Advanced Magnetic Resonance Imaging in Orthopaedics: Safety Protocols, Contraindications, and Foot & Ankle Pathologies
Key Takeaway
Magnetic Resonance Imaging (MRI) is a cornerstone of orthopaedic diagnostics, particularly for complex foot and ankle pathologies. However, strict adherence to safety protocols regarding metallic implants and devices is mandatory. This guide details absolute and relative MRI contraindications, optimal imaging techniques, and the clinical evaluation of tendinopathies, ligamentous injuries, and osteomyelitis to guide precise surgical interventions.
MAGNETIC RESONANCE IMAGING IN ORTHOPAEDICS: SAFETY AND CONTRAINDICATIONS
Magnetic Resonance Imaging (MRI) has revolutionized the diagnostic algorithm in orthopaedic surgery, offering unparalleled soft-tissue contrast and early detection of osseous abnormalities. However, the powerful magnetic fields (B0) and radiofrequency (RF) pulses utilized during image acquisition pose significant risks to patients with specific implanted devices or foreign bodies. A rigorous screening protocol is mandatory prior to any MRI examination.
Absolute Contraindications
Certain patients are strictly precluded from undergoing MRI due to the risk of catastrophic device malfunction, thermal injury, or catastrophic displacement of ferromagnetic objects. Absolute contraindications include:
* Intracerebral Aneurysm Clips: Unless explicitly documented as MRI-safe (e.g., titanium variants), older ferromagnetic clips can undergo torque and displacement, leading to fatal hemorrhage.
* Cardiac Pacemakers and Automatic Implantable Cardioverter-Defibrillators (AICDs): The magnetic field can induce erratic pacing, switch the device to an asynchronous mode, or deplete the battery. (Note: Some modern devices are "MR Conditional," requiring strict cardiology oversight and specific scanner settings).
* Biostimulators and Implanted Infusion Devices: Devices such as spinal cord stimulators or insulin pumps may malfunction or induce thermal burns at the electrode tips.
* Internal Hearing Aids (Cochlear Implants): The magnetic field can demagnetize the internal magnet or cause displacement.
* Metallic Orbital Foreign Bodies: Even microscopic ferromagnetic shards can rotate or translate, causing irreversible optic nerve or retinal damage. Pre-MRI orbital radiographs are mandatory for patients with a history of sheet metal work.
Relative Contraindications and Orthopaedic Hardware
Cardiac valve prostheses, contrary to historical belief, can generally be scanned safely, as the torque exerted by the magnetic field is negligible compared to the pulsatile forces of the heart. Relative contraindications include first-trimester pregnancy (due to theoretical risks of RF tissue heating and acoustic noise to the fetus), middle ear prostheses, and penile prostheses.
Clinical Pearl: Generally, internal orthopaedic hardware (e.g., titanium or stainless steel plates, screws, and intramedullary nails) and joint arthroplasty prostheses are safe to scan. However, ferrous metals create significant local magnetic susceptibility artifacts that can obscure adjacent tissues.
While metal prostheses may become warm during the examination due to RF-induced currents, this is rarely noticed by the patient and almost never requires termination of the study.
External Fixation Devices: Patients with metallic external fixation devices should not be scanned. The frame can act as an antenna, leading to severe induction heating and full-thickness thermal burns at the pin-tract interfaces. If there is any ambiguity regarding the MRI compatibility of an implantable device, the manufacturer's guidelines must be consulted directly.
PRINCIPLES OF FOOT AND ANKLE MRI
The foot and ankle constitute a highly complex anatomical region. The intricate biomechanics of the midfoot and hindfoot articulations, combined with a dense network of tendons, ligaments, and retinacula, make clinical and imaging evaluation challenging.
Most MRI examinations of the foot and ankle are indicated for the evaluation of tendinopathy, occult articular disorders, and osseous pathological conditions, frequently following trauma. However, MRI should be utilized to solve specific clinical dilemmas; it should not be used as a screening study for non-specific pain, as the diagnostic yield in such scenarios is exceedingly low.
Technical Optimization
Given the small size of the anatomical structures, optimal imaging requires specific technical parameters:
* Field Strength: A high-field-strength magnet (> 1.0 Tesla, optimally 1.5 T or 3.0 T) is mandatory to achieve an adequate signal-to-noise ratio (SNR).
* Coil Selection: The use of a dedicated surface coil, typically an extremity or "boot" coil, is non-negotiable.
* Field of View (FOV): The clinical presentation should direct the examination specifically toward the forefoot, midfoot, or hindfoot/ankle. This arbitrary division allows for a sufficiently small FOV (8 to 12 cm), which is critical for generating high-resolution images.
* Sequences: Images are prescribed in orthogonal or oblique planes. A standard protocol includes a combination of T1-weighted (excellent for anatomical detail and marrow evaluation), T2-weighted, and fat-suppressed sequences (e.g., STIR or T2 Fat-Sat, which are highly sensitive for edema and fluid).
Surgical Warning - The Magic Angle Artifact: Tendons oriented at approximately 55 degrees to the main magnetic field (B0) may exhibit falsely increased signal intensity on short TE sequences (T1, PD), mimicking tendinopathy or partial tears. This is particularly relevant for the peroneal tendons as they curve around the lateral malleolus. Evaluation on T2-weighted sequences (where the artifact disappears) is essential for accurate diagnosis.
TENDON INJURIES AND SURGICAL MANAGEMENT
MRI excels in the evaluation of pathological conditions affecting the numerous tendons traversing the ankle joint. The most commonly affected are the calcaneal (Achilles) and posterior tibial tendons.
The Calcaneal (Achilles) Tendon
In chronic tendinosis, the calcaneal tendon thickens and loses its normal flat or concave anterior contour, becoming oval or circular in cross-section. The enlarged tendon typically maintains a low signal on all sequences due to the lack of acute inflammation, representing mucoid degeneration.
When partially torn, the tendon demonstrates focal or fusiform thickening with interspersed areas of edema or hemorrhage, which appear hyperintense (bright) on T2-weighted series. With a complete rupture, there is a distinct discontinuity of the tendon fibers, often with a fluid-filled gap and retraction of the proximal stump.
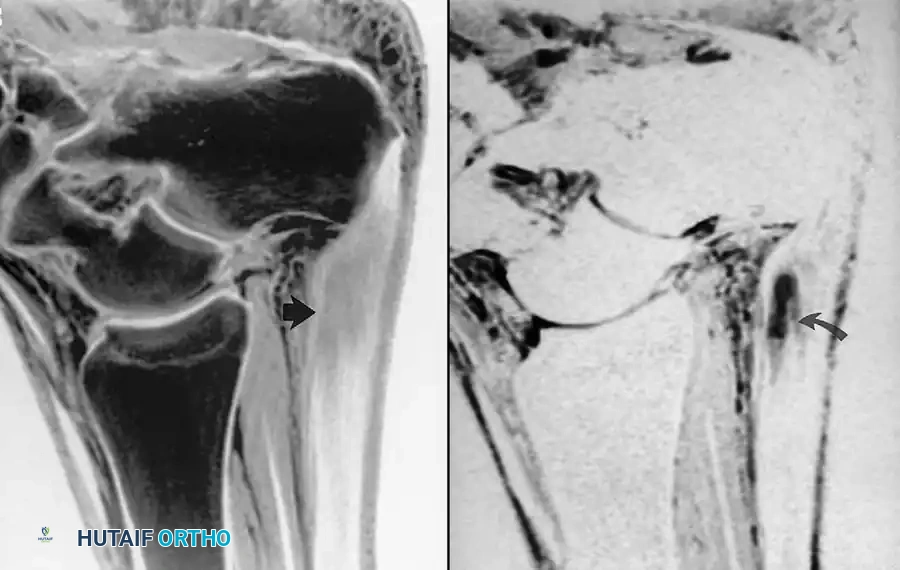
Fig. 2-2 Partial tear of calcaneal tendon. A, Sagittal T1-weighted image shows markedly thickened calcaneal tendon containing areas of intermediate signal. B, Sagittal fat-suppressed, T2-weighted image exhibits fluid within tendon substance, indicating partial tear.
Surgical Approach to Achilles Tendon Rupture
- Indications: Acute complete ruptures in active patients, or chronic ruptures with significant functional deficit.
- Positioning: Prone, with the feet hanging over the edge of the operating table to assess resting equinus.
- Incision: A posteromedial longitudinal incision is preferred to avoid the sural nerve, which crosses from medial to lateral in the proximal third of the calf.
- Technique: The paratenon is meticulously incised and preserved for later closure (crucial for gliding and vascularity). The ruptured ends are debrided. A heavy, non-absorbable suture (e.g., #2 FiberWire) is woven through both stumps using a locking Krackow technique. The ankle is placed in slight plantar flexion (equinus) to approximate the ends without tension, and the sutures are tied.
- Postoperative Protocol: The patient is placed in a non-weight-bearing equinus splint for 2 weeks, followed by a functional rehabilitation boot with heel wedges, progressively decreasing the equinus angle over 6-8 weeks.
The Posterior Tibial Tendon (PTT)
Abnormalities of the PTT, the primary dynamic stabilizer of the medial longitudinal arch, can be diagnosed confidently with MRI. Increased fluid in the tendon sheath indicates tenosynovitis. As posterior tibial tendon dysfunction (PTTD) progresses, the tendon can appear thickened (Stage II), attenuated, or completely discontinuous (Stage III).
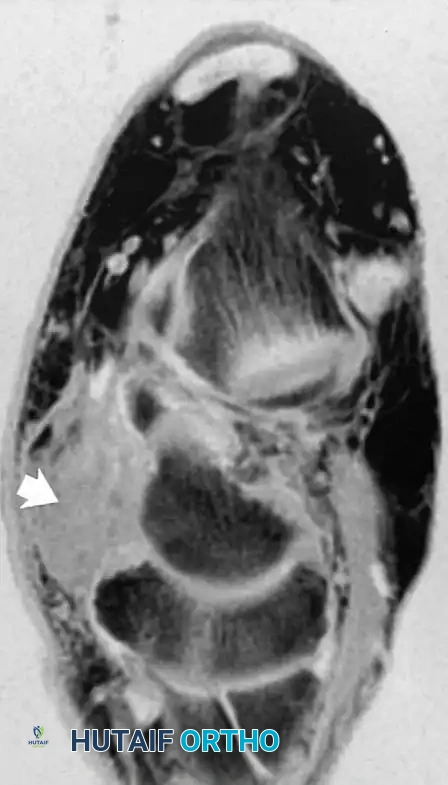
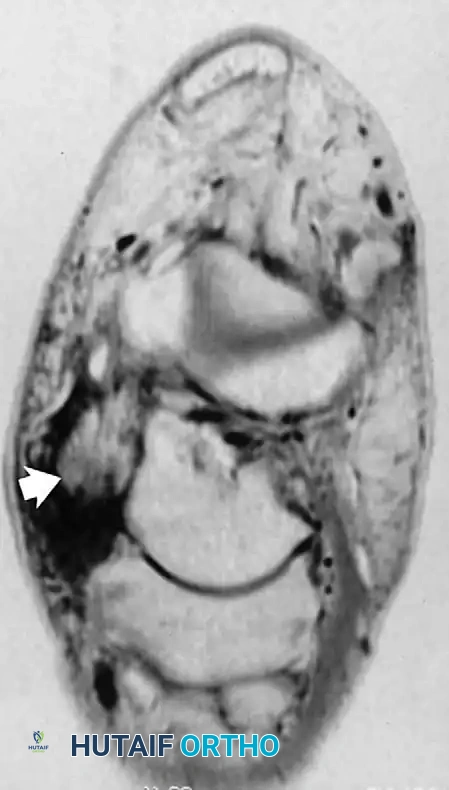
Fig. 2-3 Posterior tibial tendon tear. A, Axial T1-weighted image reveals swollen, ill-defined region of intermediate signal intensity, representing fluid and abnormal tendon. B, Axial fat-suppressed, T2-weighted image shows thickened tendon surrounded by hyperintense fluid.
Surgical Approach to PTT Dysfunction (Stage II)
- Indications: Flexible flatfoot deformity with a diseased, non-functional PTT that has failed conservative management.
- Technique: A medial incision is made over the PTT to the navicular. The diseased PTT is debrided. The Flexor Digitorum Longus (FDL) tendon is harvested and transferred into a drill hole in the navicular, secured with a biotenodesis screw. To protect the transfer and correct the biomechanical axis, a Medial Displacement Calcaneal Osteotomy (MDCO) is routinely performed via a separate lateral approach.
The Peroneal Tendons
Occasionally, similar abnormalities are seen in the flexor tendons or the peroneus longus and brevis tendons. Peroneal tendinopathy often presents with lateral ankle pain and can be associated with superior peroneal retinaculum (SPR) incompetence, leading to subluxation.
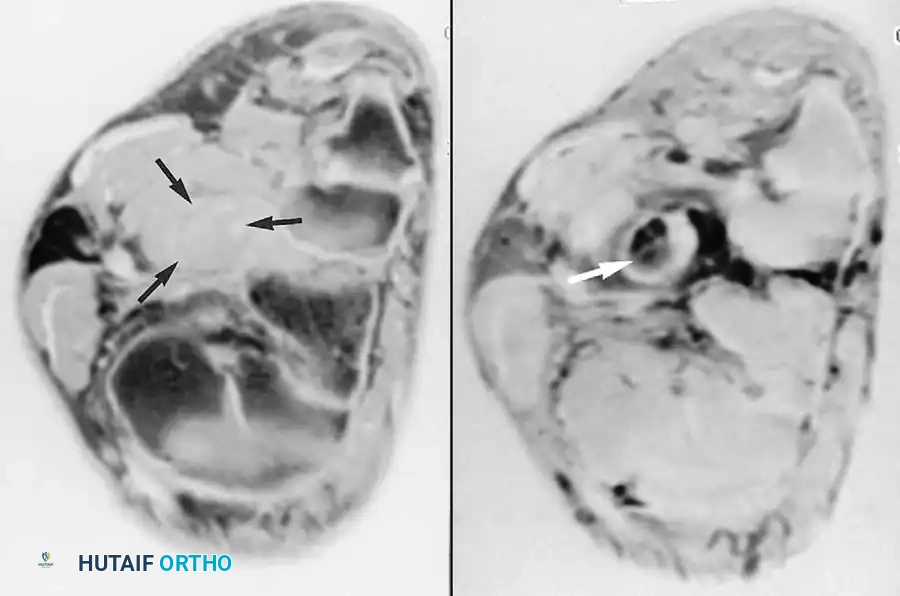
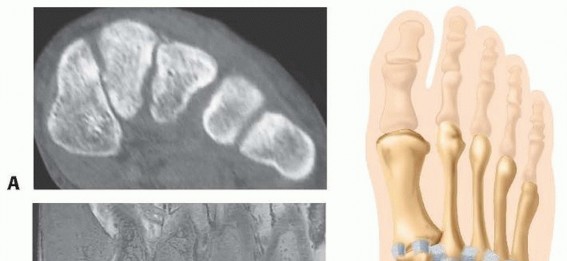
Fig. 2-4 Peroneus longus tendon rupture. A, Coronal T1-weighted image through midfoot shows increased diameter of peroneus longus tendon. B, Coronal fat-suppressed, T2-weighted image reveals fluid signal within ruptured tendon.
LIGAMENT INJURIES AND IMPINGEMENT SYNDROMES
Although ligamentous injuries around the ankle (e.g., anterior talofibular ligament [ATFL] and calcaneofibular ligament [CFL] sprains) are exceedingly common, MRI has a limited role in their acute evaluation. The medial (deltoid) and lateral stabilizing ligaments of the tibiotalar and talocalcaneal joints, as well as the distal tibiofibular syndesmotic ligaments, can usually be visualized with proper positioning.
However, the imaging status of ligaments around the ankle rarely changes the acute treatment algorithm, which remains functionally based in most patients.
Where MRI proves highly valuable is in evaluating the lateral recess of the ankle joint in patients with chronic ankle sprains and anterolateral impingement syndrome. Regions of hypertrophic fibrosis (often termed a "meniscoid lesion") are frequently seen in the lateral gutter, especially when fluid is present in the joint. These patients often benefit from arthroscopic debridement of the lateral gutter.
OSSEOUS AND ARTICULAR DISORDERS
As elsewhere in the body, bone marrow disorders, occult fractures, and osteochondral injuries are exquisitely delineated by MRI.
Osteonecrosis of the Talus
The talus is highly susceptible to avascular necrosis (osteonecrosis) following talar neck fractures due to its tenuous retrograde blood supply. MRI is the most sensitive modality for detecting early ischemic changes in the marrow.
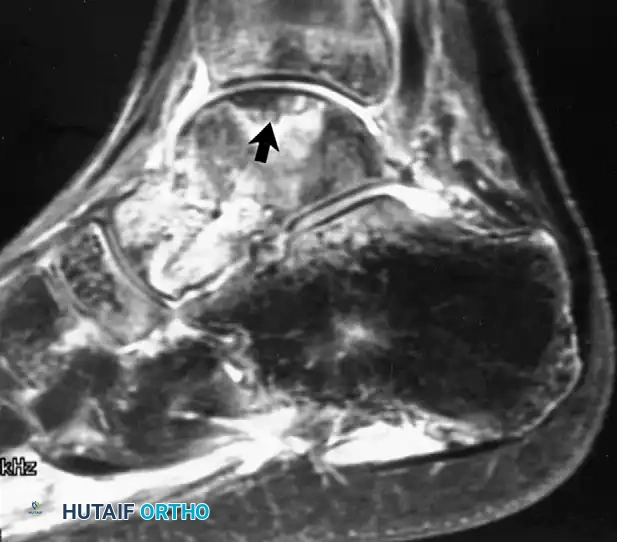
Fig. 2-5 Osteonecrosis of talus. Fat-suppressed proton density–weighted image reveals focus of abnormal signal in talar dome after fracture of talar neck.
Surgical Management of Talar Osteonecrosis
- Early Stage: Core decompression may be attempted to reduce intraosseous pressure and stimulate angiogenesis.
- Late Stage (Collapse): If the talar dome collapses, joint-sparing procedures (e.g., vascularized bone grafts from the distal radius or medial femoral condyle) or salvage procedures (tibiotalocalcaneal arthrodesis) are indicated.
Osteochondral Lesions
Osteochondral lesions of the talus (OCLT) are well evaluated on MRI, which can assess the stability of the fragment. Fluid signal interposing between the osteochondral fragment and the native bone bed on T2-weighted images is a hallmark sign of instability, necessitating surgical intervention (e.g., arthroscopic bone marrow stimulation/microfracture or osteochondral autograft transfer).
SOFT TISSUE MASSES AND NEUROPATHIC COMPLICATIONS
The excellent anatomical information provided by MRI allows for the precise detection and definition of masses in the foot.
Morton Neuroma
One mass unique to the foot is a Morton neuroma, a perineural fibrosis of the common digital nerve. Usually found in the third metatarsal interspace distally, it is most often a clinical diagnosis based on the presence of pain on the plantar surface, exacerbated by lateral compression of the forefoot (Mulder's click).
In contrast to most other tumors or inflammatory masses, a Morton neuroma typically lacks increased signal on T2-weighted sequences, appearing as a teardrop-shaped intermediate-to-low signal mass. If conservative measures (wide toe-box shoes, corticosteroid injections) fail, surgical excision via a dorsal approach is highly effective. The dorsal approach avoids a painful plantar scar, though it requires division of the deep transverse metatarsal ligament to access the neuroma.
The Diabetic Foot and Osteomyelitis
Another condition for which MRI is exceptionally well-suited is the evaluation of infection in the foot of a diabetic patient. Differentiating between acute osteomyelitis and neuropathic (Charcot) arthropathy is one of the most challenging clinical scenarios in orthopaedics.
Because of its excellent depiction of bone marrow edema, MRI can detect osteomyelitis early—perhaps 7 to 10 days before radiographic abnormalities (such as periosteal reaction or focal osteopenia) become visible.
Clinical Pearl: While the diabetic foot can be a diagnostic challenge, a completely normal MRI marrow signal confidently excludes osteomyelitis.
The anatomical information provided by MRI assists in surgical planning by defining the exact extent of marrow involvement. However, marrow edema alone can be non-specific, as it is also present in acute Charcot arthropathy. Therefore, the current workup of osteomyelitis in a diabetic foot often involves a combination of MRI, advanced scintigraphy (e.g., Indium-111 labeled white blood cell scans), laboratory data (ESR, CRP), and rigorous physical examination (the "probe-to-bone" test).
For the evaluation of surrounding soft-tissue infection, MRI is the modality of choice. The addition of intravenous gadolinium contrast-enhanced sequences is highly helpful in defining non-enhancing fluid collections (abscesses) and devascularized or gangrenous tissue that require urgent surgical debridement.
Surgical Principles in Diabetic Foot Infections
- Incision and Drainage: Abscesses identified on MRI must be aggressively debrided.
- Bone Resection: If osteomyelitis is confirmed, the infected bone must be resected to bleeding, healthy margins.
- Microbiology: Deep bone biopsies must be sent for aerobic, anaerobic, and fungal cultures prior to the initiation of empiric antibiotics to ensure targeted antimicrobial therapy.
- Postoperative Care: Meticulous wound care, offloading (e.g., Total Contact Casting once the infection is cleared), and strict glycemic control are paramount to prevent recurrence and avoid major limb amputation.
You Might Also Like