Management of Ingrown Toenails & Nail Disorders
Key Takeaway
Onychocryptosis, or ingrown toenail, is a common orthopedic condition characterized by the penetration of the lateral nail plate into the adjacent nail fold. Management is dictated by clinical staging. Stage I is treated nonoperatively with packing and splinting, while Stage II and III lesions typically require surgical intervention, such as partial nail avulsion with chemical or surgical matrixectomy, to prevent recurrence and eradicate chronic granulation tissue.
DISORDERS OF NAILS AND SKIN
INTRODUCTION TO ONYCHOCRYPTOSIS
Onychocryptosis, commonly referred to as an ingrown toenail or unguis incarnatus, is a pervasive and frequently debilitating condition encountered in orthopedic and podiatric practice. It predominantly affects the great toe (hallux) and is characterized by the painful impingement and subsequent penetration of the lateral or medial edge of the nail plate into the adjacent soft tissue of the lateral nail fold. This mechanical breach initiates a cascade of foreign-body inflammatory responses, leading to localized erythema, edema, suppuration, and the eventual formation of hypertrophic granulation tissue.
While often dismissed as a minor ailment, neglected onychocryptosis can result in severe morbidity, chronic osteomyelitis of the distal phalanx, and significant functional impairment, particularly in diabetic or immunocompromised populations. Management must be strictly evidence-based, tailored to the clinical stage of the disease, and aimed at permanent eradication of the offending nail spicule while preserving the functional and aesthetic integrity of the hallux.
ANATOMY OF THE PERIONYCHIUM
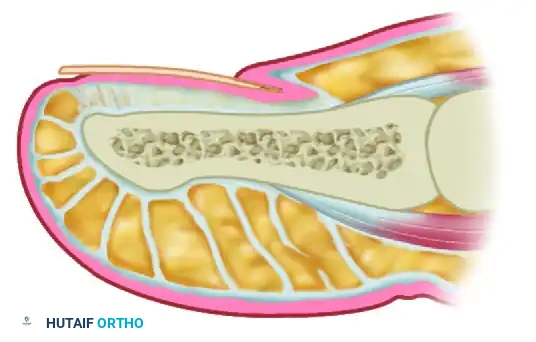
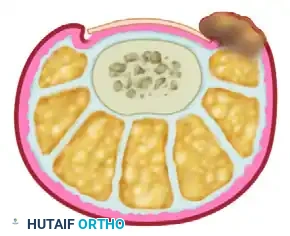
A profound understanding of the perionychial anatomy is the cornerstone of successful surgical intervention. The nail apparatus is a complex, specialized epidermal structure designed to protect the distal phalanx, enhance tactile sensation, and regulate peripheral hemodynamics.
The perionychium comprises the following distinct anatomical entities:
* Nail Plate: The hard, keratinized structure that spans the dorsum of the distal digit. It is produced primarily by the germinal matrix.
* Nail Bed: The highly vascular soft tissue beneath the nail plate, divided into two functional zones:
* Germinal Matrix: Located proximally, extending from the proximal nail fold to the lunula. It is responsible for 90% of nail plate generation. Failure to completely ablate the germinal matrix during surgical management is the primary cause of recurrence.
* Sterile Matrix: Extends from the lunula to the hyponychium. It provides strong adherence to the nail plate and contributes minimally to its thickness.
* Nail Folds: The cutaneous structures surrounding the nail plate, including the proximal nail fold (terminating in the eponychium/cuticle) and the lateral nail folds (paronychium).
* Hyponychium: The specialized epidermal junction between the distal nail bed and the volar skin of the digit, serving as a barrier against subungual infection.
Surgical Warning: The germinal matrix extends proximally beneath the eponychium for a distance of 5 to 8 mm. Surgical or chemical matrixectomy must reach this proximal recess to ensure complete ablation of the nail-forming tissue.
ETIOLOGY AND PATHOMECHANICS
The etiology of onychocryptosis is multifactorial, encompassing both extrinsic environmental factors and intrinsic anatomical predispositions.

Extrinsic Factors:
* Improper Nail Trimming: The most common precipitating factor. Trimming the nail too short or aggressively curving the corners allows the lateral nail fold to bulge over the truncated nail edge. As the nail grows, it pierces the overriding soft tissue.
* Constrictive Footwear: Tight, narrow toe-box shoes compress the lateral nail folds against the rigid nail plate, exacerbating impingement.
* Trauma: Direct microtrauma or macrotrauma to the hallux can alter the trajectory of nail growth or drive the nail plate into the paronychium.
Intrinsic Factors:
* Anatomical Variants: Pincer nails (excessive transverse curvature), abnormally wide nail plates, or disproportionately large lateral nail folds.
* Hyperhidrosis: Excessive sweating macerates the paronychial skin, decreasing its mechanical resistance to penetration by the nail plate.
Biomechanically, once the nail plate breaches the dermal barrier, the body mounts a robust foreign-body reaction. The resulting edema further exacerbates the mechanical impingement, creating a vicious cycle of inflammation, infection, and hypertrophic tissue proliferation.
CLINICAL STAGING
Treatment algorithms for onychocryptosis are dictated by the clinical stage of the disease, classically described by Heifetz and later modified by Mozena:
- Stage I (Inflammatory Stage): Characterized by mild erythema, slight edema, and pain with pressure along the lateral nail fold. The nail fold remains intact, and there is no purulent drainage or granulation tissue.
- Stage II (Abscess Stage): The nail plate has breached the dermis. Symptoms escalate to severe pain, significant erythema, and the presence of seropurulent or purulent drainage. The lateral nail fold bulges over the nail plate.
- Stage III (Granulation Stage): Chronic inflammation leads to the formation of exuberant, hypertrophic granulation tissue that covers the lateral nail fold and inhibits free drainage. If left untreated, epithelium creeps over the edge of the granulations, precluding any chance of elevating the nail edge nonoperatively.
NONOPERATIVE MANAGEMENT
Nonoperative management is the first-line treatment for Stage I and early Stage II lesions. The primary objective is to separate the offending nail plate from the inflamed paronychial soft tissue, allowing the dermal breach to heal while the nail grows out distally.
Nail Packing and Elevation
This technique aims to physically lift the embedded nail edge from its position in the dermis of the lateral nail fold.

- Technique: This is easier to perform if done after soaking the foot in warm water (often with Epsom salts or mild antiseptic), which makes the nail softer and more pliable. Nonabsorbent cotton, wool, or acrylic mesh is passed beneath the corner of the nail.
- Application: This must be done gently, as it is frequently painful. The patient may require a few days of intermittent warm soaks, a cutout shoe, and modification of activity before the local inflammation is reduced enough to allow this treatment.
- Maintenance: Once begun, the patient usually can introduce more material beneath the nail corner daily. The treatment is repeated until the nail grows out past the hyponychium and can be trimmed properly. This treatment is usually successful in 2 to 3 weeks if patient compliance is maintained.
Proper Trimming Techniques
Patient education regarding proper nail trimming is paramount to prevent recurrence. The goal is a squared nail with corners protruding distal to the hyponychium.

Proper trimming: The nail is cut straight across at right angles to the distal edge of the nail plate.

Improper trimming: Aggressive curving of the corners allows the soft tissue to override the nail.

Improper trimming: Cutting the nail too short predisposes the distal corners to embed into the paronychium as they grow.
Splinting and Orthonyxia
- Gutter Splints: Another conservative treatment option is nail splinting, which separates the nail plate from the soft tissue to provide a channel in which the nail can grow. A "gutter splint" can be fashioned from a sterilized vinyl intravenous drip infusion tube, slit from top to bottom with one end cut diagonally for smooth insertion. It is affixed to the ingrown nail edge with adhesive tape or a formable acrylic resin (e.g., cyanoacrylate). Reported recurrence rates with various splinting techniques range from 8% to 48%.
- Orthonyxia: A dynamic correction technique that uses direct force (via specialized wires or braces glued to the nail plate) to lift the nail from the nail fold, gradually flattening the transverse curvature of the nail and releasing pressure on the inflamed soft tissue.
OPERATIVE MANAGEMENT
In Stage III, and in many patients in Stage II, surgical management is preferred. Nonsurgical management of late Stage II and Stage III lesions is time-consuming, patient compliance is unpredictable, and recurrence is highly likely. The presence of epithelialized granulation tissue physically blocks drainage and prevents conservative elevation of the nail.
Preoperative Preparation and Anesthesia
The recommended anesthetic is a local digital block using 1% or 2% lidocaine or mepivacaine without epinephrine.
Clinical Pearl: While recent literature suggests that epinephrine can be safe in digital blocks for healthy patients, traditional orthopedic teaching for hallux procedures involving infected or compromised tissue still advocates for plain local anesthetic to eliminate any risk of digital ischemia.
- Injection Technique: The anesthetic is introduced with a small-gauge (25G or 27G) needle approximately 1 cm distal to the first web space. Ensure that the plantar digital nerves and the dorsal sensory branches of the superficial peroneal nerve are well anesthetized. A V-shaped or ring block technique is highly effective.
- Hemostasis: A sterile Penrose drain or a commercial digital tourniquet is applied to the base of the hallux to provide a bloodless surgical field, which is critical for visualizing the germinal matrix.
Surgical Technique 1: Partial Nail Avulsion with Chemical Matrixectomy
This is the gold standard for most Stage II and Stage III ingrown toenails due to its high success rate (>90%) and minimal postoperative morbidity.
- Preparation: Following anesthesia and exsanguination, the toe is prepped and draped in a standard sterile fashion.
- Nail Elevation: A Freer elevator or a specialized nail spatula is introduced beneath the lateral quarter of the nail plate. The elevator is advanced proximally to the eponychial fold, gently separating the nail plate from the underlying sterile and germinal matrix.
- Nail Resection: An English anvil nail splitter or straight tissue scissors are used to make a longitudinal cut through the nail plate, approximately 3 to 4 mm from the lateral edge. The cut must extend completely under the eponychium to the proximal edge of the nail root.
- Avulsion: The freed lateral sliver of nail is grasped with a straight hemostat. Using a gentle "roll and pull" motion toward the midline of the toe, the nail spicule is avulsed. It is imperative to inspect the extracted spicule to ensure the feathery proximal edge is intact, confirming no retained fragments.
- Granulation Tissue Debridement: Hypertrophic granulation tissue is aggressively curetted or sharply excised to promote healing and restore the normal contour of the nail fold.
- Chemical Matrixectomy: The surgical field is dried meticulously with sterile cotton-tipped applicators. An applicator soaked in 89% liquid phenol is introduced into the proximal nail fold, directly contacting the germinal matrix.
- Application Time: The phenol is applied for three consecutive 30-second intervals (total 90 seconds).
- Neutralization: The area is immediately flushed with isopropyl alcohol or copious saline to neutralize the phenol and prevent collateral chemical burns to the surrounding healthy tissue.
- Dressing: The tourniquet is removed, and hyperemia is confirmed. A non-adherent dressing (e.g., Adaptic or Xeroform) is applied, followed by sterile gauze and a compressive wrap.
Surgical Technique 2: Winograd Procedure (Wedge Resection)
The Winograd procedure is indicated for severe Stage III lesions with massive hypertrophy of the lateral nail fold, or when chemical matrixectomy is contraindicated or has previously failed.
- Incision: A longitudinal incision is made through the nail plate and nail bed, approximately 4 mm from the affected margin, extending proximally through the eponychium.
- Wedge Excision: A second, elliptical incision is made in the hypertrophic lateral nail fold, connecting with the proximal and distal extents of the first incision.
- Tissue Removal: The entire wedge of tissue—comprising the lateral nail plate, the underlying sterile and germinal matrix, and the hypertrophic paronychial skin—is excised sharply down to the periosteum of the distal phalanx.
- Matrix Eradication: The proximal recess is meticulously inspected. Any remaining germinal matrix (which appears as distinct, pearly-white tissue) is sharply excised or curetted to prevent spicule recurrence.
- Closure: The wound margins are approximated using non-absorbable sutures (e.g., 3-0 or 4-0 Nylon). The sutures are passed through the remaining nail plate and the lateral skin flap, drawing the skin edge tightly against the cut edge of the nail.
- Postoperative Care: Sutures are typically removed at 10 to 14 days.
Pitfall: Failure to carry the wedge excision deep enough to the periosteum or far enough proximally under the eponychial fold will leave retained germinal matrix cells, leading to a painful recurrent nail spicule (often termed a "recurrence cyst").
POSTOPERATIVE PROTOCOL
- Immediate Care: The patient is instructed to keep the foot elevated above heart level for the first 24 to 48 hours to minimize throbbing pain and edema.
- Wound Management: For chemical matrixectomies, the initial bulky dressing is removed after 24 hours. The patient begins daily warm water and Epsom salt soaks, followed by the application of a topical antibiotic ointment and a simple adhesive bandage. Serous drainage is expected for 2 to 4 weeks post-phenolization due to the chemical burn.
- Activity Modification: Weight-bearing as tolerated in a stiff-soled, open-toe surgical shoe is permitted immediately. Return to athletic footwear and vigorous activity is typically allowed once drainage ceases and tenderness resolves (usually 2 to 3 weeks).
DYSTROPHIC NAILS AND OTHER LESIONS
While onychocryptosis is the most common nail pathology, orthopedic surgeons must be adept at recognizing and managing other perionychial lesions.
Dystrophic Nails (Onychogryposis, Onychomycosis)
Onychogryposis ("ram's horn nail") involves massive, asymmetrical hypertrophy of the nail plate, often secondary to chronic trauma, peripheral vascular disease, or neglect. Onychomycosis is a fungal infection leading to thickened, brittle, and discolored nails. When conservative measures (e.g., mechanical debridement, oral antifungals) fail, total nail avulsion with complete surgical matrixectomy (Zadik procedure) or terminal Syme amputation may be indicated for definitive relief.
Subungual Exostosis
A benign osteocartilaginous tumor arising from the dorsal aspect of the distal phalanx. It presents as a painful, firm subungual mass that elevates and deforms the nail plate. Radiographs confirm the diagnosis. Treatment requires partial or total nail avulsion followed by complete marginal excision of the exostosis down to normal cancellous bone.
Subungual and Periungual Fibromas
Benign fibrous lesions that can distort the nail matrix. Koenen tumors (periungual fibromas) are pathognomonic for Tuberous Sclerosis. Surgical excision must be meticulous to avoid iatrogenic damage to the germinal matrix, which would result in permanent nail dystrophy.
Glomus Tumor
A rare, benign hamartoma of the neuromyoarterial glomus body, classically presenting with the triad of severe paroxysmal pain, point tenderness, and cold hypersensitivity. It often appears as a small, bluish discoloration beneath the nail plate. MRI is the imaging modality of choice. Treatment is complete surgical excision via a transungual approach, which is curative and provides immediate pain relief.
Malignant Melanoma
Subungual melanoma is a rare but potentially fatal malignancy. It frequently presents as Hutchinson's sign (periungual extension of brown/black pigmentation) or a longitudinal melanonychia that widens over time. Any suspicious, changing, or non-healing subungual pigmented lesion mandates an urgent full-thickness biopsy. Definitive treatment typically involves amputation at the interphalangeal or metatarsophalangeal joint, depending on the depth of invasion.
📚 Medical References
- : principles of non-operative and operative care, Clin Orthop Relat Res 142:96, 1979.
- Murtagh J: Patient education: ingrowing toenails, Aust Fam Physician 22:206, 1993.
- Ney GC: An operation for ingrowing toe nails, JAMA 80:374, 1923.
- O’Donoghue DH: Treatment of ingrown toe nail, Am J Surg 50:519, 1940.
- Pearson HJ, Bury RN, Wapples J, et al: Ingrowing toenails: is there a nail abnormality? J Bone Joint Surg 69B:840, 1987.
- Persichetti P, Simone P, Vecchi GL, et al: Wedge excision of the nail fold in the treatment of ingrown toenail, Ann Plast Surg 52:617, 2004.
- Pettine KA, Cofi eld RH, Johnson KA, et al: Ingrown toenail: results of surgical treatment, Foot Ankle 9:130, 1988.
- Quenu P: Des limites de la matrice de l’ongle incarné: applications au traitement de l’ongle incarné, Bull Mém Soc Chir 13:255, 1887.
- Rounding C, Bloomfi eld S: Surgical treatments for ingrowing toenails, Cochrane Database Syst Rev 18:CD001541, 2005.
- Samman PD: The human toe nail: its genesis and blood supply, Br J Dermatol 71:296, 1959.
- Scott P: Ingrown toenails, Med J Aust 1:48, 1968.
- Siegle RJ, Stewart R: Recalcitrant ingrowing nails: surgical approaches, J Dermatol Surg Oncol 18:744, 1992.
- South DA, Farber EM: Urea ointment in the nonsurgical avulsion of nail dystrophies: a reappraisal, Cutis 25:609, 1980.
- Stilwell G: On the treatment of ingrowing toe-nail, BMJ 1872.
- Thompson TC, Terwilliger C: The terminal Syme operation for ingrowing toenail, Surg Clin North Am 31:575, 1951.
- Tomczak RL: Embryology of the nail unit. In Myerson MS, ed: Foot and ankle disorders, Philadelphia, 2000, Saunders. Townsend AC, Scott PR: Ingrowing toenail and onychogryposis, J Bone Joint Surg 48B:354, 1966.
- Watson-Cheyne W, Burghard FF: A manual of surgical treatment, London, 1912, Longmans, Green. Wilson TE: Treatment of ingrowing toenails, Med J Aust 2:33, 1944.
- Winograd AM: A modifi cation in the technique of operation for ingrown toe-nail, JAMA 92:229, 1929.
- Wright G: Laser matricectomy in the toes, Foot Ankle 9:246, 1989.
- Zadik FR: Obliteration of the nail bed of the great toe without shortening the terminal phalanx, J Bone Joint Surg 32B:66, 1950.
- Zaias N: The nail in health and disease, New York, 1980, SP Medical & Scientifi c Books. Zook EG, Van Beek AL, Russell RC, et al: Anatomy and physiology of the perionychium: a review of the literature and anatomic study, J Hand Surg 5:528, 1980.
- Zuber TJ, Pfenninger JL: Management of ingrown toenails, Am Fam Physician 52:181, 1995.
You Might Also Like