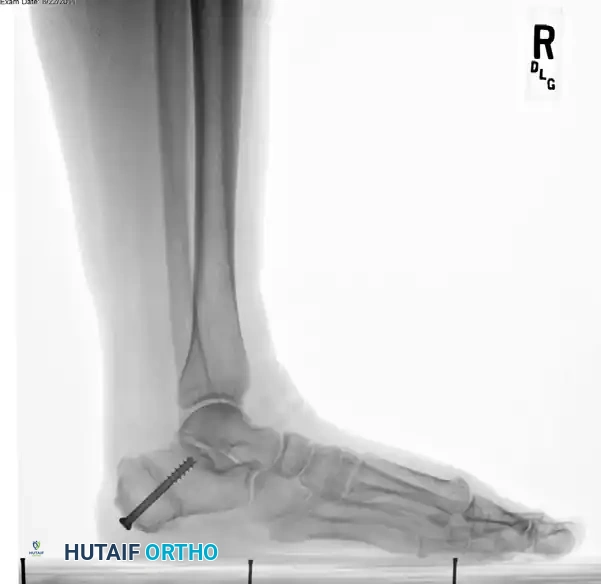
5. Fixation
- Once the 10 mm medial translation is achieved and held provisionally with a smooth Steinmann pin, prepare for definitive fixation.
- Secure the osteotomy with a single, large-diameter (6.5 mm to 7.3 mm) cannulated, self-tapping, partially threaded cancellous screw.
- Trajectory: Insert the guidewire from the posteromedial and inferior aspect of the calcaneal tuberosity, directing it toward the anterolateral and superior aspect of the anterior calcaneal process (aiming toward the sinus tarsi).
- Ensure rigid compression across the osteotomy site.
Surgical Warning: To ensure rigid fixation and prevent iatrogenic arthritis, strictly avoid inserting the screw into the posterior facet of the subtalar joint. Intraoperative fluoroscopy (Broden's views and lateral views) is essential to confirm extra-articular hardware placement.



6. Closure and Repositioning
- Irrigate the wound copiously.
- Close the lateral incision in layers, ensuring a meticulous subcutaneous closure to minimize dead space and a tension-free skin closure.
- Deflate the bean bag, carefully turn the patient to the supine position, and proceed with the planned medial soft tissue procedures (e.g., FDL transfer to the navicular and spring ligament reconstruction).
MANAGEMENT OF STAGE III DISEASE (RIGID DEFORMITY)
While MCDO is highly effective for flexible Stage II disease, it is contraindicated in Stage III PTTD. Stage III disease is characterized by a rigid, fixed deformity of the hindfoot, often accompanied by significant arthrosis and degenerative changes within the triple joint complex (subtalar, talonavicular, and calcaneocuboid joints).
If conservative measures—such as custom-molded double upright ankle-foot orthoses (AFOs) or Arizona braces—fail to provide adequate relief, arthrodesis becomes the definitive surgical indication.

Arthrodesis Options for Stage III AAFD
Multiple arthrodesis configurations have been described, tailored to the specific joints involved and the patient's functional demands:
- Triple Arthrodesis: Historically, the triple arthrodesis (fusion of the subtalar, talonavicular, and calcaneocuboid joints) has been the gold standard for rigid hindfoot deformities. It provides powerful deformity correction and reliable pain relief but sacrifices all hindfoot motion.
- Isolated Talonavicular Arthrodesis: Harper demonstrated that in elderly, low-demand patients, an isolated talonavicular arthrodesis can produce significant deformity correction with satisfactory pain relief. In a review of 29 patients (average follow-up of 26 months), 86% achieved good or excellent results. Biomechanically, fusing the TN joint effectively eliminates nearly all motion in the subtalar and CC joints, stabilizing the entire complex.
- Isolated Subtalar Arthrodesis: Kitaoka and Patzer reported good to excellent results in 16 of 21 patients undergoing isolated subtalar fusion for AAFD. However, they noted that a subset of patients continued to experience residual midfoot pain, highlighting the importance of addressing the medial column if instability persists.
- Subtalar and Talonavicular Arthrodesis (Preserving the CC Joint): Sammarco et al. advocated for correcting the deformity via subtalar and talonavicular fusions while deliberately sparing the calcaneocuboid joint. This technique preserves a degree of flexibility in the lateral column. They reported significant improvements in pain, cosmesis, and shoewear, with only one nonunion in 16 feet.
- Surgical Rationale: Denuding and compressing the talonavicular joint while preserving the calcaneocuboid joint creates a relative lateral column lengthening. This facilitates the correction of severe forefoot abduction without requiring a structural bone graft laterally. This modified double arthrodesis is frequently considered the procedure of choice for severe, rigid cases where the CC joint is free of primary arthrosis.
Medial Column Stabilization
In cases of profound flatfoot deformity where soft tissue procedures are insufficient to restore the medial longitudinal arch, stabilization of the medial column via arthrodesis or osteotomy is required. Greisberg et al. described isolated medial column arthrodesis (e.g., naviculocuneiform or tarsometatarsal fusion) to improve hindfoot alignment, reporting significant improvements in all radiographic parameters. Plantarflexion arthrodesis of the medial column effectively restores the tripod mechanics of the foot, ensuring the first ray bears appropriate weight during the stance phase.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of an MCDO, combined with medial soft tissue reconstruction, relies heavily on strict adherence to postoperative rehabilitation protocols to ensure bony union and protect the tendon transfer.
- Weeks 0-2: The patient is placed in a well-padded short leg splint, strictly non-weight-bearing (NWB). Elevation is critical to manage edema and protect the lateral skin incision.
- Weeks 2-6: Sutures are removed at 2 weeks. The patient is transitioned to a short leg fiberglass cast or a locked CAM boot, remaining strictly NWB.
- Weeks 6-10: Radiographs are obtained at 6 weeks to confirm consolidation of the calcaneal osteotomy. Once early union is evident, the patient may begin progressive partial weight-bearing in a CAM boot. Active and active-assisted range of motion exercises for the ankle and hindfoot are initiated.
- Weeks 10-12: Transition to full weight-bearing in supportive athletic shoes fitted with a custom medial longitudinal arch orthotic.
- Months 3-6: Intensive physical therapy focusing on eccentric strengthening of the gastrocsoleus complex, proprioceptive retraining, and strengthening of the transferred FDL. Maximum medical improvement is typically achieved between 9 and 12 months postoperatively.
CLINICAL OUTCOMES AND COMPLICATIONS
The clinical outcomes of MCDO for Stage II AAFD are highly favorable. Myerson and Corrigan's landmark review of 32 patients demonstrated that at an average of 20 months postoperatively, 94% of patients experienced significant pain relief, improvement in the arch of the foot, and the ability to wear regular shoes without rigid orthotic support. Radiographic correction of the deformity was reliably maintained.
Potential Complications:
* Sural Neuritis: The most common complication, resulting from traction or direct injury during the lateral approach.
* Delayed Union / Nonunion: Rare, given the excellent vascularity and broad cancellous surfaces of the calcaneal tuberosity. Smoking cessation is mandatory.
* Undercorrection: Failure to translate the tuberosity a full 10 mm, or failure to address concomitant medial column instability (e.g., a supinatus deformity), can lead to residual valgus.
* Overcorrection (Varus): Iatrogenic varus tilt of the tuberosity during translation can lead to a rigid, painful lateral column overload and must be strictly avoided intraoperatively.
* Symptomatic Hardware: The prominent head of the cannulated screw at the heel pad may cause local irritation, necessitating hardware removal after complete bony consolidation (typically after 6-12 months).
You Might Also Like
