Congenital Hallux Varus: Pathomechanics & Surgical Management

Key Takeaway
Congenital hallux varus is a rare pediatric foot deformity characterized by medial angulation of the great toe at the metatarsophalangeal joint. Pathogenesis typically involves a rudimentary accessory toe and a taut fibrous band acting as a bowstring. Surgical management is dictated by deformity severity and soft tissue rigidity, utilizing techniques such as the Farmer syndactyly procedure, Kelikian reconstruction, or arthrodesis for arthritic complications.
Introduction to Congenital Hallux Varus
Congenital hallux varus is a rare, complex structural deformity of the pediatric foot characterized by a medial angulation of the great toe at the metatarsophalangeal (MTP) joint. Unlike acquired hallux varus, which is most frequently an iatrogenic complication following overzealous surgical correction of hallux valgus, the congenital variant is deeply rooted in embryological maldevelopment.
It is imperative for the orthopedic surgeon to distinguish congenital hallux varus from varus deformity of the first metatarsal (metatarsus primus varus). In metatarsus primus varus, the first metatarsal itself is medially deviated, but the MTP joint remains congruous and undeformed. In true congenital hallux varus, the primary pathology lies at the MTP articulation, with the varus deformity of the toe varying in severity from a mild medial deviation of a few degrees to a rigid, 90-degree medial angulation.
Clinical Pearl: Always differentiate congenital hallux varus from metatarsus adductus and metatarsus primus varus. A rigid medial deviation at the MTP joint with a palpable medial fibrous band is the hallmark of congenital hallux varus.
Pathoanatomy and Biomechanics
Congenital hallux varus is typically unilateral and is frequently associated with a constellation of specific anatomical anomalies. Understanding these associations is critical for comprehensive preoperative planning. The condition is commonly linked with one or more of the following:
- A short, thick first metatarsal: This alters the biomechanical lever arm of the first ray, contributing to forefoot instability and altered weight-bearing mechanics.
- Accessory bones or toes (Preaxial Polydactyly): Remnants of duplicated digits are frequently present.
- Varus deformity of the lateral metatarsals: One or more of the four lateral metatarsals may exhibit a varus alignment, complicating the overall forefoot geometry.
- A firm, unyielding fibrous band: This band extends from the medial aspect of the great toe to the base of the first metatarsal.
The "Bowstring" Pathogenesis
The widely accepted embryological explanation for this anomaly is an incomplete duplication of the first ray. In utero, two great toes begin to originate (preaxial polydactyly); however, the medial or accessory toe fails to fully develop.
As fetal development progresses, this rudimentary medial toe, combined with its associated dysplastic fibrous tissue, forms a rigid medial tether. This structure acts exactly like a taut bowstring. As the more fully developed, dominant great toe grows, the unyielding medial fibrous band gradually pulls it into a progressive varus position. Over time, the medial capsule of the MTP joint contractures, and the lateral capsule attenuates, leading to a rigid, fixed deformity by the time of birth or early infancy.
Clinical and Radiographic Evaluation
Clinical Presentation
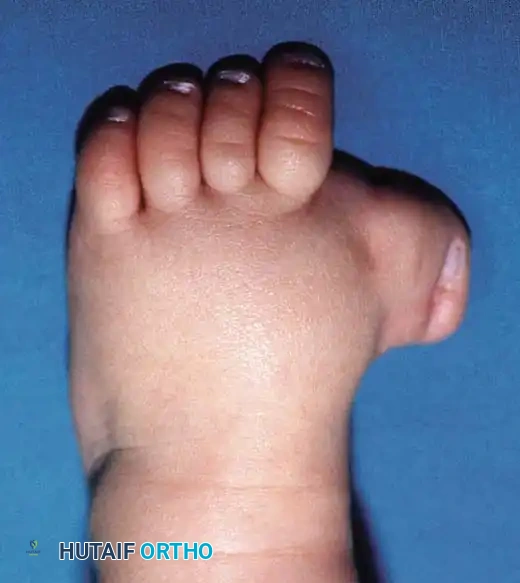
Patients typically present in infancy or early childhood. Parents often report difficulty with shoe wear and a noticeable cosmetic deformity. On physical examination, the great toe is medially deviated. The examiner must assess the flexibility of the MTP joint. In mild cases, the deformity may be passively correctable; in severe cases, it is rigidly fixed.
Palpation along the medial border of the first ray will often reveal the taut fibrous band. The length of the first metatarsal should be clinically compared to the lesser metatarsals.
Preoperative clinical photograph demonstrating severe congenital hallux varus with a rigid medial deviation of the great toe and associated soft tissue contractures.
Radiographic Assessment
Standard weight-bearing (or simulated weight-bearing in infants) anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory.
Key Radiographic Findings:
* Medial subluxation or dislocation of the proximal phalanx on the first metatarsal head.
* A shortened and widened first metatarsal.
* Presence of accessory ossicles, delta phalanges, or rudimentary accessory digits medially.
* Evaluation of the intermetatarsal angle and the alignment of the lesser metatarsals.
Anteroposterior radiograph of a right foot with congenital hallux varus. Note the exceptionally short first metatarsal and the presence of an accessory distal phalanx acting as a medial tether.
Surgical Management Strategies
The proper treatment for congenital hallux varus is entirely dependent on the severity of the deformity, the rigidity of the contracted soft structures, and the age of the patient. Non-operative management (stretching, taping, or casting) is generally ineffective due to the rigid, tethering nature of the medial fibrous band.
Indications for Surgery
- Progressive deformity interfering with ambulation.
- Inability to accommodate the foot in standard footwear.
- Pain associated with callosities or impending MTP joint arthrosis in older children.
1. The Farmer Technique (Creation of Syndactyly)
The Farmer technique is highly effective for correcting mild to moderate deformities where the first metatarsal length is adequate, but soft tissue tethering is the primary deforming force. The procedure involves a comprehensive medial soft tissue release combined with the creation of a syndactyly between the first and second toes to maintain alignment.
Preoperative Preparation and Positioning:
* The patient is placed supine on the operating table.
* A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field.
* Loupe magnification is recommended for meticulous soft tissue handling and protection of neurovascular bundles.
Step-by-Step Surgical Technique (Farmer):
- Flap Design and Elevation:
Raise a broad, Y-shaped flap of skin and subcutaneous tissue from the dorsal surface of the web space between the first and second toes. The base of this flap must be positioned dorsally in the space between the first and second metatarsals. The flap should include the skin contiguous with the web distally along the two toes for approximately one-third of their length. - Medial Approach and Capsulotomy:
From the medial edge of the base of the flap, curve the incision medially and slightly distally across the medial aspect of the first MTP joint. Deepen this incision transversely through the medial part of the capsule of the first MTP joint. - Release of the Bowstring:
Identify and completely excise the firm fibrous band extending from the medial side of the great toe to the base of the first metatarsal. This is the critical step to release the tethering force. - Excision of Accessory Structures:
Through a separate dorsomedial incision (or by extending the current exposure), meticulously excise any accessory phalanx, rudimentary toe remnants, or hypertrophic soft tissue from the medial aspect of the great toe. - Creation of Syndactyly:
Move the great toe laterally, bringing it into direct apposition against the second toe. Create a surgical syndactyly between these two toes by suturing the apposing skin edges together using interrupted non-absorbable sutures (e.g., 4-0 or 5-0 nylon). This syndactyly acts as a dynamic biological tether to prevent recurrent varus drift. - Skeletal Stabilization:
To maintain the corrected alignment during soft tissue healing, insert a smooth, longitudinal Kirschner wire (K-wire) retrograde from the tip of the great toe, across the interphalangeal and MTP joints, and into the medullary canal of the first metatarsal. Ensure the toe is pinned in a neutral position (0 degrees of varus/valgus, and neutral dorsiflexion). - Flap Transposition and Closure:
Swing the previously raised Y-shaped flap of skin and subcutaneous tissue medially. Suture it into place to cover the soft tissue defect created on the dorsal and medial aspects of the first MTP joint following the correction of the toe.
Surgical Warning: In an alternative technique described by Farmer, the Y-shaped flap is raised from the plantar surface of the foot. The remainder of the procedure is identical, with the flap swung medially. If any residual defect cannot be closed without tension, it must be left open to heal by secondary intention or covered with a full-thickness skin graft to prevent ischemic necrosis of the flap.
2. The Kelikian Procedure for Severe Deformity
For severe, rigid deformities, particularly those complicated by an excessively short first metatarsal, the Farmer technique may be insufficient. The operation described by Kelikian et al. is indicated in these complex scenarios. This procedure involves a more aggressive skeletal and soft tissue reconstruction, often creating an artificial syndactyly and utilizing extensive capsular releases to centralize the digit over the deficient metatarsal.
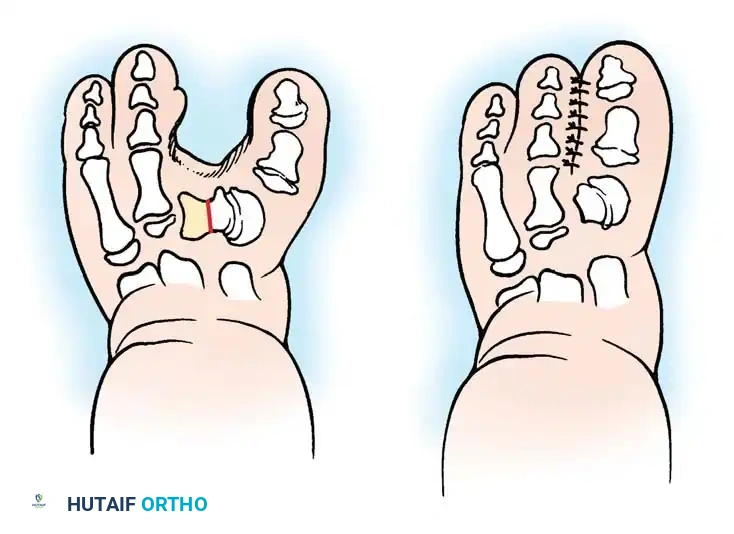
Diagrammatic representation of the Kelikian procedure for congenital hallux varus. A, Preoperative appearance demonstrating severe varus and a shortened first ray. B, Postoperative appearance after extensive medial release and the creation of an artificial syndactyly to maintain alignment.
The Kelikian approach emphasizes the complete mobilization of the MTP joint, resection of all medial tethering structures (including the abductor hallucis insertion if severely contracted), and the surgical fusion of the soft tissues of the first and second toes to provide a lateralizing force vector that counteracts the innate varus tendency.
3. Salvage Procedures: Arthrodesis and Amputation
Metatarsophalangeal Arthrodesis:
If the congenital hallux varus deformity has been neglected and is now complicated by severe, painful traumatic arthritis of the MTP joint, soft tissue reconstruction alone will fail to relieve pain. In these instances, arthrodesis of the first MTP joint is the procedure of choice.
* Positioning for Arthrodesis: The joint must be fused in approximately 10 to 15 degrees of valgus and 10 to 15 degrees of dorsiflexion relative to the first metatarsal to allow for a normal rollover phase during the gait cycle.
Amputation:
In exceedingly rare cases where the deformity is so grotesque and rigid that it is impossible to correct via soft tissue reconstruction, and the bone stock is too deficient to undergo a functional arthrodesis, amputation of the rudimentary or severely deformed ray may be indicated to allow the patient to wear standard footwear and ambulate without pain.
Adjunctive Soft Tissue Procedures and Comparative Techniques
When addressing pediatric toe deformities, the principles of soft tissue release and capsulotomy share commonalities across different digits. For instance, the Butler arthroplasty, classically utilized for the correction of an overriding or adducted fifth toe, employs a double racquet incision and extensive capsular release that conceptually mirrors the aggressive soft tissue mobilization required in hallux varus correction.
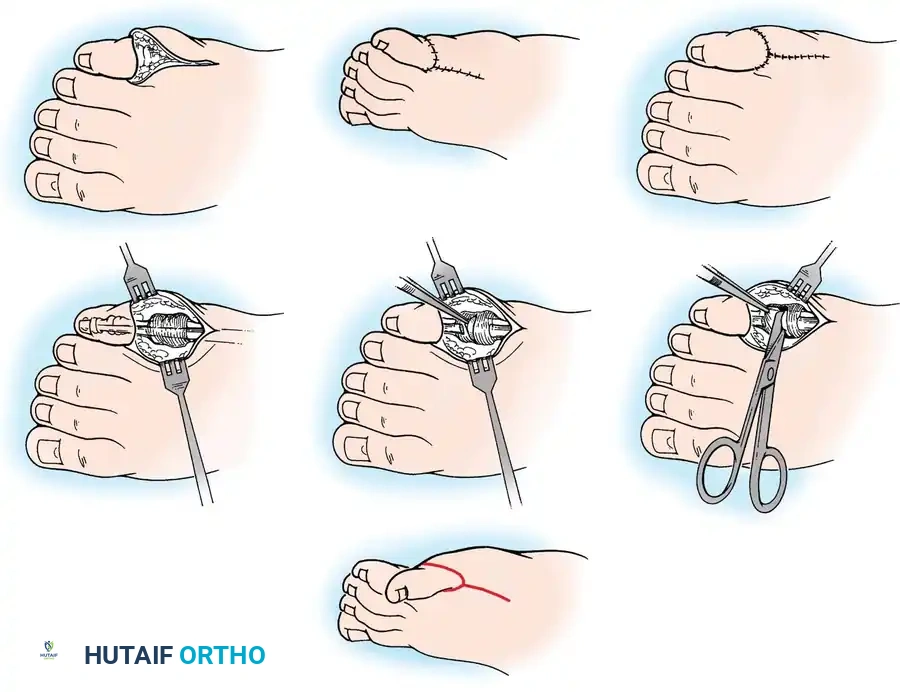
Butler arthroplasty principles. A, Double racquet incision. B, Exposure of extensor tendon. C, Transection of extensor tendon. D, Separation of adherent capsule. E, Corrected position of toe. F and G, Skin closure. While primarily for the fifth toe, the principles of circumferential capsular release and tendon lengthening are highly applicable to the medial releases required in severe hallux varus.
Understanding these parallel techniques allows the orthopedic surgeon to adapt flap designs and capsular releases based on the specific intraoperative soft tissue tension encountered during hallux varus reconstruction.
Postoperative Protocol and Rehabilitation
Meticulous postoperative care is as critical as the surgical execution to prevent recurrence and ensure optimal functional outcomes.
- Immediate Postoperative Phase:
The foot is immobilized in a well-padded, short-leg cast extending beyond the toes to protect the K-wire and the soft tissue reconstruction. The limb should be elevated strictly for the first 48 to 72 hours to minimize edema and protect flap viability. - Weight-Bearing Status:
The patient is kept strictly non-weight-bearing on the operative extremity. In young children, this may require the use of a wheelchair or specialized pediatric mobility aids. - Pin and Cast Removal:
At exactly 6 weeks postoperatively, the cast is bivalved and removed in the clinic. The longitudinal K-wire is extracted. Radiographs are obtained to confirm the maintenance of joint congruity and alignment. - Rehabilitation:
Following pin removal, full weight-bearing activities are gradually allowed as tolerated. Parents are instructed on passive range-of-motion exercises for the MTP joint (if not arthrodesed) to prevent severe stiffness. Wide-toe-box footwear is recommended to prevent any extrinsic medializing pressure on the great toe.

Anteroposterior radiograph demonstrating the appearance after surgical correction. The medial tether has been excised, the MTP joint is centralized, and the alignment of the first ray is restored to a functional, neutral position.
Complications and Pitfalls
Surgeons undertaking the correction of congenital hallux varus must be prepared to manage several potential complications:
- Recurrence of Deformity: The most common complication, usually resulting from an incomplete release of the medial fibrous band or failure to recognize and excise an accessory ossicle.
- Flap Necrosis: Excessive tension on the transposed Y-flap or aggressive dissection compromising its vascular base can lead to marginal or complete flap necrosis. If tension is noted intraoperatively, the surgeon must immediately pivot to using a full-thickness skin graft.
- MTP Joint Stiffness: Extensive capsulotomies inevitably lead to some degree of joint fibrosis. While a stiff, straight toe is functionally superior to a deformed one, parents must be counseled preoperatively regarding the expected loss of terminal MTP motion.
- Neurovascular Injury: The medial plantar digital nerve is at high risk during the excision of the fibrous band. Meticulous blunt dissection and loupe magnification are essential to prevent painful neuroma formation.
Conclusion
Congenital hallux varus is a challenging pediatric foot deformity that demands a thorough understanding of its unique pathoanatomy—specifically the bowstring effect of the medial fibrous band and associated accessory structures. Surgical intervention is almost universally required. By employing meticulous soft tissue releases, such as the Farmer syndactyly technique or the Kelikian procedure for more severe presentations, the orthopedic surgeon can successfully restore a plantigrade, functional, and cosmetically acceptable foot, allowing the child to achieve normal developmental milestones and pain-free ambulation.
📚 Medical References
- Congenital hallux varus, Am J Surg 95:274, 1958.
- Greiss ME, Williams DH: Macrodystrophia lipomatosis in the foot: a case report and review of the literature, Arch Orthop Trauma Surg 110:220, 1991.
- Grogan DP, Bernstein RM, Habal MB, et al: Congenital lipofi bromatosis associated with macrodactyly of the foot, Foot Ankle 12:40, 1991.
- Hamer AJ, Stanley D, Smith TW: Surgery for the curly toe deformity: a double-blind, randomised, prospective trial, J Bone Joint Surg 75B:662, 1993.
- Hubbard AM, Davidson RS, Meyer JS, et al: Magnetic resonance imaging of skewfoot, J Bone Joint Surg 78A:389, 1996.
- Kalen V, Burwell DS, Omer GE: Macrodactyly of the hands and feet, J Pediatr Orthop 8:311, 1988.
- Kelikian H, Clayton L, Loseff H: Surgical syndactylia of the toes, Clin Orthop 19:209, 1961.
- Kotwal PP, Farooque M: Macrodactyly, J Bone Joint Surg 80B:651, 1998.
- Kovalsky E, Guttmann GG: Early surgical correction of unilateral cleft foot deformity, Orthopedics 13:348, 1990.
- Lapidus PW: Transplantation of the extensor tendon for correction of the overlapping fi fth toe, J Bone Joint Surg 24:555, 1942.
- Lenke LG, Schoenecker PL, Gilula LA: Imaging rounds no. 105, Orthop Rev 20:295, 1991.
- Leonard MH, Rising EE: Syndactylization to maintain correction of overlapping fi fth toe, Clin Orthop Relat Res 43:241, 1965.
- Meyerding HW, Upshaw JE: Heredofamilial cleft foot deformity (lobster-claw or splitfoot), Am J Surg 74:889, 1947.
- Nakamura K, Ohara K, Ohta E: A new surgical technique for postaxial polydactyly of the foot, Plast Reconstr Surg 97:133, 1996.
- Thompson TC: Surgical treatment of disorders of the fore part of the foot, J Bone Joint Surg 46A:1117, 1964.
- Thordarson DB: Congenital crossover fi fth toe correction with soft tissue release and cutaneous Z-plasty, Foot Ankle Int 22:511, 2001.
- Topoleski TA, Ganel A, Grogan DP: Effect of proximal phalangeal epiphysiodesis in the treatment of macrodactyly, Foot Ankle Int 18:500, 1997.
- Venn-Watson EA: Problems in polydactyly of the foot, Orthop Clin North Am 7:909, 1976.
- Weaver KM, Henry GW, Reinker KA: Unilateral duplication of the great toe with anterolateral tibial bowing, J Pediatr Orthop 16:73, 1996.
- Wood VE, Peppers TA, Shook J: Cleft-foot closure: a simplifi ed technique and review of the literature. J Pediatr Orthop 17:501, 1997.
- [Anomalies of the Foot
Congenital](https://pubmed.ncbi.nlm.nih.gov/?term=Anomalies%20of%20the%20Foot%0A%0ACongenital)
You Might Also Like


