Brachymetatarsia: Surgical Lengthening & Distraction Osteogenesis
Key Takeaway
Brachymetatarsia is a congenital or acquired condition characterized by an abnormally short metatarsal, most frequently affecting the fourth ray. This disrupts the normal metatarsal parabola, leading to altered forefoot biomechanics, transfer metatarsalgia, and cosmetic concerns. Surgical management primarily involves metatarsal lengthening via distraction osteogenesis or single-stage interpositional bone grafting. Distraction osteogenesis allows for gradual soft tissue adaptation and significant length restoration while minimizing neurovascular compromise.
INTRODUCTION AND PATHOANATOMY
Brachymetatarsia is a structural anomaly characterized by the abnormal shortening of one or more metatarsals. This condition most frequently involves the fourth ray, followed in incidence by the first and fifth rays. While it can present bilaterally, it exhibits a strong female predilection (up to a 25:1 female-to-male ratio).
The etiology is most commonly congenital, stemming from the premature closure of the metatarsal epiphyseal plate. However, acquired forms may result from trauma, infection, radiation, or iatrogenic causes. Systemic conditions associated with multiple brachymetatarsia include Turner syndrome, Down syndrome, pseudohypoparathyroidism, and pseudo-pseudohypoparathyroidism.
The primary consequence of a shortened metatarsal is the disruption of the normal weight-bearing mechanics of the forefoot. The affected ray fails to participate adequately in the terminal stance phase of gait, leading to the transfer of ground reaction forces to the adjacent, normal-length metatarsal heads. This biomechanical shift frequently results in transfer metatarsalgia, intractable plantar keratoses (calluses), and dorsal soft-tissue contractures that cause the affected toe to subluxate dorsally, creating a "floating toe" deformity.
BIOMECHANICS AND RADIOGRAPHIC EVALUATION
A thorough understanding of forefoot biomechanics is essential for preoperative planning. The metatarsal heads normally form a smooth, parabolic arc (the Maestro curve), which ensures an even distribution of plantar pressures during the propulsive phase of gait.
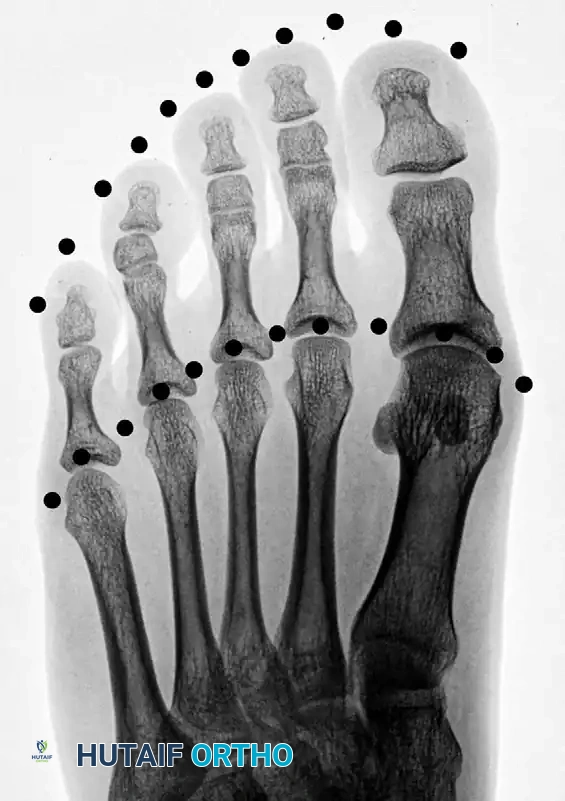
Radiographic evaluation requires standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. On the AP radiograph, the normal metatarsal parabola can be traced to identify the exact degree of shortening.
Figure 1: Normal toe-tip and metatarsal head parabolas (dotted lines), demonstrating the ideal geometric arc required for optimal forefoot biomechanics.
When brachymetatarsia is present, this parabolic arc is severely disrupted. The distance required to restore the affected metatarsal head to the ideal parabola dictates the surgical lengthening goal.

Figure 2: Disruption of the normal parabolic arc associated with brachymetatarsia of the first metatarsal.
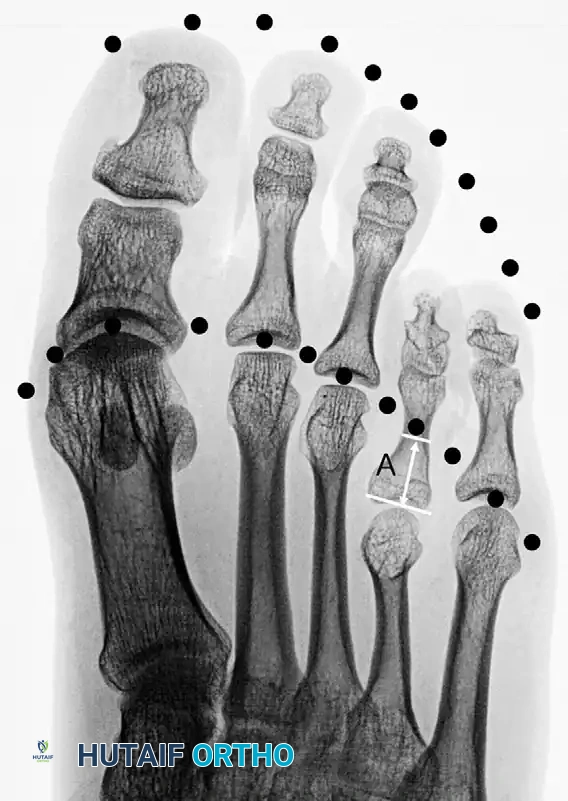
Figure 3: Disruption with brachymetatarsia of the fourth metatarsal. The distance marked “A” represents the precise length needed to obtain an ideal parabola.
Clinical Pearl: When calculating the required lengthening distance, always account for the soft tissue envelope. Lengthening a metatarsal by more than 40% of its original length significantly increases the risk of neurovascular compromise, severe joint stiffness, and MTP joint subluxation.
CONCURRENT FOREFOOT PATHOLOGIES: FREIBERG INFRACTION
When evaluating a patient with forefoot pain and altered metatarsal mechanics, the differential diagnosis must include avascular necrosis of the metatarsal head, known as Freiberg infraction. While distinct from brachymetatarsia, Freiberg disease similarly disrupts the articular mechanics of the lesser rays and can be exacerbated by abnormal stress distributions in the forefoot. It most commonly affects the second metatarsal head but can present atypically.

Figure 4: Freiberg infraction presenting in an uncommon location.

Figure 5: Three years following joint débridement and remodeling of the metatarsal head. While motion remains limited, the patient is highly active and asymptomatic.
Systemic factors, such as hemoglobinopathies, can predispose patients to multifocal osteonecrosis in the forefoot.

Figure 6: Freiberg infraction of the third metatarsal head in a teenage girl (arrow).

Figure 7: One year later, the second metatarsal head is also involved. Arrows indicate Freiberg infractions on both the second and third metatarsal heads in a patient with a known hemoglobinopathy.
SURGICAL MANAGEMENT STRATEGIES
The indications for surgical intervention in brachymetatarsia include intractable transfer metatarsalgia, difficulty with footwear due to dorsal toe subluxation, and severe psychological distress related to the cosmetic deformity.
Surgical options are broadly categorized into two techniques:
1. One-Stage Lengthening with Interpositional Bone Grafting
2. Gradual Lengthening via Distraction Osteogenesis (Callotasis)
One-Stage Lengthening with Interpositional Graft
One-stage lengthening is generally reserved for mild deformities where the required lengthening is less than 10 to 15 mm. Attempting acute lengthening beyond this threshold places excessive tension on the neurovascular bundles, risking digital ischemia and severe soft tissue contracture.
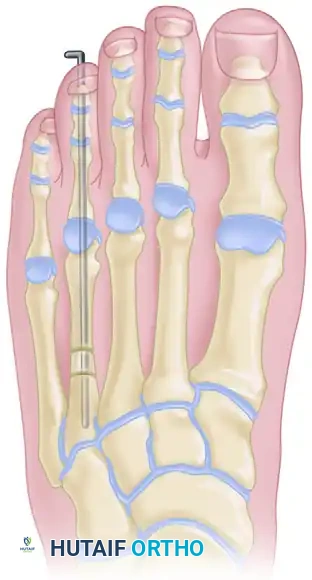
Figure 8: Lengthening of the metatarsal utilizing a one-stage allograft interposition technique. Rigid internal fixation (typically with a plate or intramedullary K-wire) is required to stabilize the intercalary graft.
Distraction Osteogenesis (Callotasis)
For lengthening requirements exceeding 15 mm (or >40% of the native bone length), distraction osteogenesis is the gold standard. This technique, based on Ilizarov principles, allows for the gradual adaptation of the bone, skin, tendons, and neurovascular structures, significantly reducing the risk of acute ischemic complications.
SURGICAL TECHNIQUE: DISTRACTION OSTEOGENESIS FOR METATARSAL LENGTHENING (LEE ET AL.)
The following technique details the application of a unilateral external fixator for gradual metatarsal lengthening. Meticulous pin placement and a low-energy corticotomy are paramount to the success of this procedure.
Preoperative Preparation and Positioning
- Position the patient supine on a radiolucent operating table.
- Administer regional anesthesia (popliteal block) or general anesthesia.
- Apply a calf tourniquet to ensure a bloodless surgical field.
- Position the fluoroscopy unit (C-arm) to allow for unobstructed AP and lateral views of the forefoot.
Pin Insertion Principles
Under strict fluoroscopic guidance, the goal is to insert two mini-Schanz half-pins into the proximal metaphysis and two into the distal metaphysis of the affected metatarsal.
For First Metatarsal Brachymetatarsia:
* Utilize 3.0 mm diameter mini-Schanz pins.
* Direct the distal pins from medial to lateral to avoid the extensor hallucis longus (EHL) tendon dorsally and the sesamoid apparatus plantarly.
* Apply the unilateral external fixator to the medial aspect of the first metatarsal.
* Ensure the fixator is positioned as parallel to the plantar surface of the foot as possible in the transverse plane. This prevents plantarflexion or dorsiflexion malalignment during the distraction phase.
For Fourth Metatarsal Brachymetatarsia:
* Utilize 2.0 mm diameter mini-Schanz pins due to the smaller diaphyseal diameter.
* Insert the pins on the dorsolateral aspect of the fourth metatarsal.
* Surgical Warning: Extreme care must be taken to avoid entrapping the extensor digitorum longus (EDL) tendon to the fifth toe.
* Technique Pearl: Position the proximal two pins lateral to the fifth EDL tendon, and position the two distal pins medial to it. This strategic placement creates a safe corridor that prevents tendon tethering during lengthening.
Fixator Alignment
Proper alignment of the external fixator rail is the most critical step in preventing axial deviation during the lengthening process.
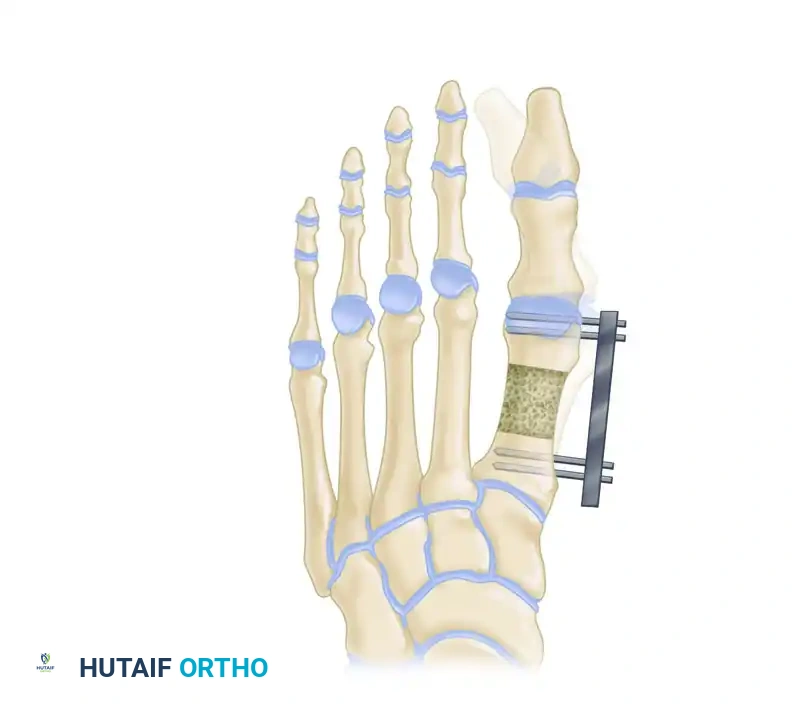
Figure 9: External fixator application in the transverse plane. The fixator must be applied as parallel as possible to the axis of the second metatarsal to ensure a straight longitudinal distraction.

Figure 10: External fixator application in the sagittal plane. The rail must be parallel to the plantar surface of the foot to prevent iatrogenic elevation or depression of the metatarsal head.
The Corticotomy
- Make a 1.5-cm longitudinal incision directly over the metatarsal shaft, centered between the proximal and distal pin clusters.
- Carefully dissect down to the bone, retracting the extensor tendons.
- Longitudinally incise the periosteum and elevate it meticulously. Preserving the periosteal sleeve is vital for robust callus formation.
- Perform the corticotomy. Using a motorized sagittal saw with continuous saline cooling, make a transverse cut perpendicular to the plantar surface of the foot.
> Surgical Warning: Thermal necrosis from the saw blade will destroy the osteogenic potential of the bone ends, leading to delayed union or nonunion. Copious irrigation during sawing is mandatory. Alternatively, a multiple drill-hole and osteotome technique can be utilized to minimize thermal injury. - Once the osteotomy is complete, confirm the proper direction of metatarsal lengthening by acutely distracting the osteotomy approximately 5 mm.
- Assess the direction of the distraction under fluoroscopy to ensure there is no angular or translational deformity.
- After confirmation, restore the bone surfaces to complete apposition (zero distraction) to begin the latency phase.
- Close the periosteum with fine absorbable sutures, followed by standard skin closure.
POSTOPERATIVE CARE AND REHABILITATION PROTOCOL
The success of distraction osteogenesis relies heavily on strict adherence to the postoperative protocol, which is divided into three distinct phases: Latency, Distraction, and Consolidation.
1. Latency Phase
- Duration: 7 days postoperatively.
- Purpose: Allows for the resolution of acute surgical inflammation and the initiation of the early fracture healing cascade (hematoma organization and mesenchymal stem cell migration). No distraction is performed during this week.
- Weight-bearing: Full weight-bearing, heel-touch ambulation utilizing a rigid postoperative shoe is permitted beginning on the second day after surgery.
2. Distraction Phase
- Rate and Rhythm: Beginning on postoperative day 8, distraction is initiated at a rate of 0.25 mm three times daily (totaling 0.75 mm per day).
- Monitoring: The distraction rate and rhythm are not static; they must be titrated according to radiographic findings and the patient’s clinical tolerance.
- Radiographic Follow-up: Radiographs are obtained every other week to evaluate the quality of the regenerate bone (osteogenesis) and to monitor the adjacent metatarsophalangeal (MTP) joint for signs of subluxation.
- Endpoint: Distraction is continued until a satisfactory parabola incorporating all five metatarsal heads has been achieved. Over-lengthening must be strictly avoided to prevent excessive stiffness.
3. Consolidation Phase
- Once the desired length is achieved, the distraction is halted. The external fixator is locked and left in place to act as a neutralization device while the regenerate bone mineralizes.
- Fixator Removal: The external fixator is removed only when radiographs demonstrate mature, tricortical callus bridging the distraction gap. This typically takes twice as long as the distraction phase (a consolidation index of roughly 30-40 days per centimeter of lengthening).
- Following fixator removal, the patient is transitioned to a stiff-soled shoe or walking boot for an additional 2 to 4 weeks to protect the newly formed bone from bending forces.
COMPLICATIONS AND PITFALLS
While highly effective, distraction osteogenesis for brachymetatarsia carries a distinct complication profile:
- Pin Tract Infections: The most common complication. Managed with aggressive local pin care (chlorhexidine or saline) and oral antibiotics. Intravenous antibiotics or pin removal are rarely necessary unless osteomyelitis develops.
- MTP Joint Subluxation: As the metatarsal lengthens, tension on the long flexor and extensor tendons increases, which can drive the MTP joint into dorsal subluxation or dislocation. Prevention: Some surgeons advocate for prophylactic pinning of the MTP joint with a K-wire during the distraction phase.
- Axial Deviation: Usually plantarflexion or dorsiflexion of the distal fragment due to improper fixator alignment or asymmetric muscle pull. Requires early identification on bi-weekly radiographs and potential adjustment of the fixator.
- Premature Consolidation: Occurs if the distraction rate is too slow or the latency period is too long. May require a return to the operating room to re-cut the bone.
- Delayed Union / Nonunion: Occurs if the distraction rate is too fast, or if the periosteum/endosteal blood supply was severely damaged during the corticotomy. Managed by temporarily compressing the fixator ("accordion technique") to stimulate osteogenesis, or ultimately, bone grafting.
You Might Also Like


