Medial Approach Triple Arthrodesis: Surgical Technique
Key Takeaway
The isolated medial approach to triple arthrodesis, popularized by Myerson, is an invaluable technique for patients at high risk of lateral wound complications. This approach is particularly indicated in cases of severe rheumatoid arthritis, prior lateral surgical incisions, or compromised lateral soft tissue envelopes. By utilizing a single medial incision, surgeons can effectively prepare and fuse the subtalar, talonavicular, and calcaneocuboid joints while minimizing catastrophic wound breakdown and optimizing biomechanical alignment.
INTRODUCTION TO THE ISOLATED MEDIAL APPROACH
Triple arthrodesis remains the gold standard for the surgical management of severe, rigid hindfoot deformities, end-stage osteoarthritis, and inflammatory arthropathies affecting the subtalar, talonavicular (TN), and calcaneocuboid (CC) joints. Traditionally, this procedure is performed via a dual-incision technique (a lateral incision for the subtalar and CC joints, and a medial incision for the TN joint). However, the lateral soft tissue envelope of the hindfoot is notoriously tenuous, possessing a fragile vascular supply that is highly susceptible to catastrophic wound breakdown, dehiscence, and deep infection.
To mitigate these risks, Mark S. Myerson described an isolated medial approach to the triple arthrodesis. This technique is specifically designed for patients at an elevated risk for lateral wound complications. By accessing all three joints of the hindfoot complex through a single medial window, the surgeon preserves the lateral vascular perforators and avoids placing an incision over compromised skin.
Indications and Patient Selection
The isolated medial incision is not universally indicated for all triple arthrodeses but is a powerful tool in the armamentarium of the foot and ankle reconstruction specialist. Primary indications include:
- Rheumatoid Arthritis (RA) and Systemic Inflammatory Disease: Patients with RA often present with severe valgus hindfoot deformities, systemic vasculitis, and poor tissue turgor secondary to chronic corticosteroid or biologic therapy. A single medial incision significantly reduces the risk of postoperative wound necrosis.
- Compromised Lateral Soft Tissue Envelope: Patients with a history of prior lateral surgical approaches (e.g., extensile lateral approach for calcaneal fractures), previous lateral infections, or severe scarring.
- Severe Rigid Valgus Deformity: In cases of end-stage posterior tibial tendon dysfunction (Stage III or IV) where the lateral skin is already contracted and under tension, a lateral incision is at high risk of failing to close or breaking down postoperatively.
💡 Clinical Pearl: Patient Optimization
In patients with rheumatoid arthritis, coordinate with the treating rheumatologist regarding the perioperative management of disease-modifying antirheumatic drugs (DMARDs) and biologic agents. While methotrexate can often be continued, biologic agents (e.g., TNF-alpha inhibitors) typically require cessation prior to surgery to optimize wound healing and minimize infection risk.
BIOMECHANICS AND PATHOANATOMY
The subtalar, talonavicular, and calcaneocuboid joints function as a highly coupled biomechanical unit, often referred to as the coxa pedis or the transverse tarsal locking mechanism. Motion in one joint obligates motion in the others.
Arthrodesis of the talonavicular joint alone eliminates approximately 90% of subtalar joint excursion. Therefore, when performing a triple arthrodesis, the primary goal is not merely the cessation of painful motion, but the restoration of a plantigrade, biomechanically sound foot. The medial approach allows excellent visualization for the correction of hindfoot valgus and the restoration of the medial longitudinal arch. However, because the calcaneocuboid joint is accessed indirectly across the foot, meticulous technique is required to ensure adequate preparation and avoid nonunion.
PREOPERATIVE PLANNING AND POSITIONING
Standard weight-bearing radiographs (anteroposterior, lateral, and mortise views of the ankle, as well as AP, lateral, and oblique views of the foot) are mandatory. A preoperative computed tomography (CT) scan is highly recommended to assess bone stock, identify cystic changes, and evaluate the exact morphology of the subtalar and transverse tarsal joints.
Positioning:
* The patient is placed in the supine position on a radiolucent operating table.
* A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position, allowing access to both the medial and lateral aspects of the leg.
* A well-padded thigh tourniquet is applied.
* Intraoperative fluoroscopy must be positioned to allow seamless AP, lateral, and axial imaging of the hindfoot without compromising the sterile field.
SURGICAL TECHNIQUE: STEP-BY-STEP
Phase 1: Proximal Peroneal Tendon Release
In rigid valgus deformities, the peroneus brevis and longus act as powerful deforming forces. Releasing these tendons proximally removes this deforming vector and facilitates the reduction of the hindfoot without requiring a lateral incision over the foot itself.
- Incision: Make a 2-cm longitudinal incision over the peroneal tendons approximately 10 cm proximal to the level of the ankle joint.
> ### ⚠️ Surgical Warning
> To avoid catastrophic wound problems in this high-risk patient cohort, absolutely do not make the incision on the lateral aspect of the foot. Keep the incision strictly proximal to the lateral malleolus. - Tendon Delivery: Dissect through the subcutaneous tissue to the peroneal fascia. Open the fascia longitudinally. Use a mosquito clamp to hook and deliver both the peroneus longus and peroneus brevis tendons out of the incision.
- Tenotomy: Divide both tendons sharply.

Figure A: A mosquito clamp is used to deliver the peroneus longus and brevis tendons out of a 2-cm longitudinal incision approximately 10 cm proximal to the ankle joint.
💡 Clinical Pearl: Peroneus Longus Management
We do not recommend leaving the peroneus longus tendon intact. Despite its potential beneficial effect on plantarflexing the first metatarsal, an intact peroneus longus in a rigid deformity may still limit inversion and impede the correction of the valgus hindfoot.
Phase 2: The Medial Incision and Exposure
- Main Incision: Make an 8-cm medial longitudinal incision. The incision should extend from the undersurface of the medial malleolus and be centered directly over the talonavicular joint, following the course of the posterior tibial tendon.
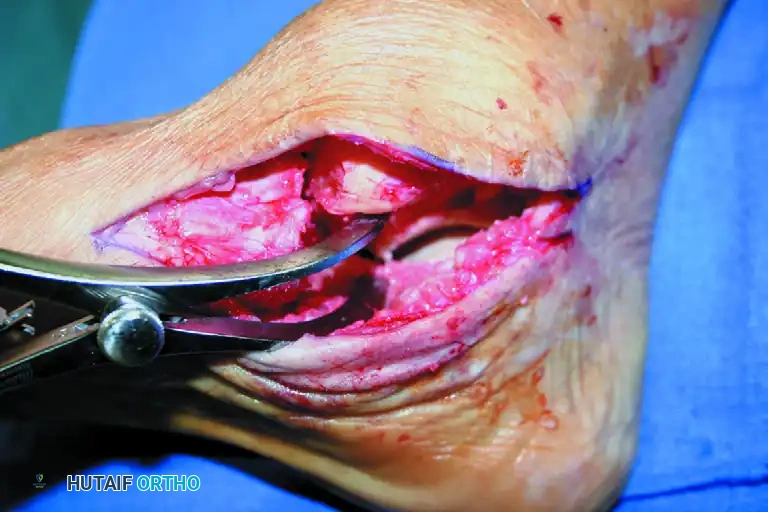
Figure B: An 8-centimeter medial longitudinal incision is centered over the talonavicular joint.
- Superficial Dissection: Divide the subcutaneous tissue longitudinally. Carefully identify the branches of the saphenous vein crossing the medial tarsus. Tie or coagulate these communicating veins that cross the wound at right angles to prevent postoperative hematoma.
- Nerve Management: Identify the branches of the saphenous nerve. While preservation is ideal, if a branch compromises the surgical exposure, it can be sacrificed cleanly to prevent traction neuritis.
- Capsulotomy: Incise the talonavicular joint capsule longitudinally.
Phase 3: Joint Preparation (Talonavicular and Subtalar)
- Talonavicular Identification: Abduct and adduct the forefoot to clearly identify the articular margins of the talonavicular joint.
- Tendon Débridement: Remove any degenerative remnants of the posterior tibial tendon from its insertion on the navicular tuberosity to clear the medial workspace.
- Deep Exposure: Utilize a subperiosteal dissection technique to gain the necessary exposure of the talonavicular and subtalar joints.
> ### ⚠️ Surgical Warning: Neurovascular Protection
> Place a blunt Hohmann or right-angle retractor carefully under the talus to protect the flexor digitorum longus (FDL), flexor hallucis longus (FHL), and the critical medial neurovascular bundle (posterior tibial artery and tibial nerve). - Subtalar Access: Follow the neck of the talus proximally and inferiorly to expose the anterior, middle, and posterior facets of the subtalar joint.
- Cartilage Removal: Use a combination of curved and straight osteotomes, curettes, and a lamina spreader to expose and débride the talonavicular joint, the subtalar joint, and the sinus tarsi. Pay special attention to the lateral aspect of the talonavicular joint, which can be difficult to visualize from the medial side.
- Subchondral Preparation: Remove all eburnated or sclerotic subchondral bone down to healthy, bleeding, cancellous bony surfaces. Small, thin osteotomes are highly effective for this delicate work.

Figure C: All eburnated or subchondral bone is meticulously removed from the talonavicular joint to expose bleeding, cancellous bony surfaces.
- Osteoconduction: Drill multiple small holes (using a 2.0mm or 2.5mm drill bit) on both sides of the prepared joints to stimulate vascular ingrowth and promote osteogenesis.
Phase 4: Calcaneocuboid Joint Preparation
Preparation of the calcaneocuboid (CC) joint is universally considered the most challenging aspect of the single-incision medial approach, as it requires working across the width of the foot.
- Exposure: Place a lamina spreader directly into the prepared talonavicular joint and open it to distract the midfoot. This maneuver provides the necessary visual and physical access to the lateral column.
- Capsular Release: Reach across the foot with a long-handled scalpel (e.g., a #15 blade on a long handle). Sharply release the capsule of the calcaneocuboid joint and the bifurcate ligament by feel.

Figure D: A lamina spreader is placed in the talonavicular joint to distract the midfoot, allowing for deep exposure of the calcaneocuboid joint.
- Débridement: Because the calcaneocuboid joint has a relatively flat articular surface, débridement and scaling of the cartilage can be achieved using long, straight curettes and narrow osteotomes passed through the medial window. Ensure all cartilage is removed down to bleeding bone.
Phase 5: Reduction and Fixation
Anatomic reduction and rigid internal fixation are paramount. The sequence of fixation is critical to achieving a plantigrade foot.
- Subtalar Reduction and Fixation:
- Reduce the subtalar joint, correcting the valgus deformity by translating the calcaneus medially and restoring hindfoot height.
- Temporarily pin the joint with a heavy Kirschner wire.
- Fix the subtalar joint with a single 6.5-mm (or larger) partially threaded cannulated screw. The trajectory should extend from the posterior non-weight-bearing aspect of the calcaneus, across the posterior facet, and into the dense bone of the talar body.
- Talonavicular Reduction and Fixation:
- Realign the transverse tarsal joints.
- Crucial Step: Pay careful attention to any residual forefoot supination. As the hindfoot valgus is corrected, the forefoot will often supinate. This must be manually reduced (pronated) through the transverse tarsal joint before fixation.
- Fix the talonavicular joint with two 4.5-mm or 5.0-mm cannulated screws to prevent rotational instability.
- Calcaneocuboid Fixation:
- Place a percutaneous, posteriorly directed 4.5-mm or 5.0-mm cannulated screw across the calcaneocuboid joint.
- The starting point is at the dorsal-anterior aspect of the cuboid, aiming proximal and plantar into the anterior process of the calcaneus.

Figure E: A posteriorly directed 4.5-mm or 5.0-mm screw is inserted percutaneously across the calcaneocuboid joint.
- Radiographic Confirmation: Utilize intraoperative fluoroscopy to confirm the anatomic reduction of all three joints, the complete seating of all screw heads, and the appropriate length of the hardware without joint penetration.

Figure F: Completed fixation includes two cannulated screws in the talonavicular joint, one large (6.5-mm) screw through the posterior calcaneus into the talar body, and a percutaneous screw across the calcaneocuboid joint.
- Closure: Thoroughly irrigate the wound. Perform a layered closure, ensuring the capsule and subcutaneous tissues are meticulously reapproximated to eliminate dead space. Close the skin with non-absorbable sutures using a tension-free technique (e.g., Allgöwer-Donati or vertical mattress).
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The postoperative protocol must be strictly adhered to, as premature weight-bearing can lead to catastrophic hardware failure or nonunion, particularly in patients with compromised bone density (e.g., rheumatoid arthritis).
- 0 to 14 Days: The patient is placed in a well-padded, bulky posterior splint with a U-stirrup in the operating room. The limb is strictly elevated above heart level to minimize edema. At 14 days, the splint is removed, the wound is inspected, and sutures are removed.
- 2 to 6 Weeks: The patient is transitioned to a short-leg fiberglass cast. Touch-down weight-bearing (TDWB) may be permitted depending on bone quality, but strict non-weight-bearing (NWB) is strongly encouraged to optimize the fusion mass.
- 6 to 12 Weeks: At the 6-week mark, radiographs are obtained. If early consolidation is visible, the patient may begin progressive full weight-bearing in a cast. The cast is maintained for a total of 12 weeks from the date of surgery.
- 12+ Weeks: At 12 weeks, the cast is removed. Radiographs are taken to confirm clinical and radiographic union. The patient is placed in support hose (compression stockings) to manage dependent edema and transitioned to a large, soft-soled, cushioned shoe. A short-leg removable walking boot (CAM boot) may be utilized during this transition phase and worn for an additional 4 to 6 weeks.
- Long-Term Expectations: The surgeon must explicitly inform the patient preoperatively that dependent swelling of the foot and ankle is expected to persist for up to 1 year, and occasionally, mild edema may persist indefinitely due to the alteration of venous and lymphatic return pathways.
COMPLICATIONS AND PITFALLS
While the medial approach significantly reduces lateral wound complications, it introduces specific technical challenges:
- Calcaneocuboid Nonunion: Because the CC joint is prepared indirectly across the foot, inadequate cartilage removal is a risk. Utilizing a lamina spreader in the TN joint is mandatory for adequate visualization. If the CC joint cannot be adequately prepared medially, a limited 2-cm lateral incision directly over the CC joint may be required as a salvage maneuver.
- Malunion (Residual Forefoot Supination): Correcting severe hindfoot valgus unmasks forefoot supination. Failure to recognize and correct this at the transverse tarsal joint prior to TN fixation will result in a lateral border overload and a painful, non-plantigrade foot.
- Neurovascular Injury: The medial approach places the posterior tibial neurovascular bundle at risk during the plantar and lateral dissection of the subtalar joint. Retractors must be placed subperiosteally and with extreme care.
-
Hardware Prominence: The medial skin over the navicular is thin. Ensure the heads of the TN screws are adequately countersunk to prevent painful hardware prominence, which may necessitate later removal.
You Might Also Like
