Revision Anterior Cruciate Ligament Reconstruction: Principles, Planning, and Surgical Execution

Key Takeaway
Revision anterior cruciate ligament (ACL) reconstruction is a complex salvage procedure necessitated by primary graft failure. Successful outcomes depend on meticulous preoperative planning, accurate identification of the failure etiology, and precise surgical execution. This guide details the biomechanical principles, indications for single-stage versus two-stage revisions, hardware management, and evidence-based graft selection strategies essential for orthopedic surgeons managing recurrent knee instability and restoring optimal joint kinematics.
INTRODUCTION TO REVISION ANTERIOR CRUCIATE LIGAMENT SURGERY
The incidence of primary anterior cruciate ligament (ACL) reconstruction failure has become an increasingly prevalent challenge in orthopedic sports medicine. Recent epidemiological reports suggest a broad failure rate ranging from 10% to 25% following primary ACL reconstruction. However, establishing an accurate and universally accepted failure rate remains difficult because the clinical definition of "failure" is highly variable. When utilizing the strict criterion of recurrent symptomatic instability secondary to structural graft failure, the incidence is estimated to occur in 0.7% to 8% of primary reconstructions.
Revision anterior cruciate ligament surgery is inherently more complex than primary reconstruction. It demands a comprehensive understanding of knee biomechanics, meticulous preoperative planning, and advanced surgical proficiency. The orthopedic surgeon must navigate compromised soft tissue envelopes, altered osseous anatomy, retained fixation hardware, and the potential for concurrent meniscal or chondral deficiencies. The primary objective of revision surgery is not merely to replace the torn graft, but to systematically identify and correct the underlying cause of the index failure to prevent a catastrophic recurrence.
ETIOLOGY OF PRIMARY ACL RECONSTRUCTION FAILURE
Determining the precise cause of primary ACL reconstruction failure is the most critical step in the preoperative evaluation. Failure is rarely multifactorial, and a systematic approach is required to categorize the etiology into technical, biological, or traumatic domains.
Chronology of Failure
The timing of graft failure provides vital diagnostic clues regarding its etiology:
* Early Failure (< 6 months): Failures occurring within the first six months postoperatively are predominantly iatrogenic or rehabilitation-related. Common causes include gross technical errors (e.g., severe tunnel malposition), overly aggressive or non-compliant rehabilitation, premature return to high-demand pivoting sports, or a fundamental failure of biological graft incorporation.
* Late Failure (> 1 year): Failures occurring after the first year of reconstruction are more typically the result of a new, significant traumatic event. Once the graft has undergone complete "ligamentization" and remodeling, its failure biomechanics closely mirror those of a native ACL.
Technical Errors
Surgical technique remains the most common—and most avoidable—cause of primary ACL reconstruction failure.
Surgical Pitfall: Femoral tunnel malposition is the single most frequent technical error leading to graft failure. A femoral tunnel placed too anteriorly results in a graft that is excessively tight in flexion and lax in extension, leading to restricted range of motion and eventual graft stretching or rupture. A tunnel placed too vertically (high in the notch) fails to control rotational laxity, resulting in a persistent pivot-shift phenomenon despite a negative Lachman test.
Other technical errors include:
* Inadequate Notchplasty: Failure to adequately clear the intercondylar notch can lead to graft impingement against the lateral femoral condyle or the roof of the notch during terminal extension, causing mechanical attrition and eventual rupture.
* Improper Graft Tensioning: Securing the graft in excessive tension can lead to joint capture and articular cartilage degeneration, while inadequate tensioning results in persistent clinical laxity.
* Fixation Failure: Loss of fixation before biological incorporation occurs can result from poor bone quality, improper hardware sizing, or divergent interference screw placement.
Biological and Anatomic Factors
Biological failures encompass issues with graft incorporation, such as delayed ligamentization, localized osteolysis, or subclinical indolent infections. Furthermore, failure to recognize and address concurrent injuries to secondary restraints—such as the anterolateral ligament (ALL), posterolateral corner (PLC), or medial collateral ligament (MCL)—places disproportionate biomechanical stress on the central ACL graft, inevitably leading to premature attenuation.
PREOPERATIVE EVALUATION AND IMAGING
A detailed history and physical examination are paramount. The surgeon must obtain all previous operative notes to determine the type of graft used, the fixation methods employed, and any concomitant procedures performed during the index surgery.
Advanced Imaging Modalities
Standard weight-bearing radiographs (AP, lateral, Rosenberg, and Merchant views) are essential to assess joint space narrowing, lower extremity alignment, and the position of retained hardware. Magnetic Resonance Imaging (MRI) is utilized to evaluate the integrity of the primary graft, the status of the menisci, and the condition of the articular cartilage.
However, Computed Tomography (CT) is the gold standard for evaluating bone tunnel anatomy in the revision setting.
FIGURE 45-127: High-resolution CT scan with multiplanar reconstruction used to determine the exact location, trajectory, and size of existing bone tunnels before anterior cruciate ligament revision.
CT imaging allows the surgeon to accurately measure tunnel widening (osteolysis) and determine if the existing tunnels are anatomically placed. This dictates whether the old tunnels can be reused, if new tunnels must be drilled divergently, or if a staged bone-grafting procedure is mandatory.
INDICATIONS FOR STAGED REVISION SURGERY
The decision to perform a single-stage versus a two-stage revision is one of the most critical decision-making nodes in revision ACL surgery.
Management of Arthrofibrosis and Motion Deficits
Staged revision surgery must be strongly considered if the patient presents with significant preoperative motion deficits. Specifically, a lack of 5 degrees of terminal extension or less than 120 degrees of flexion (a 20-degree deficit from normal) precludes immediate revision. In these scenarios, the first stage consists of aggressive arthroscopic lysis of adhesions, notchplasty, and hardware removal, followed by intensive physical therapy to restore full range of motion before the actual graft revision is attempted.
Management of Bone Defects and Tunnel Widening
The presence of massive osteolysis or severe tunnel malposition that intersects the planned anatomic trajectory necessitates a two-stage approach.
Clinical Pearl: As recommended by Harner et al., a staged bone grafting procedure is indicated if the existing bone tunnel exceeds 15 mm in diameter. Attempting to place a new graft into a massively widened tunnel compromises fixation and invites recurrent failure.
During the first stage, existing hardware is removed, the sclerotic tunnel walls are aggressively debrided to bleeding cancellous bone, and the defects are packed with autograft or allograft bone (e.g., cancellous chips, dowels, or synthetic bone substitutes). The second stage (definitive ACL reconstruction) is delayed for 4 to 6 months to allow for complete radiographic and clinical consolidation of the bone graft.
SURGICAL TECHNIQUE AND HARDWARE MANAGEMENT
Incision and Exposure
Pre-existing surgical incisions should be utilized or judiciously extended whenever possible. The creation of narrow skin bridges (less than 7 cm wide) must be strictly avoided to prevent devastating skin necrosis and wound healing complications. Upon entering the joint, a thorough diagnostic arthroscopy is performed. Any concurrent meniscal tears or articular cartilage lesions must be addressed concurrently. The remnants of the failed primary ACL graft should be meticulously debrided to visualize the native femoral and tibial footprints.
Hardware Removal Strategies
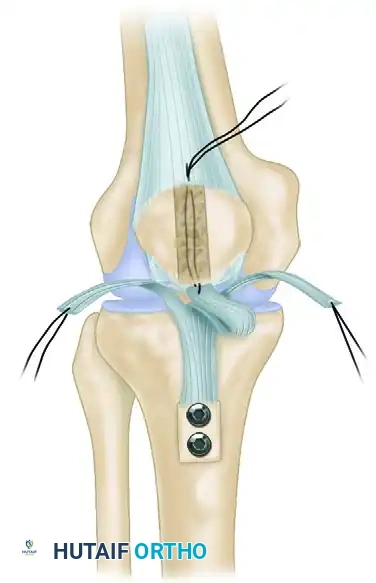
The management of retained hardware is a technically demanding aspect of revision surgery. The fundamental rule is that hardware should be removed only if absolutely necessary. Unnecessary removal of well-fixed, asymptomatic hardware that does not interfere with the new anatomic tunnels creates large cavitary bone defects that complicate subsequent fixation.
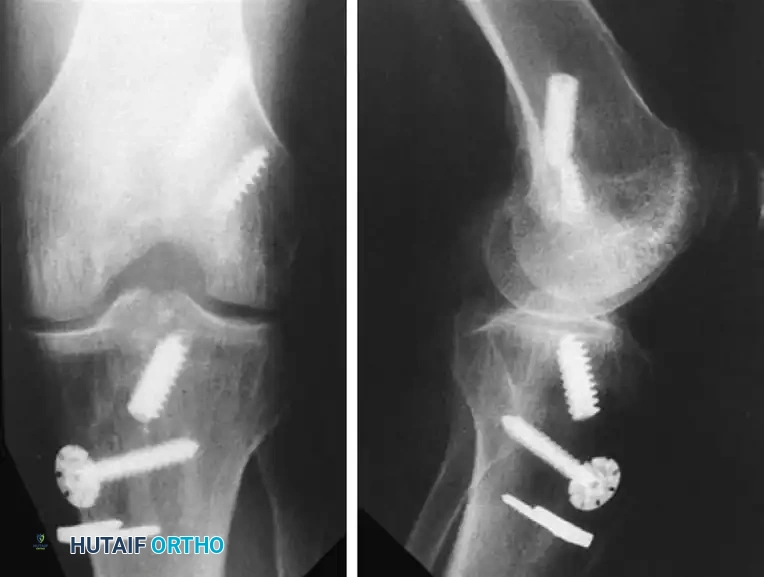
FIGURE 45-128: If possible, original fixation hardware should be left in place during revision anterior cruciate ligament reconstruction to avoid creating unnecessary osseous defects.
When hardware removal is mandatory (e.g., intersecting the new tunnel trajectory), the following principles apply:
* Femoral Hardware: Femoral interference screws are notoriously difficult to extract, particularly if they are deeply buried or covered by a layer of neo-osteogenesis. If a metallic screw has been in situ for an extended period, the metal may have softened. A single turn with an improperly seated screwdriver can strip the screw head, rendering extraction exceedingly difficult.
* Cannulated Systems: If the retained screw is cannulated, the surgeon should first pass a rigid guide pin through the central cannula. This ensures the screwdriver remains perfectly coaxial with the screw, drastically reducing the risk of stripping the head.
* Tibial Hardware: Tibial hardware is generally more accessible. Intraoperative fluoroscopy (image intensification) is highly recommended to locate screws that have been overgrown by bone.
* Bioabsorbable Screws: Surgeons must be aware that bioabsorbable screws (typically composed of poly-L-lactic acid [PLLA]) degrade very slowly. They can remain structurally intact for 2 to 5 years postoperatively. Attempting to extract a partially degraded bioabsorbable screw often results in fragmentation. It is generally preferable to leave these screws intact if they do not interfere, or to simply over-ream directly through the bioabsorbable material when creating the new tunnel.
GRAFT SELECTION IN REVISION SURGERY
Graft selection in the revision setting is complex and must be individualized based on the patient's anatomy, previous graft harvest sites, tunnel sizes, and patient expectations. The surgeon must always have a primary plan and at least one backup graft option available in the operating room.
Autograft Options
- Ipsilateral Bone-Patellar Tendon-Bone (BTB): Reharvesting the ipsilateral patellar tendon is generally not recommended. While some ultrasound and MRI studies suggest satisfactory ligament regeneration up to 18 months post-harvest, rigorous animal models (canine and goat) have consistently demonstrated significantly inferior biomechanical properties, reduced stiffness, and lower load-to-failure rates in reharvested tendons.
- Contralateral BTB: Utilizing a BTB autograft from the contralateral, uninjured knee is an excellent biomechanical option, providing a pristine graft with bone blocks for rigid fixation. However, it carries the significant disadvantage of introducing donor site morbidity (anterior knee pain, patellar fracture risk) to the patient's normal knee.
- Hamstring Autografts: Double, triple, or quadruple-looped semitendinosus and gracilis grafts are viable options. However, a critical limitation in revision surgery is graft-tunnel mismatch. Because revision tunnels are often widened, a standard hamstring graft may be too small in diameter. This mismatch compromises aperture fixation and leads to the "windshield wiper" effect—micromotion of the graft within the tunnel that exacerbates osteolysis and delays biological incorporation.
Allograft Options
Allografts are heavily utilized in revision ACL surgery. The most common choices include BTB allografts, Achilles tendon-bone allografts, and robust soft-tissue grafts like the Tibialis anterior or Fascia lata.
Advantages of Allografts:
* Zero donor site morbidity.
* Shorter operative and tourniquet times.
* Availability of large bone blocks to fill widened tunnels (e.g., using the calcaneal bone block of an Achilles allograft to fill a massive tibial defect).
* No size limitations, allowing the surgeon to precisely match the graft to the existing tunnel diameter.
Disadvantages and Biological Considerations:
* Cost: High financial burden.
* Disease Transmission: While exceedingly rare with modern tissue banking, a non-zero risk of viral or bacterial transmission exists.
* Sterilization Effects: The method of allograft sterilization profoundly impacts its structural integrity. High-dose gamma irradiation (greater than 1.5 to 2.0 Mrad) significantly degrades the collagen cross-linking, resulting in inferior mechanical properties and a higher clinical failure rate.
* Delayed Incorporation: Animal models (specifically goat studies) have conclusively demonstrated that allografts undergo a significantly delayed biological incorporation and remodeling process compared to autografts. The inflammatory immune response, while usually subclinical, slows the revascularization and cellular repopulation of the graft.
Surgical Warning: Because of the delayed biological incorporation of allografts, the postoperative rehabilitation protocol must be decelerated. Premature return to sport before complete allograft ligamentization is a primary driver of late revision failures.
POSTOPERATIVE REHABILITATION AND OUTCOMES
The rehabilitation protocol following revision ACL reconstruction must be highly individualized, taking into account the graft type, the security of fixation, and any concomitant procedures (e.g., meniscal repair, cartilage restoration, or extra-articular tenodesis).
In general, revision rehabilitation is significantly more conservative than primary ACL protocols. Weight-bearing may be restricted if large bone grafts were utilized or if fixation was tenuous due to poor bone stock. Return to cutting and pivoting sports is typically delayed until 9 to 12 months postoperatively, contingent upon the restoration of symmetric quadriceps strength, excellent neuromuscular control, and psychological readiness.
While modern surgical techniques have vastly improved the outcomes of revision ACL surgery, patients must be counseled preoperatively that clinical outcomes—including subjective knee scores, return to pre-injury level of sport, and long-term joint preservation—are statistically inferior to those of successful primary reconstructions. Meticulous execution of the principles outlined in this chapter is essential to maximize joint stability and optimize the patient's functional recovery.
📚 Medical References
- Revision ACL reconstruction: autograft versus allograft Arthroscopy 11:378, 1995 (abstract). Gillquist J, Liljedahl SO, Lindvall H: Reconstruction for old rupture of the anterior cruciate ligament: a follow-up study, Injury 2:271, 1971.
- Gillquist J, Messner K: Anterior cruciate ligament reconstruction and the long-term incidence of gonarthrosis, Sports Med 27:143, 1999.
- Gillquist J, Odensten M: Reconstruction of old anterior cruciate ligament tears with a Dacron prosthesis: a prospective study, Am J Sports Med 21:358, 1993.
- Glashow JL, Katz R, Schneider M, et al: Double-blind assessment of the value of magnetic resonance imaging in the diagnosis of anterior cruciate and meniscal lesions, J Bone Joint Surg 71A:113, 1989.
- Goldblatt JP, Fitzsmmons SE, Balk E, et al: Reconstruction of the anterior cruciate ligament: meta-analysis of patellar tendon versus hamstring tendon autograft, Arthroscopy 21:791, 2005.
- Gomes JLE, Marczyk LRS: Anterior cruciate ligament reconstruction with a loop or double thickness of semitendinosus tendon, Am J Sports Med 12:199, 1984.
- Good L, Odensten M, Gillquist J: Precision in reconstruction of the anterior cruciate ligament: a new positioning device compared with hand drilling, Acta Orthop Scand 58:658, 1987.
- Goradia VK, Rochat MC, Kida M, et al: Natural history of a hamstring tendon autograft used for anterior cruciate ligament reconstruction in a sheep model, Am J Sports Med 38:40, 2000.
- Graf B, Simon T, Jackson D: Isometric replacement of cruciate ligament substitutes. Unpublished material, presented in part at the annual meeting of the International Society of the Knee, Salzburg, Austria, May 1985.
- Graf BK, Henry J, Rothenberg M, et al: Anterior cruciate ligament reconstruction with patellar tendon: an ex vivo study of wear-related damage and failure at the femoral tunnel, Am J Sports Med 22:131, 1994.
- Graf BK, Ott JW, Lange RH, et al: Risk factors for restricted motion after anterior cruciate reconstruction, Orthopedics 17:909, 1994.
- Greis PE, Johnson DL, Fu FH: Revision anterior cruciate ligament surgery: causes of graft failure and technical considerations of revision surgery, Clin Sports Med 12:839, 1993.
- Greis PE, Steadman JR: Revision of failed prosthetic anterior cruciate ligament reconstruction, Clin Orthop Relat Res 325:78, 1996.
- Grontvedt T, Engebretsen L, Benum P, et al: A prospective, randomized study of three operations for acute rupture of the anterior cruciate ligament, J Bone Joint Surg 78A:159, 1996.
- Grood ES, Suntay WJ, Noyes FR, et al: Biomechanics of the knee-extension exercise: effect of cutting the anterior cruciate ligament, J Bone Joint Surg 66A:725, 1984.
- Guzzanti V, Falciglia F, Gigante A, et al: The effect of intraarticular ACL reconstruction on the growth plates of rabbits, J Bone Joint Surg 76B:960, 1994.
- Gwinn DE, Wilckens JH, McDevitt ER, et al: The relative incidence of anterior cruciate ligament injury in men and women at the United States Naval Academy, Am J Sports Med 28:98, 2000.
- Hame SL, Markolf KL, Gabayan AJ, et al: The effect of anterior cruciate ligament graft rotation on knee laxity and graft tension: an in vitro biomechanical analysis, Arthroscopy 18:55, 2002.
- Hanley P, Lew WD, Lewis JL, et al: Load sharing and graft forces in anterior cruciate ligament reconstructions with the ligament augmentation device, Am J Sports Med 17:414, 1989.
- Harner CD, Griffi n JR, Dunteman RC, et al: Evaluation and treatment of recurrent instability after anterior cruciate ligament reconstruction, J Bone Joint Surg 82A:1652, 2000.
- Harner CD, Paulos LE, Greenwald AE, et al: Detailed analysis of patients with bilateral anterior cruciate ligament injuries, Am J Sports Med 22:37, 1994.
- Harner CD, Poehling GG: Double bundle or double trouble? Arthroscopy 20:1013, 2004.
- Hart AJ, Buscombe J, Malone A, et al: Assessment of osteoarthritis after reconstruction of the anterior cruciate ligament: a study using single-photon emission computed tomography at ten years, J Bone Joint Surg 87B:1483, 2005.
- Harter RA, Osternig LR, Singer KM, et al: Long-term evaluation of knee stability and function following surgical reconstruction for anterior cruciate ligament insuffi ciency, Am J Sports Med 16:434, 1988.
- Harter RA, Osternig LR, Singer KM: Instrumented Lachman tests for the evaluation of anterior laxity after reconstruction of the anterior cruciate ligament, J Bone Joint Surg 71A:975, 1989.
- Hefzy MS, Grood ES, Noyes FR: Factors affecting the region of most isometric femoral attachments. II. The anterior cruciate ligament, Am J Sports Med 17:208, 1989.
- Hewett TE, Myer GD, Ford KR, et al: Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study, Am J Sports Med 33:492, 2005.
- Holmes PE, James SL, Larson RL, et al: Retrospective direct comparison of three intraarticular anterior cruciate ligament reconstructions, Am J Sports Med 19:596, 1991.
- Hooper GJ, Walton DI: Reconstruction of the anterior cruciate ligament using the bone-block iliotibial-tract transfer, J Bone Joint Surg 69A:1150, 1987.
- Howe JG, Johnson RJ, Kaplan MJ, et al: Anterior cruciate ligament reconstruction using quadriceps patellar tendon graft. I. Long-term follow-up, Am J Sports Med 19:447, 1991.
- Howell SM, Barad SJ: Knee extension and its relationship to the slope of the intercondylar roof: implications for positioning the tibial tunnel in anterior cruciate ligament reconstructions, Am J Sports Med 23:288, 1995.
- Howell SM, Clark JA: Tibial tunnel placement in anterior cruciate ligament reconstructions and graft impingement, Clin Orthop Relat Res 283:187, 1992.
- Howell SM, Deutsch ML: Comparison of endoscopic and two-incision techniques for reconstructing a torn anterior cruciate ligament using hamstring tendons, Arthroscopy 15:594, 1999.
- Howell SM, Knox KE, Farley TE, et al: Revascularization of a human anterior cruciate ligament graft during the fi rst two years of implantation, Am J Sports Med 23:42, 1995.
- Howell SM, Taylor MA: Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof, J Bone Joint Surg 75A:1044, 1993.
- Hughston JC: Anterior cruciate–defi cient knee, Am J Sports Med 11:1, 1983 (editorial). Hughston JC: Complications of anterior cruciate ligament surgery, Orthop Clin North Am 16:237, 1985.
- Hughston JC, Barrett GR: Acute anteromedial rotatory instability: long-term results of surgical repair, J Bone Joint Surg 65A:145, 1983.
- Indelicato PA, Linton RC, Huegel M: The results of fresh-frozen patellar tendon allografts for chronic anterior cruciate ligament defi ciency of the knee, Am J Sports Med 20:118, 1992.
- Indelicato PA, Pascale MS, Huegel MO: Early experience with the GORE-TEX polytetrafl uoroethylene anterior cruciate ligament prosthesis, Am J Sports Med 17:55, 1989.
- Insall JN, Joseph DM, Aglietti P, et al: Bone-block iliotibial-band transfer for anterior cruciate insuffi ciency, J Bone Joint Surg 63A:560, 1981.
- Ireland J, Trickey EL: MacIntosh tenodesis for anterolateral instability of the knee, J Bone Joint Surg 62B:340, 1980.
- Irrgang JJ, Harner CD: Loss of motion following knee ligament reconstruction, Sports Med 19:150, 1995.
- Jackson DW, Cohn BT, Morrison DS: A new technique for harvesting the patella tendon in patients undergoing anterior cruciate ligament reconstruction, Orthopedics 13:165, 1990.
- Jackson DW, Gasser SI: Tibial tunnel placement in ACL reconstruction, Arthroscopy 10:124, 1994.
- Jackson DW, Grood ES, Arnoczky SP, et al: Cruciate reconstruction using freeze dried anterior cruciate ligament allograft and a ligament augmentation device (LAD): an experimental study in a goat model, Am J Sports Med 15:528, 1987.
- Jackson DW, Grood ES, Arnoczky SP, et al: Freeze-dried anterior cruciate ligament allografts: preliminary studies in a goat model, Am J Sports Med 15:295, 1987.
- Jackson DW, Grood ES, Cohn BT, et al: The effects of in situ freezing on the anterior cruciate ligament, J Bone Joint Surg 73A:201, 1991.
- Jackson DW, Grood ES, Goldstein JD, et al: A comparison of patellar tendon autograft and allograft used for anterior cruci- ate ligament reconstruction in the goat model, Am J Sports Med 21:176, 1993.
- Jackson DW, Grood ES, Wilcox P, et al: The effects of processing techniques on the mechanical properties of bone–anterior cruciate ligament–bone allografts: an experimental study in goats, Am J Sports Med 16:101, 1988.
- Jackson DW, Schaefer RK: Cyclops syndrome: loss of extension following intra-articular anterior cruciate ligament reconstruction, Arthroscopy 6:171, 1990.
- Jackson DW, Simon TM, Kurzweil PR, et al: Survival of cells after intra-articular transplantation of fresh allografts of the patellar and anterior cruciate ligaments: DNA-probe analysis in a goat model, J Bone Joint Surg 74A:112, 1992.
- Jansson KA, Linko E, Sandelin J, et al: A prospective randomized study of patellar versus hamstring tendon autografts for anterior cruciate ligament reconstruction, Am J Sports 31:12, 2003.
- Jarvela T, Kannus P, Jarvinen M: Anterior knee pain 7 years after an anterior cruciate ligament reconstruction with a bone– patellar tendon–bone autograft, Scand J Med Sci Sports 10:221, 2000.
- Jarvela T, Paakkala T, Kannus P, et al: The incidence of patellofemoral osteoarthritis and associated fi ndings 7 years after anterior cruciate ligament reconstruction with a bone– patellar tendon–bone autograft, Am J Sports Med 29:18, 2001.
- Jarvela T, Paakkala T, Kannus P, et al: Ultrasonographic and power Doppler evaluation of the patellar tendon ten years after harvesting its central third for reconstruction of the anterior cruciate ligament: comparison of patients without or with anterior knee pain, Am J Sports Med 32:39, 2004.
- Jaureguito JW, Paulos LE: Why grafts fail, Clin Orthop Relat Res 325:25, 1996.
- Johnson DL, Fu FH: Anterior cruciate ligament reconstruction: why do failures occur, Instr Course Lect 44:391, 1994.
- Johnson DL, Harner CD, Maday MG, et al: Revision anterior cruciate ligament surgery. In Fu FH, Harner CD, Vince KG, eds: Knee surgery, vol 1, Baltimore, 1994, Williams & Wilkins. Johnson DL, Miller MD, Fu FH: The arthroscopic “impingement test” during anterior cruciate ligament reconstruction, Arthroscopy 9:714, 1993.
- Johnson GE, Shelbourne KD: Patient selection for anterior cruciate ligament reconstruction, Oper Tech Sports Med 1:16, 1993.
- Johnson RJ, Beynnon BD, Nichols CE, et al: Current concepts review: the treatment of injuries of the anterior cruciate ligament, J Bone Joint Surg 74A:140, 1992.
- Jones KG: Reconstruction of the anterior cruciate ligament using the central one-third of the patellar ligament, J Bone Joint Surg 52A:1302, 1970.
- Jones KG: Results of use of the central one-third of the patellar ligament to compensate for anterior cruciate ligament defi ciency, Clin Orthop Relat Res 147:39, 1980.
- Jonsson H, Elmqvist LG, Kärrholm J, et al: Over-the-top or tunnel reconstruction of the anterior cruciate ligament, J Bone Joint Surg 76B:82, 1994.
- Kannus P, Järvinen M: Conservatively treated tears of the anterior cruciate ligament: long-term results, J Bone Joint Surg 69:1007, 1987.
- Kannus P, Latvala K, Järvinen M: Thigh muscle strengths in the anterior cruciate ligament–defi cient knee: isokinetic and isometric long-term results, J Orthop Sports Phys Ther 9:223, 1987.
- Kaplan MJ, Howe JG, Fleming B, et al: Anterior cruciate ligament reconstruction using quadriceps patellar tendon graft. II. A specifi c sport review, Am J Sports Med 19:458, 1991.
- Karns DJ, Hedit RS Jr, Holladay BR, et al: Case report: revision anterior cruciate ligament reconstruction, Arthroscopy 10:48, 1994.
- Kartus J, Magnusson L, Stener S, et al: Complications following arthroscopic anterior cruciate ligament reconstruction. A 2to 5-year follow-up of 604 patients with special emphasis on anterior knee pain, Knee Surg Sports Traumatol Arthrosc 7:28, 1999.
- Kartus J, Stener S, Lindahl S, et al: Ipsior contralateral patellar tendon graft in anterior cruciate ligament revision surgery: a comparison of two methods, Am J Sports Med 26:499, 1998.
- Keays SL, Bullock-Saxton J, Keays AC: Strength and function before and after anterior cruciate ligament reconstruction, Clin Orthop Relat Res 373:174, 2000.
- Kennedy JC, Fowler PJ: Medial and anterior instability of the knee: an anatomical and clinical study using stress machines, J Bone Joint Surg 53A:1257, 1971.
- Kennedy JC, Stewart R, Walker DM: Anterolateral rotatory instability of the knee joint: an early analysis of the Ellison procedure, J Bone Joint Surg 60A:1031, 1978.
- Kennedy JC, Weinberg HW, Wilson AS: The anatomy and function of the anterior cruciate ligament, as determined by clinical and morphological studies, J Bone Joint Surg 56A:223, 1974.
- Kessler MA, Behrend H, Rukavina A, et al: Function and osteoarthritis after ACL rupture: 12-year follow-up results after non-operative vs. operative treatment, 25th meeting of the Arthroscopy Association of North America, Hollywood, Fla, May 18-21, 2006.
- Khalfayan EE, Sharkey PF, Alexander AH, et al: The relationship between tunnel placement and clinical results after anterior cruciate ligament reconstruction, Am J Sports Med 24:335, 1996.
- Kilger RH, Stehle J, Fisk JA, et al: Anatomical double-bundle anterior cruciate ligament reconstruction after valgus high tibial osteotomy: a biomechanical study, Am J Sports Med 34:961, 2006.
- Kleiner JB, Amiel D, Roux RD, et al: Origin of replacement cells for the anterior cruciate ligament allograft, J Orthop Res 4:466, 1986.
- Klootwyk TE, Shelbourne KD, DeCarlo MS: Perioperative rehabilitation considerations, Oper Tech Sports Med 1:22, 1993.
- Kornblatt I, Warren RF, Wickiewicz TL: Long-term follow-up of anterior cruciate ligament reconstruction using the quadriceps tendon substitution for chronic anterior cruciate ligament insuffi ciency, Am J Sports Med 16:444, 1988.
- Kurosaka M, Yoshiya S, Andrish JT: A biomechanical comparison of different surgical techniques of graft fi xation in anterior cruciate ligament reconstruction, Am J Sports Med 15:225, 1987.
- Lambert KL: Vascularized patellar tendon graft with rigid internal fi xation for anterior cruciate ligament insuffi ciency, Clin Orthop Relat Res 172:85, 1983.
- LaPrade RF, Burnett QM II: Femoral intercondylar notch stenosis and correlation to anterior cruciate ligament injuries: a prospective study, Am J Sports Med 22:198, 1994.
- LaPrade RF, Hamilton CD, Montgomery RD, et al: The reharvested central third of the patellar tendon: a histologic and biomechanical analysis, Am J Sports Med 25:779, 1997.
- Larson RL: Augmentation of acute rupture of the anterior cruciate ligament, Orthop Clin North Am 16:135, 1985.
- Larson RL, Taillon M: Anterior cruciate ligament insuffi ciency: principles of treatment, J Am Acad Orthop Surg 2:26, 1994.
- Larson RV: ACL reconstruction utilizing autograft hamstring tendons. Paper presented at the American Academy of Orthopaedic Surgeons Summer Institute, Seattle, Sept 1999.
- Lipscomb AB, Johnston RK, Snyder RB, et al: Secondary reconstruction of anterior cruciate ligament in athletes by using the semitendinosus tendon: preliminary report of 78 cases, Am J Sports Med 7:81, 1979.
- Lipscomb AB, Johnston RK, Snyder RB, et al: Evaluation of hamstring strength following use of semitendinosus and gracilis tendons to reconstruct the anterior cruciate ligament, Am J Sports Med 10:340, 1982.
- Liu SH, Osti L, Hentry M, et al: The diagnosis of acute complete tears of the anterior cruciate ligament: comparison of MRI, arthrometry, and clinical examination, J Bone Joint Surg 77B:586, 1995.
- Lochemes JJ, Dutkowsky JP, Pifer LL, et al: Pre-surgical inactivation of HIV-1 by in vitro cesium 137 irradiation. Transactions of the 41st annual meeting of the Orthopaedic Research Society, Orlando, Fla, Feb 1995.
- Loh JC, Fukuda Y, Tsuda E, et al: Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o’clock and 10 o’clock femoral tunnel placement, Arthroscopy 19:297, 2003.
- Lohmander LS, Hoerner LA, Lark MW: Metalloproteinases, tissue inhibitor, and proteoglycan fragments in knee synovial fl uid in human osteoarthritis, Arthritis Rheum 36:181, 1993.
- Lohmander LS, Ostenberg A, Englund M, et al: High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury, Arthritis Rheum 50:3145, 2004.
- López-Vázquez E, Juan JA, Vila E, et al: Reconstruction of the anterior cruciate ligament with a Dacron prosthesis, J Bone Joint Surg 73A:1294, 1991.
- Losee RE: Diagnosis of chronic injury to the anterior cruciate ligament, Orthop Clin North Am 16:83, 1985.
- Lukianov AV, Gillquist J, Grana WA, et al: An anterior cruciate ligament (ACL) evaluation format for assessment of artifi cial or autologous anterior cruciate reconstruction results, Clin Orthop Relat Res 218:167, 1987.
- Lukianov AV, Richmond JC, Barrett GR, et al: A multicenter study on the results of anterior cruciate ligament reconstruction using a Dacron ligament prosthesis in “salvage” cases, Am J Sports Med 17:380, 1989.
- MacDonald PB, Hedden D, Pacin O, et al: Effects of an accelerated rehabilitation program after anterior cruciate ligament reconstruction with combined semitendinosus-gracilis autograft and a ligament augmentation graft, Am J Sports Med 23:588, 1995.
- MacIntosh DL, Darby TA: Lateral substitution reconstruction, J Bone Joint Surg 58B:142, 1976.
- MacNicol MF, Penny ID, Sheppard L: Early results of the LeedsKeio anterior cruciate ligament replacement, J Bone Joint Surg 73B:377, 1991.
- Maeda A, Shino K, Horibe S, et al: Anterior cruciate ligament reconstruction with multistranded autogenous semitendinosus tendon, Am J Sports Med 24:504, 1996.
- Markolf KL, Hame S, Hunter DM, et al: Effects of femoral tunnel placement on knee laxity and forces in an anterior cruciate ligament graft, J Orthop Res 20:1016, 2002.
- Markolf KL, Kochan A, Amstutz HC: Measurement of knee stiffness and laxity in patients with documented absence of the anterior cruciate ligament, J Bone Joint Surg 66A:242, 1984.
- Marshall JL, Girgis FG, Zelko RR: The biceps femoris tendon and its functional signifi cance, J Bone Joint Surg 54A:1444, 1972.
- Marshall JL, Warren RF, Wickiewicz TL, et al: The anterior cruciate ligament: a technique of repair and reconstruction, Clin Orthop Relat Res 143:97, 1979.
- Matthews LS, Soffer SR: Pitfalls in the use of interference screw for anterior cruciate ligament reconstruction: brief report, Arthroscopy 5:225, 1989.
- Mayday MG, Harner CD, Fu FH: Revision ACL surgery: evaluation and treatment. In Feagin JA Jr, ed: The crucial ligaments: diagnosis and treatment of ligamentous injuries about the knee, ed 2, New York, 1994, Churchill Livingstone. McAllister DR, Parker RD, Cooper AE, et al: Outcomes of postoperative
You Might Also Like