Mastering Hindfoot Reconstruction: Arthrodesis Techniques and Biomechanics
Key Takeaway
Hindfoot arthritis frequently presents with complex deformities driven by dynamic stabilizer imbalance and static restraint failure. Surgical management, including subtalar, double, or triple arthrodesis, aims to restore a plantigrade, stable foot. Precise correction requires 5 to 10 degrees of hindfoot valgus, meticulous joint preparation, and rigid internal fixation. This guide details the biomechanics, indications, and step-by-step operative techniques for hindfoot reconstruction.
Introduction to Hindfoot Pathology and Biomechanics
Primary degenerative arthritis with preserved, physiological alignment may occur in the hindfoot, but it is exceedingly rare as an isolated entity. More commonly, hindfoot arthropathy is inextricably linked to underlying instability, structural deformity, or systemic inflammatory conditions. The pathogenesis frequently stems from an imbalance of the dynamic stabilizers of the hindfoot—most notably the posterior tibial tendon (PTT) and the peroneal tendon complex.
However, the hindfoot does not exist in isolation. Pathological processes originating in the ankle, midfoot, or forefoot can exert abnormal biomechanical forces, leading to the malalignment of an otherwise normal hindfoot. Over time, these aberrant forces contribute to the progressive insufficiency of static stabilizers (such as the spring ligament complex, plantar fascia, and deltoid ligament), culminating in the degeneration of the transverse tarsal and subtalar joints.
Subtalar motion is typically the first and most severely affected parameter. Furthermore, the vast majority of patients presenting for consideration of subtalar or triple arthrodesis exhibit a concomitant contracture of the gastrocsoleus complex.
Clinical Pearl: Examination of the hindfoot must always be performed with the patient bearing weight. Non-weight-bearing assessments will mask flexible deformities and fail to demonstrate the true extent of static stabilizer insufficiency. The Coleman block test is mandatory to differentiate between a flexible and rigid hindfoot deformity driven by a plantarflexed first ray.
Rheumatoid Arthritis and Inflammatory Arthropathies
The ankle and hindfoot are involved in 30% to 60% of patients suffering from rheumatoid arthritis (RA). In this demographic, hindfoot deformity is frequently the most debilitating aspect of the disease, severely limiting ambulation and independence.
The hallmark clinical presentation of the rheumatoid hindfoot is severe heel valgus, which precipitates a cascade of secondary deformities: resultant midfoot arch collapse (pes planovalgus) and forefoot rotation in an axial plane (abduction and supination). These profound structural failures are driven by a combination of aggressive synovitis, synovial hypertrophy, and eventual articular destruction of the tibiotalar (ankle), subtalar, and talonavicular joints.
Clinical Presentation and Diagnostic Evaluation
Patients typically present with a primary complaint of deep, aching pain localized to the sinus tarsi and the subfibular region. This pain is characteristically activity-related and frequently associated with localized swelling and effusion.
Diagnostic Warning: Any indication of an inflammatory arthropathy—such as bilateral hindfoot symptoms, multiple joint complaints, or advanced joint degeneration in a young patient lacking a history of significant trauma—must prompt a rigorous rheumatological workup.
Standard weight-bearing radiographs (anteroposterior, lateral, and mortise views of the ankle, alongside AP, lateral, and oblique views of the foot) are essential. A weight-bearing AP radiograph of the ankle joint is particularly critical for diagnosing concomitant ankle joint instability or asymmetric joint space narrowing, which may dictate the need for a pantalar or tibiotalocalcaneal (TTC) arthrodesis rather than an isolated hindfoot procedure.
Non-Operative Management
Conservative management remains the first line of treatment, particularly in the early stages of degenerative or inflammatory arthropathy.
* Pharmacotherapy: Oral nonsteroidal anti-inflammatory drugs (NSAIDs) and disease-modifying antirheumatic drugs (DMARDs) for RA patients.
* Orthotics and Bracing: Custom-molded arch supports, medial heel wedges, or articulated Ankle-Foot Orthoses (AFOs) can mechanically unload the painful joints and stabilize flexible deformities.
* Corticosteroid Injections: Fluoroscopically or ultrasound-guided intra-articular steroid injections into the subtalar or talonavicular joints can provide significant diagnostic information and therapeutic relief.
Progressive arthritis, however, inevitably results in increased deformity. As the structural architecture of the foot collapses, pain intensifies, making standard shoewear impossible and rendering bracing ineffective or poorly tolerated due to bony prominences.
Surgical Indications and Decision Making
Failure of conservative treatment, or the presence of persistent synovitis and synovial hypertrophy that remains unrelieved after 6 months of optimized medical therapy, constitutes a definitive indication for surgical intervention.
In patients with flexible deformities, combined bony and soft tissue procedures are often highly beneficial to realign the hindfoot. However, surgical decision-making must be heavily modified in the presence of inflammatory arthropathy.
Surgical Pitfall: In patients with rheumatoid arthritis or other destructive inflammatory arthropathies, isolated soft-tissue procedures (tendon transfers, tendon grafts, or tendon advancements) should be used with extreme caution. The underlying destructive disease process will inevitably compromise the transferred tissue. Bony stabilization (arthrodesis) is almost always required to maintain correction and provide durable symptom relief.
An exception to the requirement for arthrodesis is a patient presenting with heel valgus where symptoms are strictly localized along the course of the posterior tibial tendon, accompanied by obvious tenosynovitis and synovial hypertrophy, but without lateral hindfoot pain (fibular abutment). In this specific scenario, if the deformity of the subtalar and midtarsal joints is completely reducible, an isolated tenosynovectomy of the posterior tibial tendon may be sufficient.
Selecting the Appropriate Arthrodesis
If symptomatic hindfoot valgus is unrelieved by conservative measures, arthrodesis is indicated, provided the tibiotalar (ankle) joint is stable and relatively spared.
- Subtalar Arthrodesis: Indicated to correct heel valgus if the midtarsal joint (talonavicular and calcaneocuboid) has been spared by the degenerative or rheumatoid process.
- Triple Arthrodesis: Indicated when both the subtalar and transverse tarsal joints exhibit advanced arthritis or rigid deformity.
- Double Arthrodesis: As the biomechanical consequences of fusion on adjacent joints have become better understood, limited arthrodesis techniques have gained favor. For patients without involvement of the calcaneocuboid joint, a "double" arthrodesis (fusion of the talonavicular and subtalar joints) is preferred to preserve lateral column mobility (as described by Sammarco et al.).
- Single-Incision Techniques: Wachter et al. described an elegant technique for arthrodesis of the talonavicular and talocalcaneal joints utilizing a single medial incision, minimizing lateral soft tissue stripping.
Operative Techniques in Hindfoot Reconstruction
The overarching goal of surgical treatment is to restore hindfoot stability in a strictly plantigrade, biomechanically sound position.
Target Alignment:
* Hindfoot Valgus: 5 to 10 degrees of valgus must remain. Fusing the hindfoot in varus locks the transverse tarsal joint, creating a rigid lateral column that leads to intractable lateral border pain, fifth metatarsal stress fractures, and rapid adjacent segment degeneration.
* Forefoot Position: The forefoot must be brought medially and plantarward to match the corrected hindfoot.
* Equinus Correction: A percutaneous lengthening of the Achilles tendon (Hoke or Strayer procedure) is frequently required if reducing the talonavicular joint places the ankle into obligate equinus.
Subtalar Arthrodesis: Step-by-Step
1. Patient Positioning and Incision
The patient is placed in the lateral decubitus or supine position with a large bump under the ipsilateral hip to internally rotate the leg, providing excellent access to the lateral hindfoot. A thigh tourniquet is applied.
An anterolateral incision is made, starting at the tip of the lateral malleolus and extending distally toward the base of the fourth metatarsal.

Figure A: The standard anterolateral skin incision for exposure of the subtalar joint, carefully avoiding the sural nerve inferiorly and the superficial peroneal nerve superiorly.
2. Deep Dissection and Joint Exposure
The extensor digitorum brevis (EDB) muscle belly is identified and elevated sharply from its origin on the calcaneus, reflecting it distally. The sinus tarsi fat pad is evacuated. The cervical and interosseous talocalcaneal ligaments are sharply excised to allow distraction of the subtalar joint. A lamina spreader is inserted into the sinus tarsi to open the posterior facet.
3. Articular Surface Preparation
Meticulous joint preparation is the most critical step in preventing nonunion. The articular cartilage and subchondral bone of the posterior facet of the talus and calcaneus are aggressively debrided using curettes, osteotomes, and a high-speed burr.
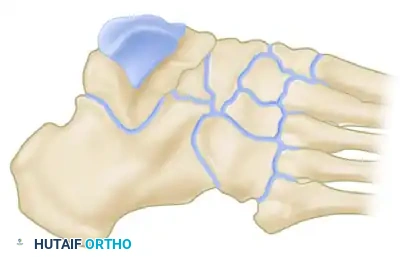
Figure B: Excision of the articular surfaces. The posterior facet of the talus and calcaneus must be completely denuded down to bleeding cancellous bone. The middle and anterior facets should also be addressed if a complete fusion is desired.
The subchondral bone is then "fish-scaled" or drilled with a 2.0mm drill bit to release osteoprogenitor cells and promote robust osteogenesis.
4. Deformity Correction and Provisional Fixation
The lamina spreader is removed. The calcaneus is manually translated medially to correct the valgus deformity, ensuring the heel is positioned in the target 5 to 10 degrees of valgus. The head and neck of the talus are lifted dorsally and laterally. Provisional fixation is achieved with heavy Kirschner wires driven from the calcaneal tuberosity into the body of the talus.
5. Definitive Internal Fixation
Rigid compression is paramount. Typically, one or two large-fragment (6.5 mm or 7.3 mm) cannulated, partially threaded cancellous screws are utilized.
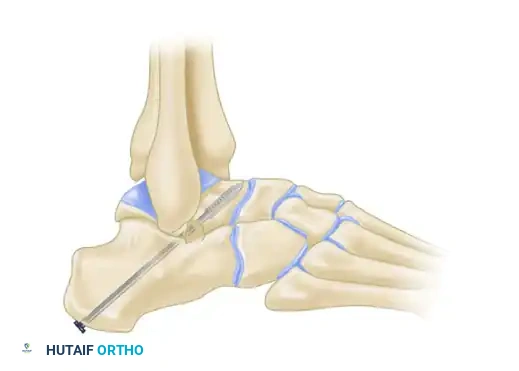
Figure C: Definitive fixation utilizing a large cannulated screw. The trajectory runs from the talar neck-body junction, across the posterior facet, and anchors solidly into the dense bone of the calcaneal tuberosity.
Screws can be placed either from the calcaneus up into the talus, or from the dorsal talar neck down into the calcaneus, depending on surgeon preference and local bone quality. Fluoroscopy is used to confirm hardware placement, ensuring no penetration into the ankle joint or subtalar joint space.
Triple Arthrodesis Considerations
When a triple arthrodesis is indicated, two incisions are classically utilized:
1. Anterolateral Incision: (As described above) for access to the subtalar and calcaneocuboid joints.
2. Medial Incision: Centered over the talonavicular joint, extending from the medial malleolus to the medial cuneiform.
Surgical Warning: Forefoot supination must be strictly avoided when final fixation is placed across the talonavicular joint. If the talonavicular joint is fused in supination, the patient will bear weight exclusively on the lateral border of the foot, leading to severe pain and callosities. The forefoot must be pronated relative to the hindfoot to ensure the first ray engages the ground during the stance phase of gait.
Fixation of the talonavicular and calcaneocuboid joints can be achieved with a variety of constructs, including staples, cannulated screws, or modern low-profile anatomic locking plates, which offer superior biomechanical stability in osteopenic rheumatoid bone.
Postoperative Protocol and Rehabilitation
The success of hindfoot arthrodesis relies heavily on strict adherence to postoperative immobilization protocols.
- Phase 1 (Weeks 0-2): The patient is placed in a bulky, well-padded posterior splint and kept strictly non-weight-bearing. Elevation is critical to manage edema and protect the soft tissue envelope.
- Phase 2 (Weeks 2-6): Sutures are removed at 2 weeks. The patient is transitioned to a short-leg fiberglass cast. Strict non-weight-bearing is maintained.
- Phase 3 (Weeks 6-10): Radiographs are obtained to assess early trabecular bridging. If progressing well, the patient is transitioned to a controlled ankle motion (CAM) boot and begins progressive partial weight-bearing, advancing to full weight-bearing as tolerated.
- Phase 4 (Weeks 10+): Once clinical and radiographic union is confirmed (typically 10-12 weeks), the patient is transitioned to supportive athletic shoes, often with a custom orthotic to support the transverse arch and accommodate the newly fused hindfoot. Physical therapy focuses on proprioception, gait retraining, and strengthening of the proximal kinetic chain.
Complications
Despite meticulous technique, complications can occur:
* Nonunion: The talonavicular joint has the highest rate of nonunion in a triple arthrodesis (up to 10-15%), often due to its complex spherical anatomy and sheer forces.
* Malunion: Fusing the hindfoot in varus is the most devastating malunion, leading to a rigid, painful foot.
* Adjacent Segment Disease: Fusing the hindfoot dramatically increases stress on the ankle joint proximally and the tarsometatarsal joints distally, potentially accelerating osteoarthritis in these regions over the subsequent decade.
===
📚 Medical References
- Hindfoot arthrodesis in adults utilizing a Dowell graft technique, Clin Orthop Relat Res 257:193, 1990.
- Crego CH Jr, Ford LT: An end-result study of various operative procedures for correcting fl at feet in children, J Bone Joint Surg 34A:183, 1952.
- Deland JT, Aronoczky SP, Thompson FM: Adult acquired fl atfoot deformity at the talonavicular joint: reconstruction of the spring ligament in an in vitro model, Foot Ankle 13:327, 1992.
- DuMontier TA, Falicov A, Mosca V, et al: Calcaneal lengthening: investigation of deformity correction in a cadaver fl atfoot model, Foot Ankle Int 26:166, 2005.
- Duncan JW, Lovell WW: Modifi ed Hoke-Miller fl atfoot procedure, Clin Orthop Relat Res 181:24, 1983.
- Evans D: Relapsed club foot, J Bone Joint Surg 43B:722, 1961.
- Evans D: Calcaneo-valgus deformity, J Bone Joint Surg 57B:270, 1975.
- Fraser RK, Menelaus MB, Williams PF, et al: The Miller procedure for mobile fl at feet, J Bone Joint Surg 77B:396, 1995.
- Gallien R, Morin F, Marquis F: Subtalar arthrodesis in children, J Pediatr Orthop 9:59, 1989.
- Geist ES: Supernumerary bones of the foot—a roentgen study of the feet of one hundred normal individuals, Am J Orthop Surg 12:403, 1914.
- Geist ES: The accessory scaphoid bone, J Bone Joint Surg 7:570, 1925.
- Giannestras NJ: Foot disorders: medical and surgical management, 2nd ed, Philadelphia, 1973, Lea & Febiger. Giannini S, Girolami M, Ceccarelli F: The surgical treatment of infantile fl at foot: a new expanding endo-orthotic implant, Ital J Orthop Trauma 11:315, 1985.
- Giladi, M, Milgrom C, Stein M, et al: The low arch, a protective factor in stress fractures, Orthop Rev 14:709, 1985.
- Golding-Bird CH: Operations on the tarsus in confi rmed fl at foot, Lancet 1:677, 1889.
- Greisberg J, Assal M, Hansen ST, et al: Isolated medial column stabilization improves alignment in adult-acquired fl atfoot, Clin Orthop Relat Res 435:197, 2005.
- Grice DS: An extraarticular arthrodesis of the subastragalar joint for correction of paralytic fl at feet in children, J Bone Joint Surg 34A:927, 1952.
- Grogan DP, Gasser SI, Ogden JA: The painful accessory navicular: a clinical and histopathological study, Foot Ankle 10:164, 1989.
- Guttmann G: Modifi cation of the Grice-Green subtalar arthrodesis in children, J Pediatr Orthop 1:219, 1981.
- Haddad SI, Myerson M, Pell RF, et al: Clinical and radiographic outcome of revision surgery for failed triple arthrodesis, Foot Ankle Int 18:489, 1997.
- Hadfi eld MH, Snyder JW, Liacouras PC, et al: Effects of medializing calcaneal osteotomy on Achilles tendon lengthening and plantar foot pressures, Foot Ankle Int 24:523, 2003.
- Harris RI, Beath T: Hypermobile fl at-foot with short tendo Achilles, J Bone Joint Surg 30A:116, 1948.
- Hirose CB, Johnson JE: Plantarfl exion opening wedge medial cuneiform osteotomy for correction of fi xed forefoot varus associated with fl atfoot deformity, Foot Ankle Int 25:568, 2004.
- Hogan MT, Staheli LT: Arch height and lower limb pain: an adult civilian study, Foot Ankle Int 23:43, 2002.
- Hoke M: An operation for the correction of extremely relaxed fl atfeet, J Bone Joint Surg 13:773, 1931.
- Howie CR, Fulford GE, Stewart K: A modifi ed technique for subtalar arthrodesis, J Bone Joint Surg 71B:533, 1989.
- Hsu LCS, Jaffray D, Leong JCY: The Batchelor-Grice extraarticular subtalar arthrodesis, J Bone Joint Surg 68B:125, 1986.
- Huang CK, Kitaoka HB, An KN, et al: Biomechanical evaluation of longitudinal arch stability, Foot Ankle 14:353, 1993.
- Jack EA: Naviculo-cuneiform fusion in the treatment of fl atfoot, J Bone Joint Surg 35B:75, 1953.
- Kidner FC: The prehallux (accessory scaphoid) in its relation to fl at-foot, J Bone Joint Surg 11:831, 1929.
- Kiter E, Erdag N, Karatosun V, et al: Tibialis posterior tendon abnormalities in feet with accessory navicular bone and fl atfoot, Acta Orthop Scand 70:618, 1999.
- Kiter E, Erduran M, Gunal I: Inheritance of the accessory navicular bone, Arch Orthop Trauma Surg 120:582, 2000.
- Kiter E, Gunal I, Turgut A, et al: Evaluation of simple excision in the treatment of symptomatic accessory navicular associated with fl at feet, J Orthop Sci 5:333, 2000.
- Kopp FJ, Marcus RE: Clinical outcome of surgical treatment of the symptomatic accessory navicular, Foot Ankle Int 25:27, 2004.
- Koutsogiannis E: Treatment of mobile fl at foot by displacement osteotomy of the calcaneus, J Bone Joint Surg 53B:96, 1971.
- Leonard MH, Gonzalez S, Breck LW, et al: Lateral transfer of the posterior tibial tendon in certain selected cases of pes plano valgus (Kidner operation), Clin Orthop Relat Res 40:139, 1965.
- MacNicol MF, Voutsinas S: Surgical treatment of the symptomatic accessory navicular, J Bone Joint Surg 66B:218, 1984.
- Malicky ES, Crary JL, Houghton MJ, et al: Talocalcaneal and subfi bular impingement in symptomatic fl atfoot in adults, J Bone Joint Surg 84A:2005, 2002.
- Malicky ES, Levine DS, Sangeorzan BJ: Modifi cation of the Kidner procedure with fusion of the primary and accessory navicular bones, Foot Ankle Int 20:53, 1999.
- McCall RE, Lillich JS, Harris JR, et al: The Grice extraarticular subtalar arthrodesis: a clinical review, J Pediatr Orthop 5:442, 1985.
- Michelson JD, Durant DM, McFarland E: The injury risk associated with pes planus in athletes, Foot Ankle Int 23:629, 2002.
- Miller OL: A plastic fl at-foot operation, J Bone Joint Surg 9:84, 1927.
- Miller TT, Staron RB, Feldman F, et al: The symptomatic accessory tarsal navicular bone: assessment with MR imaging, Radiology 195:849, 1995.
- Momberger N, Morgan JM, Bachus KN, et al: Calcaneocuboid joint pressure after lateral column lengthening in a cadaver planovalgus deformity model, Foot Ankle Int 21:730, 2000.
- Mosca VS: Calcaneal lengthening for valgus deformity of the hindfoot, J Bone Joint Surg 77A:500, 1995.
- Mosca VS: Flexible fl atfoot and skewfoot, Instr Course Lect 46:347, 1997.
- Nakayama S, Sugimoto K, Takakura Y, et al: Percutaneous drilling of symptomatic accessory navicular in young athletes, Am J Sports Med 33:531, 2005.
- Nyska M, Parks BG, Chu IT, et al: The contribution of the medial calcaneal osteotomy to the correction of fl atfoot deformities, Foot Ankle Int 22:278, 2001.
- Oloff LM, Naylor BL, Jacobs AM: Complications of
You Might Also Like
