Soft-Tissue Reduction Techniques for Onychocryptosis: The Jansey and Bose Procedures
Key Takeaway
The Jansey and Bose techniques offer a tissue-sparing approach to onychocryptosis by excising hypertrophic lateral nail folds without disturbing the nail plate or germinal matrix. These procedures address the pathoanatomy of the overgrown ungual labia rather than the nail itself. Long-term outcomes demonstrate high efficacy when meticulous surgical technique, adequate wedge resection, and appropriate postoperative footwear modifications are employed.
Introduction to Soft-Tissue Reduction in Onychocryptosis
Onychocryptosis, commonly known as an ingrown toenail, is a pervasive and debilitating condition frequently encountered in orthopedic and podiatric practice. While traditional surgical management has heavily favored partial or total nail avulsion combined with chemical or surgical matrixectomy (e.g., the Winograd or Zadik procedures), these techniques inherently alter the anatomy of the nail unit. In cases where the nail plate itself is of normal width and morphology, the primary pathology often lies not within the nail, but within the hypertrophic, inflamed lateral nail fold (the ungual labia).
The Jansey and Bose techniques represent a critical paradigm shift in the management of onychocryptosis. Operating on the principle that "the nail is innocent and the skin is guilty," these soft-tissue reduction procedures focus entirely on excising the hypertrophic lateral nail fold. By meticulously avoiding any disturbance to the nail plate or the germinal matrix, these techniques preserve the natural biomechanics and cosmesis of the nail unit while definitively addressing the source of impingement.
Pathoanatomy and Biomechanics of the Nail Unit
To fully appreciate the rationale behind the Jansey and Bose procedures, the operating surgeon must understand the complex biomechanics of the first ray and the hallux nail unit. The nail plate is bordered laterally and proximally by the nail folds (paronychium and eponychium, respectively).
In the pathogenesis of onychocryptosis, extrinsic factors—such as constrictive footwear, improper nail trimming techniques, or repetitive microtrauma—cause the lateral nail fold to bulge over the lateral margin of the nail plate. During the toe-off phase of the gait cycle, ground reaction forces push the plantar soft tissues dorsally and laterally. If the nail fold is hypertrophic, it is driven directly into the sharp, rigid edge of the nail plate. This mechanical conflict breaches the epidermis, allowing normal skin flora (predominantly Staphylococcus aureus) to colonize the dermal tissues, leading to a cascade of inflammation, infection, and the formation of exuberant granulation tissue.
💡 Clinical Pearl: The "Innocent Nail" Concept
Before selecting a surgical intervention, carefully evaluate the width of the nail plate relative to the nail bed. If the nail plate is not abnormally wide or excessively incurvated (pincer nail), a matrixectomy may unnecessarily narrow the nail, leading to poor cosmetic outcomes. In these patients, soft-tissue reduction via the Jansey or Bose technique is the anatomically superior choice.
Indications and Patient Selection
The Jansey and Bose techniques are highly specialized procedures that yield excellent results when applied to the correct patient demographic.
Primary Indications:
* Stage II and Stage III Onychocryptosis: Patients presenting with significant hypertrophy of the lateral nail fold, accompanied by chronic inflammation, purulent drainage, or exuberant granulation tissue.
* Recurrent Onychocryptosis: Patients who have previously undergone partial nail avulsions and now possess a narrow nail plate, yet continue to experience soft-tissue impingement.
* Preservation of Cosmesis: Patients who strongly desire to maintain the natural width and appearance of their toenail.
* Pediatric and Adolescent Patients: Where preservation of the native nail matrix is highly desirable to ensure normal future nail growth.
Contraindications:
* Severe pincer nail deformity (excessive transverse overcurvature of the nail plate), which requires matrix alteration.
* Active, spreading cellulitis extending beyond the digit (requires systemic antibiotic therapy prior to elective soft-tissue resection).
* Severe peripheral arterial disease (PAD) or uncontrolled diabetes mellitus with compromised microvascular perfusion, which may impair secondary intention healing.
Preoperative Preparation and Anesthesia
Meticulous preoperative preparation is essential for optimizing visualization and ensuring patient comfort during soft-tissue resection.
- Positioning: The patient is placed in the supine position. The affected foot is positioned at the edge of the operating table, with a bolster placed under the ipsilateral calf to elevate the heel and provide unobstructed access to the hallux.
- Anesthesia: A standard digital ring block or a Mayo block is performed using a 50/50 mixture of 1% Lidocaine and 0.5% Bupivacaine plain. The use of epinephrine in digital blocks remains controversial; however, current evidence-based literature supports its safety in patients without severe peripheral vascular disease. Nonetheless, many surgeons prefer plain local anesthetics combined with a mechanical tourniquet to ensure absolute safety against digital ischemia.
- Exsanguination and Tourniquet: The digit is exsanguinated by elevating the limb and applying a sterile Penrose drain or a commercial digital tourniquet at the base of the toe. A bloodless surgical field is absolutely critical, as the lateral nail fold is highly vascular, and brisk bleeding will obscure the surgical planes.
- Preparation: The foot is prepped and draped in a standard sterile fashion. If gross purulence is present, the area is aggressively irrigated with sterile saline or a dilute povidone-iodine solution prior to incision.
Surgical Technique: The Jansey Procedure
The Jansey technique is a highly effective, linear soft-tissue resection that removes the offending lateral nail fold while leaving the nail matrix entirely unmolested.
Step 1: Initial Incision and Penetration
The procedure begins with the precise placement of a No. 11 scalpel blade. The surgeon inserts the sharp point of the No. 11 blade directly under the hypertrophic nail fold, targeting the midportion of the lateral nail border. The blade is angled such that the tip penetrates the skin approximately 5 to 7 mm plantarward to the nail fold.
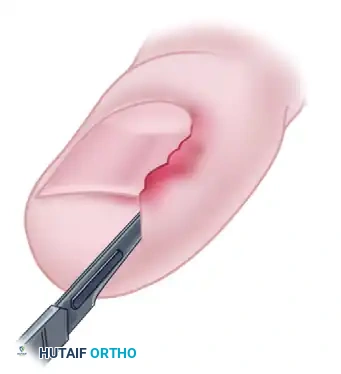
FIGURE 87-21A: Incision into the nail fold. The No. 11 blade is inserted under the hypertrophic tissue, penetrating plantarward to establish the resection plane.
Step 2: Distal Advancement
Once the blade has penetrated the tissue to the appropriate depth, the surgeon advances the blade distally in a smooth, straight line. This motion effectively slices through the hypertrophic nail fold, removing the distal portion of the offending tissue and exposing the distal half of the lateral edge of the nail plate.
⚠️ Surgical Warning: Matrix Preservation
Throughout the distal and proximal advancement of the blade, the surgeon must maintain strict spatial awareness of the nail matrix and the nail plate. The flat edge of the blade should glide parallel to the nail margin. In neither the Jansey nor the Bose technique is the nail or nail bed disturbed. Inadvertent scoring of the nail bed can lead to postoperative onycholysis or epidermoid cyst formation.

FIGURE 87-21B: Distal advancement of the blade. Note that neither the nail matrix nor the nail plate is disturbed during this soft-tissue resection.
Step 3: Proximal Excision
After the distal half of the nail fold is freed, the surgeon reverses the direction of the No. 11 blade. The blade is drawn proximally to excise the remaining hypertrophic nail fold at the base of the nail. This completes the linear wedge resection of the lateral paronychium.
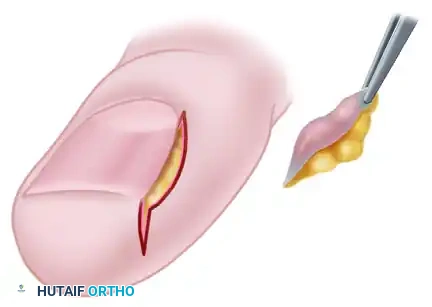
FIGURE 87-21C: A wedge of the hypertrophic nail fold is completely excised using tissue forceps, clearing the lateral margin of the nail plate.
Step 4: Coronal Verification and Debridement
Following the excision, the surgeon must inspect the surgical site from a coronal perspective to ensure that an adequate volume of tissue has been removed. The goal is to create a spatial gap between the lateral edge of the nail plate and the newly created skin margin, ensuring that future weight-bearing forces will not drive the skin back into the nail.
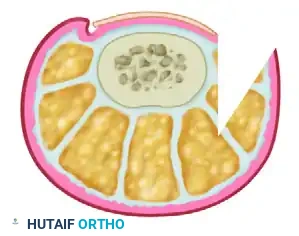
FIGURE 87-21D: Coronal view demonstrating the substantial amount of soft tissue removed. The wedge excision effectively eliminates the mechanical conflict between the nail plate and the ungual labia.
At this stage, the surgeon must carefully inspect the lateral nail sulcus. Trim any residual nail spikes flush with the lateral nail margin using a dual-action nail nipper. Failure to remove hidden nail spicules is a primary cause of early surgical failure and persistent postoperative pain.
Step 5: Hemostasis and Closure
Upon release of the digital tourniquet, bleeding is usually brisk due to the rich vascular network of the digital pulp and paronychium. Hemostasis can be achieved through direct, sustained local pressure or the judicious use of bipolar electrocautery.
Closure of the Jansey procedure is entirely optional. Many surgeons prefer to leave the wound open to heal by secondary intention, which allows for continuous drainage and reduces the risk of closed-space infection. If closure is desired to expedite epithelialization, simple interrupted sutures (e.g., 4-0 non-absorbable nylon or prolene) can be placed to approximate the plantar skin edge to the nail bed margin.

FIGURE 87-21E: Primary closure of the Jansey procedure. Closure is optional and should only be performed if the wound edges approximate without excessive tension.
Surgical Technique: The Bose Procedure
The Bose technique shares the same fundamental philosophy as the Jansey procedure—preservation of the nail unit through targeted soft-tissue resection—but differs slightly in its geometric approach to the excision.
For the Bose technique, no nail or matrix is removed. Instead of a linear slice, a distinct, wide wedge consisting of the entire hypertrophic nail fold is excised. This technique is particularly useful for patients with massive, bulbous hypertrophy of the lateral nail fold that extends significantly over the dorsal aspect of the nail plate.
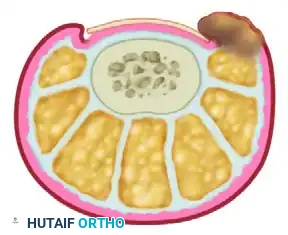
FIGURE 87-22: Bose technique of nail fold removal. A wide, elliptical wedge of the hypertrophic paronychial tissue is excised, completely decompressing the lateral nail margin without altering the nail plate.
The Bose excision is typically left open to heal by secondary intention. The resulting defect fills with healthy granulation tissue and epithelializes over a period of 3 to 5 weeks, resulting in a flat, non-impinging lateral nail fold.
Postoperative Care and Rehabilitation Protocol
The success of soft-tissue reduction procedures relies heavily on strict adherence to postoperative care protocols. Because these wounds are often left to heal by secondary intention, patient compliance is paramount.
Immediate Postoperative Phase (Days 0-2):
* Dressing: Cover the wound with a nonadherent dressing (e.g., Adaptic or Xeroform) to prevent the regenerating tissue from adhering to the gauze. Wrap the toe securely in sterile gauze and secure with a mild compressive wrap (e.g., Coban) to manage postoperative edema and minor oozing.
* Activity: The patient is instructed to elevate the foot above the level of the heart for the first 48 hours to minimize throbbing pain and swelling. Weight-bearing is permitted as tolerated, but ambulation should be minimized.
Early Rehabilitation Phase (Days 2-10):
* Wound Care: The initial surgical dressing is removed at 48 hours. At this point, the patient is instructed to begin warm water soaks (often with Epsom salts or dilute chlorhexidine) for 15 to 20 minutes, twice daily. This promotes vasodilation, aids in the mechanical debridement of exudate, and soothes the surgical site.
* Footwear: The patient must strictly avoid wearing closed-toe shoes for 7 to 10 days. Open-toed sandals or a rigid postoperative shoe are mandatory to prevent extrinsic compression on the healing lateral nail fold.
* Suture Management: If the surgeon opted for primary closure (as seen in Figure 87-21E), the sutures are removed at 7 to 10 days postoperatively.
Long-Term Phase (Weeks 2 and Beyond):
* Once the wound has sufficiently epithelialized or the sutures are removed, the patient may transition back to standard footwear. However, it is critical that the patient utilizes a wide toe box shoe to prevent recurrence of the mechanical impingement that caused the initial pathology.
Long-Term Follow-Up and Clinical Outcomes
Evaluating the long-term efficacy of soft-tissue reduction techniques requires a critical analysis of the available literature. Long-term follow-up data specifically isolating the Jansey and Bose procedures are historically difficult to find in large-scale randomized controlled trials, largely due to the overwhelming popularity of chemical matrixectomies in modern practice.
However, historical and retrospective data provide valuable insights. Jansey originally stated that he had utilized his specific soft-tissue reduction procedure for more than 20 years with minimal complications. When performed correctly, the technique permanently alters the spatial relationship between the nail plate and the paronychium, effectively curing the condition without sacrificing nail width.
Conversely, the literature does present conflicting data regarding soft-tissue resections. One notable report analyzing partial nail avulsion combined with an elliptical lateral nail fold excision demonstrated a recurrence rate of 16.6%.
📊 Academic Insight: Analyzing Recurrence Rates
The 16.6% recurrence rate reported in some soft-tissue excision studies is often attributable to two primary surgical errors:
1. Inadequate Wedge Resection: Failure to remove a sufficiently deep or wide wedge of tissue (as demonstrated in Figure 87-21D) allows the paronychium to regenerate and re-impinge on the nail plate.
2. Failure to Address Nail Spikes: Leaving a sharp spicule of nail deep in the proximal sulcus will inevitably lead to recurrent inflammation, regardless of how much soft tissue is removed.
To achieve the "minimal complications" reported by Jansey, the operating surgeon must be aggressive in the soft-tissue resection and meticulous in the exploration of the lateral gutter for hidden nail fragments.
Complications and Pitfalls
While generally considered safe and tissue-sparing, the Jansey and Bose techniques carry specific risks that the orthopedic surgeon must be prepared to manage:
- Recurrence: As noted, inadequate resection of the ungual labia or failure of the patient to adopt wide toe box footwear can lead to recurrent impingement.
- Infection: Because these procedures are often performed in the presence of pre-existing localized infection (paronychia), postoperative cellulitis is a risk. Aggressive intraoperative irrigation and postoperative warm soaks are critical mitigators.
- Epidermal Inclusion Cysts: If the No. 11 blade inadvertently scores or implants fragments of the germinal matrix into the deep dermal tissues during the proximal excision, an epidermal inclusion cyst or a spicule of ectopic nail may develop months later.
- Prolonged Healing: Wounds left to heal by secondary intention (particularly the wider Bose excision) may take several weeks to fully epithelialize, requiring prolonged patient compliance with wound care protocols.
Conclusion
The Jansey and Bose procedures remain highly valuable techniques in the armamentarium of the orthopedic surgeon managing onychocryptosis. By adhering to the philosophy of preserving the innocent nail plate and aggressively resecting the guilty hypertrophic soft tissue, these techniques offer a functional and cosmetically superior alternative to traditional matrixectomies. Mastery of the precise blade angles, adequate wedge resection, and strict postoperative footwear modifications will ensure excellent long-term outcomes and high patient satisfaction.
You Might Also Like
