ABOS Part I & AAOS OITE Orthopedic Surgery Review: MOM Hip Resurfacing, Paget's Disease, Trauma | Part 21587

Key Takeaway
This comprehensive module provides 30 advanced multiple-choice questions mirroring the ABOS Part I and AAOS OITE examinations. It covers high-yield clinical cases in orthopedic surgery, including Metal-on-Metal hip resurfacing complications, Paget's disease, pelvic trauma, periprosthetic fractures, and other key musculoskeletal pathologies, offering detailed explanations for exam preparation.
ABOS Part I & AAOS OITE Orthopedic Surgery Review: MOM Hip Resurfacing, Paget's Disease, Trauma | Part 21587
A 52-year-old woman presents with non-specific right hip pain 3 years after a right metal-on-metal (MOM) hip resurfacing. Her anteroposterior (AP) radiograph is shown below. Based on the provided image and case discussion, which of the following findings is most concerning for potential complications related to her MOM resurfacing?

Correct Answer: C
The candidate in the case specifically notes that the anteroposterior (AP) radiograph demonstrates a higher abduction angle (lateral opening) than normal, with current recommendations for an acetabular abduction angle of 40 degrees. The discussion emphasizes that a high cup angle has been consistently reported to lead to greater wear and higher serum metal ion levels, which are direct precursors to complications like ALVAL and pseudotumours. This finding is a significant risk factor for the patient's presenting symptoms.
Option A is incorrect because a divot sign is associated with impingement and repetitive bone-to-component abutment, which can cause wear. Its absence does not rule out other causes of wear or complications, and the case highlights other significant risk factors.
Option B is incorrect. The case states that a small head size (less than 46mm) is a risk factor for ALVAL and pseudotumours, not protective. The candidate notes, 'the head size appears small; the current recommendations are that unless a minimum 46 mm head size can be used the procedure should not be performed because of the risks of ALVAL and pseudotumours.'
Option D is incorrect. While no obvious narrowing of the neck is a positive finding, it does not mitigate the risk associated with a high abduction angle or small head size, which are explicitly linked to complications in the case.
Option E is incorrect. The absence of radiolucency around the metaphyseal stem is a good sign regarding aseptic loosening, but it does not address the primary concern of metal-on-metal wear and pseudotumour formation, which are the focus of this case and are linked to cup positioning and head size.
A 52-year-old woman with a 3-year history of right metal-on-metal hip resurfacing presents with non-specific right hip pain. The examiner asks about the difference between ALVAL and pseudotumour. Based on the case discussion, which statement accurately differentiates ALVAL from a pseudotumour?
Correct Answer: C
The case explicitly states: 'ALVAL (aseptic lymphocyte-dominated vasculitis-associated lesion) is caused by metal particulate debris. Patients present with localized hip pain and a localized osteolytic reaction. A more severe inflammatory reaction is termed a pseudotumour.' This directly supports option C.
Option A is incorrect because it reverses the severity and characteristics. ALVAL is the localized osteolytic reaction, and pseudotumour is the more severe inflammatory reaction.
Option B is incorrect. The case states that the origin of pseudotumours is 'probably multifactorial caused either by excessive wear, metal hypersensitivity, a combination of the two, or as yet an unknown cause.' ALVAL is caused by metal particulate debris, which can be related to wear, not exclusively hypersensitivity.
Option D is incorrect. The case mentions that 'Pseudotumor-like reactions have also been reported in non-metal-on-metal bearings,' indicating they are not exclusive to MOM. ALVAL is specifically linked to metal particulate debris, which is a hallmark of MOM wear.
Option E is incorrect. While Campbell et al. reported some pseudotumours with minimal wear suggesting hypersensitivity, the case also states that 'Several studies have described an association between pseudotumours and increased wear of retrieved components.' Therefore, pseudotumours are not *always* associated with minimal wear, and their origin is multifactorial.
Following the diagnosis of a pseudotumour in a 52-year-old woman with a painful MOM hip resurfacing, the examiner asks about risk factors. Which of the following combinations of patient characteristics and implant features would represent the highest risk for developing a pseudotumour, according to the case?
Correct Answer: B
The case explicitly lists significant risk factors for the development of pseudotumour: 'female sex, age less than 40 years, small component size, hip dysplasia and specific implant designs (ASR).'
Option B includes female sex, age 38 (less than 40), small component size, and history of hip dysplasia. This combination aligns perfectly with multiple high-risk factors mentioned in the case.
Option A includes male sex and age 45 (not less than 40), which are not high-risk factors according to the case.
Option C includes age 55 (not less than 40) and large component size, which are not high-risk factors.
Option D includes male sex, which is not a risk factor, and while age 30 and small component size are risk factors, the combination in B is stronger due to the inclusion of female sex and hip dysplasia.
Option E includes female sex, but age 42 is not less than 40, and 'average component size' is not specified as a risk factor (small component size is). Inflammatory arthritis is listed as a factor for higher revision rates for hip resurfacing in general, but not specifically for pseudotumour development in the risk factor list.
A 52-year-old woman with a painful MOM hip resurfacing is being investigated for her symptoms. The examiner asks about the British Hip Society's recommendations for investigation. Beyond a careful history and physical examination, which of the following is the most appropriate initial diagnostic step according to the British Hip Society guidelines mentioned in the case?
Correct Answer: C
The case states, when prompted about British Hip Society recommendations: 'Blood cobalt and chromium ions should be measured, as these are indicators of surface wear. If levels are raised the patient will require close observation. If levels are rising and the hip is painful it may be sensible to consider revising the implant.'
Option A is incorrect because investigation precedes surgery. While revision may be necessary, it's not the immediate diagnostic step.
Option B is a general diagnostic tool but not specifically highlighted as the initial British Hip Society recommendation for a painful MOM resurfacing in the context of metal ion concerns.
Option D is incorrect. While nerve impingement could be an extrinsic cause of pain, the primary concern with a painful MOM resurfacing is intrinsic pathology related to the implant, for which metal ion levels are a key indicator.
Option E is a diagnostic tool but not the specific initial recommendation from the British Hip Society for evaluating MOM resurfacing complications related to wear and metal ions.
A 52-year-old woman with a painful MOM hip resurfacing undergoes further imaging after elevated metal ion levels. The MRI scan with metal artifact reduction sequences (MARS) is shown below. Based on the images and the case, what is the most appropriate immediate next step in management?
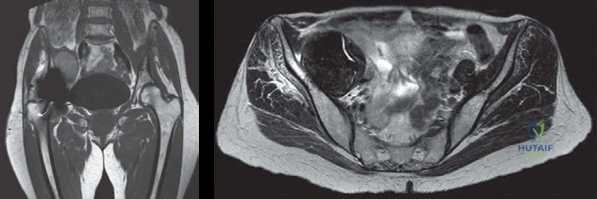
Correct Answer: C
The MRI (Figures 2.5a and 2.5b) demonstrates an intra-pelvic mass, which the examiner confirms was a pseudotumour, palpable clinically. When asked 'What are you going to do?', the candidate responds: 'This patient requires urgent revision surgery to the hip.' The candidate further stresses 'the importance of early revision surgery as the longer the MOM resurfacing implant is left in place the more extensive the soft tissue destruction will most likely be.'
Option A and B are incorrect as conservative management is not appropriate for a symptomatic pseudotumour, especially one that is palpable and confirmed by MRI.
Option D is incorrect. While a biopsy could confirm the diagnosis histologically, the clinical presentation, elevated metal ions, and characteristic MRI findings are sufficient for diagnosis and the case indicates immediate surgical intervention is required, not further diagnostic delay.
Option E is incorrect. The patient has a confirmed, symptomatic pseudotumour. Continuing observation would delay necessary treatment and potentially lead to more extensive soft tissue destruction, as highlighted by the candidate.
During the discussion of revision surgery for the pseudotumour, the examiner asks about the principles of surgery. Which of the following surgical principles is most consistent with the candidate's recommended approach for this patient?
Correct Answer: C
The candidate outlines the principles of surgery: 'The pseudotumour needs to be managed with aggressive debridement of all involved soft tissue. It is important to do a thorough debridement of the abnormal tissue similar to the treatment of infection.' Regarding bearing surfaces, the candidate states: 'Although she is still relatively young I would use a metal-on-polyethylene bearing surface. A ceramic bearing surface has the potential for catastrophic fracture. We are already revising for a rare complication and we don’t want anything to go wrong again. However I would use an uncemented implant. I would keep the option of using a constrained cup open as the soft tissues may be so poorly compromised that the hip is unstable but obviously would prefer to avoid this, as components will loosen early in this situation.'
Option C accurately reflects all these points: thorough debridement, uncemented metal-on-polyethylene bearing, and consideration of a constrained cup for instability.
Option A is incorrect because the candidate specifically advises against a ceramic bearing surface due to fracture risk.
Option B is incorrect due to 'limited debridement' (the candidate recommends aggressive/thorough) and 'cemented' (the candidate recommends uncemented).
Option D is incorrect. 'Debridement only of the visible mass' is not thorough enough, and 'large metal-on-metal jumbo hip replacement' is contraindicated as a primary procedure due to metal wear and corrosion, and certainly not appropriate for revision of a MOM pseudotumour.
Option E is incorrect. The case emphasizes urgent revision surgery due to the risk of extensive soft tissue destruction, not conservative management.
The examiner challenges the candidate on the utility of MOM hip resurfacing, suggesting that conventional THA works equally well. The candidate defends resurfacing by listing its advantages. Which of the following is NOT listed as an advantage of MOM hip resurfacing in the case discussion?
Correct Answer: D
The candidate lists several advantages of MOM hip resurfacings: 'better restoration of hip biomechanics, improved proprioceptive feedback, improved wear characteristics with no PE-induced osteolysis, increased levels of postsurgical activity, greater range of movement, reduced risk of dislocation, improved femoral bone stock mass because the neck and most of the head are retained and ease of conversion to a THA if the implant should fail.'
However, when discussing outcomes, the case explicitly states: 'There is a higher revision rate in hip resurfacing compared with conventional THA.' Therefore, lower revision rates are NOT an advantage; in fact, the opposite is true.
Options A, B, C, and E are all directly listed as advantages by the candidate in the case.
The examiner asks about contraindications for hip resurfacing. Based on the detailed list provided by the candidate, which of the following patient profiles would be an absolute contraindication for hip resurfacing?
Correct Answer: D
The candidate lists several contraindications for resurfacing: 'These include severe osteoporosis, insufficient bone stock in the femoral head, large cysts at the femoral neck or head, a narrow femoral neck, notching of the femoral neck and severe obesity (BMI > 35 kg/m2). Other contraindications include a history of chronic renal disease, metal hypersensitivity, those with anatomical abnormalities in the acetabulum or proximal femur and certainly caution in women of childbearing age.'
Option D, 'A 60-year-old male with severe osteoporosis and insufficient bone stock in the femoral head,' combines two absolute contraindications explicitly stated: 'severe osteoporosis' and 'insufficient bone stock in the femoral head.'
Option A: BMI of 32 is not > 35 (severe obesity). Mild femoral head cysts are not listed as an absolute contraindication, though large cysts are.
Option B: While metal hypersensitivity is a contraindication, the question asks for an *absolute* contraindication from the list. This is a strong contraindication, but D combines two distinct, severe bone-related contraindications.
Option C: A narrow femoral neck is a contraindication, but this option only lists one. Option D lists two severe, bone-related contraindications.
Option E: 'Caution in women of childbearing age' is mentioned, but the candidate clarifies that most surgeons believe women should not be excluded, although the examiner notes a trend to avoid in all females. It's not presented as an *absolute* contraindication in the same vein as severe osteoporosis or insufficient bone stock.
After successful revision surgery for the pseudotumour, the patient's postoperative radiograph is shown below. The examiner notes that the patient was kept non-weightbearing for 6 weeks due to an extensive anterior wall defect in the acetabulum. This specific post-operative instruction primarily aims to prevent which of the following complications?

Correct Answer: C
The case states: 'We kept her non-weightbearing for 6 weeks as there was quite an extensive anterior wall defect in the acetabulum.' An acetabular wall defect compromises the structural integrity and initial stability of the acetabular component. Non-weightbearing protects the bone-implant interface during early healing and osseointegration, thereby preventing excessive stress that could lead to micromotion, loosening, or migration of the acetabular component.
Option A (DVT) is a general surgical complication, but non-weightbearing is not its primary prevention strategy; anticoagulation and early mobilization (when permitted) are.
Option B (Heterotopic ossification) is a known complication of hip surgery, but non-weightbearing does not directly prevent it. Prophylaxis typically involves NSAIDs or radiation.
Option D (Periprosthetic joint infection) is a serious complication, but non-weightbearing is not a direct preventative measure. Strict aseptic technique and prophylactic antibiotics are key.
Option E (Femoral nerve palsy) is a potential nerve injury during surgery, but non-weightbearing is not a preventative measure for this complication.
The examiner asks about the outcomes of hip resurfacing compared with conventional THA. Based on the case discussion, which statement accurately summarizes the comparative outcomes?
Correct Answer: B
The case directly addresses this: 'Several recent studies report identical Harris hip scores but a greater percentage of patients with resurfacing involved in high demand activities. There is a higher revision rate in hip resurfacing compared with conventional THA.'
Option A is incorrect because hip resurfacing does not have lower revision rates; it has higher revision rates.
Option C is incorrect. The candidate lists 'better restoration of hip biomechanics' and 'improved proprioceptive feedback' as advantages of MOM hip resurfacing, not conventional THA.
Option D is incorrect. While hip resurfacing does have a reduced risk of dislocation, it is associated with 'no PE-induced osteolysis' because it's a metal-on-metal bearing, not a higher incidence of it.
Option E is incorrect. The candidate lists 'improved femoral bone stock mass because the neck and most of the head are retained' and 'ease of conversion to a THA if the implant should fail' as advantages of MOM hip resurfacing, not conventional THA.
A 68-year-old woman presents with an 18-month history of left hip pain and difficulty walking. An anteroposterior radiograph of the pelvis is obtained:
Based on the radiographic findings, which of the following is the MOST characteristic feature of Paget's disease in this image?

Correct Answer: C
The radiograph demonstrates classic features of Paget's disease, including a coarsened trabecular pattern, thickened left cortex, and increased density (sclerosis) of the left hip compared with the right side. Both iliopectineal (Brim sign) and ilioischiatic lines are thickened, and there is sclerosis involving the left pelvis (ileum, ischium, and pubic rami), left femur, and lower lumbar spine. These findings are highly suspicious of Paget's disease, which is characterized by disorganized bone turnover leading to biomechanically weak, enlarged, and sclerotic bone.
Option A describes features of osteoarthritis, which may coexist but are not the primary findings of Paget's disease itself. Option B describes osteoporosis, which is characterized by decreased bone density, the opposite of what is seen in the sclerotic phase of Paget's. Option D describes lytic lesions, which can be seen in the early lytic phase of Paget's (e.g., osteoporosis circumscripta in the skull or 'candle flame' sign in long bones), but the predominant features in this image are sclerotic. Multiple lytic lesions are also characteristic of other conditions like multiple myeloma or metastatic disease, which are differential diagnoses but do not match the overall pattern. Option E describes features of ankylosing spondylitis, which is unrelated to the findings in this case.
A 72-year-old male with known Paget's disease of the lumbar spine presents with progressive bilateral lower extremity weakness and numbness. Physical examination reveals diminished sensation in a stocking-glove distribution and hyperreflexia. Which of the following is the MOST likely cause of his neurological symptoms?
Correct Answer: C
The case describes Pagetic spinal stenosis as a complication, defined as compression of the spinal cord, cauda equina, or spinal nerves by expanded pagetic bony tissue of the spine. It is most common in the lumbar region and typically single level, causing cord or nerve root compression. The patient's symptoms of progressive bilateral lower extremity weakness, numbness, and hyperreflexia are classic signs of spinal cord or cauda equina compression.
Option A, compression fractures of the vertebral body, are common complications of spinal Paget's, but while they can cause neurological deficits, the primary mechanism of chronic, progressive compression in Paget's is often the expanded pagetic bone itself, rather than an acute fracture. Option B, high cardiac output, is a rare complication of Paget's due to increased bone vascularity, but it does not directly cause peripheral neuropathy. Option D, malignant transformation to osteosarcoma, is a serious complication, but it typically presents with unrelenting bone pain and radiographic bone destruction, not primarily with progressive bilateral neurological deficits in this manner. Option E, hydrocephalus, is a complication of skull involvement in Paget's disease, leading to increased intracranial pressure and cranial nerve deficits, but it would not cause lower extremity weakness and numbness in a stocking-glove distribution.
A 60-year-old patient with Paget's disease of the tibia presents with new onset anterior bowing and localized pain. Radiographs show a transverse fissure on the convex anterior surface of the tibia. This finding is best characterized as:
Correct Answer: C
The case states that in Paget's disease, 'Fine cracks may appear (stress fractures) which resemble Looser zones but occur on the convex bone surface.' The tibia developing an anterior curvature is also mentioned as a deformity that may result in fracture. The description of a transverse fissure on the convex anterior surface of the tibia in a patient with anterior bowing is highly consistent with a stress fracture in pagetic bone, which is biomechanically weak and prone to deformity and fracture.
Option A is incorrect because while they resemble Looser zones, the case explicitly differentiates them, stating they occur on the convex bone surface in Paget's, unlike Looser zones which are typically associated with osteomalacia and occur on the concave (compression) side. Option B, the 'candle flame' or 'blade of grass' sign, represents a wedge- or V-shaped pattern of advancing lysis in the diaphysis of long bones, characteristic of the lytic phase, not a stress fracture. Option D, while malignant transformation is a complication, a stress fracture is a more common and direct consequence of the altered bone mechanics in Paget's, and the description does not suggest the aggressive destruction seen with sarcoma. Option E, a 'picture-frame' vertebral body, is a radiographic feature of spinal Paget's, not a tibial finding.
A 55-year-old male with Paget's disease is being evaluated for hip pain. His alkaline phosphatase (AlkPhos) level is significantly elevated. The orthopedic surgeon is concerned about the potential for increased intraoperative bleeding during a planned total hip arthroplasty (THA). What is the MOST appropriate preoperative measure to mitigate this risk?
Correct Answer: C
The case explicitly states that 'Patients with very high AlkPhos levels are thought to be at higher risk of bleeding and heterotrophic ossification formation.' It also mentions that if Paget's disease is active, a referral for Pamidronate (a bisphosphonate) injection is indicated. Pamidronate is described as a 'potent inhibitor of osteoclastic activity, and hence bone resorption. This reduces bone vascularity and bleeding and possibly the incidence of heterotopic ossification.' Therefore, referring for Pamidronate is the most appropriate measure to reduce the risk of excessive bleeding due to increased bone vascularity in active Paget's disease.
Option A, prophylactic antibiotics, are standard for THA but do not address the specific bleeding risk associated with active Paget's. Option B, NSAIDs, are not indicated for reducing surgical bleeding; in fact, some can increase bleeding risk. Option D, a diagnostic local anesthetic injection, is important for differentiating joint pain from bone pain or referred pain, but it does not directly mitigate the risk of intraoperative bleeding from hypervascular pagetic bone. Option E is incorrect, as the case clearly highlights the tendency for excessive bleeding as a significant technical issue in THA for Paget's disease, necessitating specific blood management strategies.
During a total hip arthroplasty (THA) for a patient with severe Paget's disease of the proximal femur, the surgeon encounters extremely hard and sclerotic bone, making reaming and broaching difficult. Which of the following technical considerations is MOST appropriate in this scenario?
Correct Answer: B
The case explicitly addresses technical issues of performing THA in Paget's disease, stating: 'Bone can be very hard and sclerotic making it difficult to ream and broach. Burrs may be needed to enter the bone prior to reaming and/or broaching.' Therefore, using burrs to facilitate initial entry is the most appropriate technical consideration.
Option A is incorrect because the case highlights that hard, sclerotic bone *does* make reaming and broaching difficult, contradicting the idea of proceeding with standard techniques without modification. Option C is an extreme measure and generally not necessary, as the case discusses various strategies to overcome surgical challenges. Option D is incorrect; while uncemented components are used, they still require precise bone preparation for ingrowth, and the difficulty in reaming/broaching applies to both cemented and uncemented preparations. Option E, significantly increasing reamer size without proper preparation, could lead to iatrogenic fracture or malalignment in sclerotic bone.
A 65-year-old woman with Paget's disease of the pelvis and proximal femur is undergoing preoperative planning for a total hip arthroplasty. Her radiographs show significant varus deformity of the proximal femur and a protrusio deformity of the acetabulum. Which of the following is a key consideration for the femoral component during this surgery?
Correct Answer: C
The case states: 'Varus deformity of the proximal end of the femur predisposes to varus placement of the femoral component.' It further elaborates on managing severe deformity: 'In the majority of patients with Paget’s THA can be performed without need for osteotomy. However, if deformity is severe, precluding implantation with a standard stem, then planning for reduction osteotomy to correct the deformity and/or the use of modular stems must be made preoperatively.' Therefore, for severe deformity, osteotomy or modular stems are key considerations.
Option A is incorrect; the case states varus deformity predisposes to *varus* placement, not valgus. Option B is incorrect, as the case explicitly mentions that severe deformity may preclude implantation with a standard stem, necessitating other approaches. Option D is incorrect; the choice between cemented and uncemented is discussed, but varus deformity itself does not contraindicate cementless components, though severe deformity might influence the need for osteotomy regardless of fixation type. Option E is incorrect; protrusio deformity complicates surgery, and marked protrusio can make hip dislocation very difficult, not simplify femoral component insertion.
A 70-year-old patient with Paget's disease undergoes a total hip arthroplasty. Postoperatively, the patient develops significant heterotopic ossification (HO) around the hip joint. Based on the case discussion, what is the MOST accurate statement regarding HO in Paget's disease patients undergoing THA?
Correct Answer: B
The case explicitly states under 'Technical issues of performing THA in Paget’s disease': 'There is some controversy as to whether there is an increased risk of heterotopic ossification occurring from the abnormalities of osteogenic differentiation in Paget’s disease patients. Some surgeons routinely give prophylaxis to reduce the risk of HO.' Later, under 'Any special complications that can occur postoperatively?', the candidate correctly identifies 'a reported greater incidence of heterotopic ossification.'
Option A is incorrect, as the case clearly indicates a reported greater incidence of HO. Option C is incorrect; the case does not link HO exclusively to cemented THA. Option D is incorrect; the case does not mention age as a direct risk factor for HO in Paget's, although age is discussed in the context of cemented vs. uncemented implant choice. Option E is incorrect; while surgical excision might be a treatment for severe HO, the initial management strategy discussed is prophylaxis, and immediate excision is not the primary or sole management.
A 62-year-old patient with Paget's disease is being considered for total hip arthroplasty. The orthopedic surgeon is debating between a cemented and uncemented femoral component. The patient is otherwise healthy, and the bone is noted to be very sclerotic. Which of the following statements BEST reflects the current understanding and recommendations regarding implant choice in Paget's disease?
Correct Answer: C
The case discusses the evolving trend in implant choice: 'Although previous studies have recommended the use of cement in the last 20 years there has been a trend to use uncemented components.' It specifically states: 'Some surgeons prefer cementless components especially when bone is very sclerotic or a concurrent osteotomy is done. Extremely sclerotic bleeding bone will make interdigitation of cement difficult and cement extravasation into the fracture gaps may occur after osteotomy. If using a cementless cup the use of adjuvant acetabular screws is recommended.'
Option A is incorrect; while historically recommended, there's a trend towards uncemented, and the choice is now more nuanced. Option B is incorrect; the case explicitly states: 'Patients with Paget’s disease are not known to have compromised ability for fracture healing and these patients progress through the biological process of fracture healing at normal speed.' This supports ingrowth. Option D is incorrect; the case states: 'The worry that the altered morphology of pagetoid bone adversely influences ingrowth into cementless implants has not been borne out in practice.' Option E is incorrect; the examiner explicitly states, 'No, I am not aware of an increased risk of dislocation' in Paget's disease post-THA.
A 58-year-old patient with Paget's disease of the skull presents with progressive hearing loss and facial weakness. Which of the following is the MOST likely underlying mechanism for these symptoms?
Correct Answer: C
The case lists complications of Paget's disease, specifically mentioning skull involvement: 'An enlarged and deformed skull can lead to increased intracranial pressure, hydrocephalus or cranial nerve deficits such as facial palsy (narrowing of neural foramina), hearing loss or blindness (pressure on optic nerve).' Therefore, narrowing of neural foramina due to the enlarged and deformed pagetic bone is the most direct and likely mechanism for facial palsy and hearing loss.
Option A, high cardiac output, is a rare systemic complication and would not directly cause localized cranial nerve deficits. Option B, osteoporosis circumscripta, is a lytic phase radiographic feature of the skull, but it describes bone lysis, not the enlargement and deformation that leads to nerve compression. Option D, malignant transformation, is a possibility but less common than direct nerve compression from bone enlargement, and the symptoms described are classic for nerve impingement. Option E, 'cotton wool appearance' is a radiographic feature of mixed lytic/blastic skull involvement, and while it indicates thickened calvarium, the direct cause of cranial nerve deficits is the *pressure* or *narrowing* of foramina, not the appearance itself, and increased intracranial pressure is a separate complication that can also arise from skull enlargement, but the specific symptoms point to nerve compression.
A 68-year-old woman with Paget's disease of the left hemipelvis and proximal femur is being evaluated for persistent hip pain after a total hip arthroplasty (THA). Her alkaline phosphatase levels remain elevated. Which of the following postoperative complications is NOT specifically mentioned as an increased risk in Paget's disease patients following THA in the provided text?
Correct Answer: E
The examiner specifically states: 'No, I am not aware of an increased risk of dislocation.' This directly contradicts the idea of an increased risk of dislocation. The candidate initially suggests dislocation, but the examiner corrects this.
The other options are all mentioned as potential complications:
- Heterotopic ossification: 'There is a reported greater incidence of heterotopic ossification.'
- Osteolysis: 'However, several studies have documented osteolysis following THA in patients with Paget’s disease.'
- Periprosthetic fracture: 'Other complications include periprosthetic fracture around total hip implants...'
- Continuation of bone pain: '...and the continuation of bone pain following arthroplasty...'
A 45-year-old male presents following a high-speed motor vehicle collision. He is hemodynamically unstable, with a heart rate of 120 bpm and blood pressure of 80/50 mmHg. Physical examination reveals a widely abducted lower extremity, perineal ecchymosis, and scrotal swelling. A Foley catheter insertion is attempted but meets resistance. A CT scan confirms an open-book pelvic fracture (APC-III) with significant symphyseal diastasis and sacral fractures. Which of the following is the most appropriate *immediate* next step in management after initial ATLS protocol?
Correct Answer: D
The most immediate and life-saving intervention for a hemodynamically unstable patient with an open-book pelvic fracture (APC-III) after initial ATLS assessment is the application of a circumferential pelvic binder. This maneuver reduces pelvic volume, compresses vascular structures, and helps tamponade hemorrhage, thereby improving hemodynamic stability. While other interventions like angiography/embolization, C-clamp, or external fixation may be required, they are typically performed *after* initial stabilization with a binder. Laparotomy would be considered for identified intra-abdominal hemorrhage, but the initial focus is on the pelvic instability as the primary source of bleeding in this scenario. The urethral injury (resistance to Foley) needs to be addressed with a suprapubic catheter, but it is secondary to hemodynamic instability in this critical phase.
A 7-year-old child presents after a fall from a trampoline, complaining of neck pain and bilateral lower extremity weakness. Neurological examination reveals 2/5 strength in both lower extremities, normal upper extremity strength, and intact sensation throughout. Reflexes are hyperreflexic in the lower extremities. X-rays of the cervical spine are normal, and a subsequent MRI shows no fracture, dislocation, or spinal cord compression, but reveals subtle signal changes within the cord. What is the most likely diagnosis?
Correct Answer: C
The clinical presentation of a child with neurological deficits after trauma, coupled with normal radiographs and absence of bony pathology on MRI, but with signal changes within the cord, is pathognomonic for Spinal Cord Injury Without Radiographic Abnormality (SCIWORA). This condition is more common in children due to increased spinal elasticity and laxity of ligaments, allowing for transient cord stretch or compression without bony injury. Atlantoaxial instability would typically show radiographic evidence. Transient myelopathy and acute transverse myelitis are diagnoses of exclusion often related to inflammatory or idiopathic causes, less likely acutely post-trauma with cord signal changes. An epidural hematoma would be visible on MRI as a mass compressing the cord.
A 68-year-old female presents with groin pain and a leg length discrepancy 6 months following a cemented total hip arthroplasty for osteoarthritis. She reports increasing pain with ambulation and night pain. Radiographs demonstrate lucencies greater than 2mm around the femoral stem and acetabular component in multiple zones, with some subsidence of the femoral stem. Laboratory markers (ESR, CRP, WBC count) are within normal limits. Aspiration of the hip joint yields a clear, viscous fluid. What is the most likely diagnosis?
Correct Answer: B
The clinical picture of increasing groin pain, leg length discrepancy, and classic radiographic lucencies (greater than 2mm in multiple zones) around both components, coupled with normal inflammatory markers and a clear joint aspirate, strongly points towards aseptic loosening. Periprosthetic joint infection would typically present with elevated inflammatory markers and potentially purulent aspirate, although chronic low-grade infections can be subtle. Heterotopic ossification can cause pain and stiffness but is usually identifiable on X-ray as mature bone formation and does not typically present with component lucencies. Stress shielding is a radiographic finding (bone resorption around the implant) that contributes to loosening but is not the primary diagnosis. Component impingement would cause activity-related pain and potentially dislocation, but not the specific radiographic findings of widespread lucency and subsidence.
A 72-year-old male with a history of hypertension and osteoporosis sustains a fall, resulting in a periprosthetic fracture of the femur around the stem of his 10-year-old cemented total knee arthroplasty. Radiographs reveal a Vancouver Type B2 fracture. What is the most appropriate management?
Correct Answer: D
A Vancouver Type B2 periprosthetic fracture involves a fracture around or distal to a stable femoral stem, with a loose femoral component. Given the described lucencies around the stem and the fracture, the femoral component is likely loose. Therefore, revision of the femoral component with a longer, cemented stem is the appropriate treatment, providing stability both proximally (by bypassing the fracture) and distally (by engaging healthy bone). Non-operative management is typically reserved for stable, non-displaced fractures (e.g., Vancouver Type C or some Type A). ORIF alone is insufficient as the component is loose. An uncemented stem might be considered in younger, healthier patients with good bone quality, but a cemented stem is often preferred in older patients with osteoporosis for immediate stability. Knee fusion is a salvage procedure typically reserved for failed revisions or severe infection.
A 65-year-old female presents with chronic, debilitating shoulder pain and weakness, severely limiting her activities of daily living. Physical examination reveals pseudoparalysis, a positive shoulder shrug sign, and severe limitations in active range of motion, particularly elevation and external rotation. Radiographs show severe glenohumeral osteoarthritis and superior migration of the humeral head with complete absence of the rotator cuff. She has failed extensive conservative management. Which surgical option is most appropriate?
Correct Answer: C
The constellation of severe glenohumeral osteoarthritis, superior migration of the humeral head, pseudoparalysis, and complete absence of the rotator cuff (referred to as 'rotator cuff arthropathy') are classic indications for a reverse total shoulder arthroplasty (rTSA). Anatomic total shoulder arthroplasty relies on an intact rotator cuff for function and stability. Hemiarthroplasty might address pain but would not restore function in the setting of pseudoparalysis. Arthroscopic debridement and rotator cuff repair are not feasible for a complete, irreparable cuff tear with arthropathy. Shoulder fusion is a salvage procedure for younger, higher-demand patients or failed arthroplasty, and would severely limit motion.
A 14-year-old obese male presents with a 3-month history of a painful limp and hip pain that radiates to his knee. He has limited internal rotation and abduction of the hip, and external rotation upon hip flexion (Drehmann sign). Radiographs of the hip show widening of the physis and posterior and inferior displacement of the epiphysis relative to the metaphysis. What is the most appropriate initial management?
Correct Answer: B
This clinical presentation is classic for Slipped Capital Femoral Epiphysis (SCFE), characterized by the Drehmann sign and radiographic findings. For stable SCFE, percutaneous pinning in situ with a single screw is the standard of care to prevent further slip and promote physeal closure. This approach minimizes complications and allows for early weight-bearing. Open reduction is reserved for unstable or severely displaced slips. Observation or casting is insufficient and risks progression. Traction and closed reduction are contraindicated due to the risk of avascular necrosis (AVN) as the slip is typically chronic and involves remodeling.
A 32-year-old construction worker presents with chronic wrist pain and tenderness in the anatomical snuffbox after falling onto an outstretched hand 6 months ago. Initial radiographs taken at an urgent care clinic were reported as normal, and he was treated conservatively with a wrist brace. Current radiographs show a sclerotic nonunion of the scaphoid at the waist with evidence of early degenerative changes in the radiocarpal joint. What is the most appropriate next step in management?
Correct Answer: D
The presence of chronic pain, tenderness in the anatomical snuffbox, and radiographic evidence of a sclerotic scaphoid nonunion with early degenerative changes (SNAC wrist) indicates the need for surgical intervention. Percutaneous screw fixation is not appropriate for established nonunions, especially with sclerosis. Given the presence of a nonunion and early degenerative changes, a vascularized or non-vascularized bone graft with internal fixation (e.g., screw or K-wires) is the standard treatment to achieve union and prevent progression of osteoarthritis. Continued conservative management has failed. Excision of the fragment is not a reconstructive option. Wrist arthrodesis is a salvage procedure for advanced radiocarpal arthritis after failed reconstruction.
A 35-year-old male sustains a crush injury to his foot after a heavy object falls on it. He complains of severe midfoot pain and inability to bear weight. Physical examination reveals swelling and ecchymosis over the dorsum of the foot, tenderness at the tarsometatarsal joints, and subtle widening of the interval between the first and second toes. Plain radiographs are equivocal, but a weight-bearing radiograph shows diastasis between the medial cuneiform and the base of the second metatarsal. What is the most appropriate definitive management?
Correct Answer: B
The clinical presentation and radiographic findings (diastasis between medial cuneiform and second metatarsal base) are highly suggestive of a Lisfranc injury. Given the instability and potential for long-term functional impairment, surgical intervention is almost always indicated for displaced or unstable Lisfranc injuries. ORIF with screws (across the medial and intermediate cuneiforms to the second metatarsal base, and other unstable joints) is the standard of care for acute, displaced injuries to restore anatomical alignment and stability. Non-weight bearing in a cast is for stable, non-displaced injuries. Primary arthrodesis may be considered for chronic or highly comminuted injuries, or if severe degenerative changes are already present. Excision of the second metatarsal base is not a standard treatment. Early weight-bearing with a walking boot is contraindicated.
A 55-year-old male presents with worsening lower back pain, bilateral leg numbness, and progressive weakness, particularly in his quadriceps muscles. He describes his symptoms as being worse with standing and walking, and relieved by sitting or leaning forward (shopping cart sign). Physical examination reveals diminished patellar reflexes and weak knee extension bilaterally. MRI shows severe degenerative changes at L3-L4 and L4-L5 with significant narrowing of the spinal canal. What is the most appropriate initial management approach?
Correct Answer: E
The patient's symptoms (neurogenic claudication, 'shopping cart sign,' motor weakness, diminished reflexes) are classic for lumbar spinal stenosis. The initial management for symptomatic lumbar spinal stenosis, especially without acute neurological deficits (e.g., cauda equina syndrome), is typically conservative. This involves a trial of NSAIDs, activity modification, and physical therapy focused on flexion exercises to open the spinal canal, improve posture, and strengthen core muscles. Epidural steroid injections can provide temporary symptomatic relief. Surgical decompression and fusion are reserved for those who fail conservative management or develop progressive neurological deficits. Rigid bracing is generally not effective and can lead to muscle atrophy. Progressive resistance exercises are often part of physical therapy but not a standalone initial approach.
A 16-year-old male presents with persistent knee pain, swelling, and a palpable mass in the distal femur. Radiographs show a lytic, destructive lesion with a 'sunburst' periosteal reaction and Codman's triangle in the metaphysis of the distal femur. A biopsy confirms osteosarcoma. Which of the following is the most important prognostic factor for this patient?
Correct Answer: D
The most important prognostic factor in osteosarcoma is the response to neoadjuvant chemotherapy (percentage of tumor necrosis). A good histological response (typically >90% necrosis) is strongly correlated with improved overall survival and decreased recurrence rates. While the presence of pulmonary metastases at diagnosis (Stage IV disease) is a very poor prognostic indicator, the *response to chemotherapy* is a dynamic and critical factor in determining the effectiveness of treatment and guiding subsequent surgical and adjuvant therapy. Age, tumor location, and tumor size are less significant than the chemotherapy response.
What is the most likely diagnosis?
A 50-year-old woman undergoes revision of a painful metal-on-metal hip resurfacing. Intraoperatively, a large cystic mass containing thick, necrotic fluid is found. Histopathological examination of the periprosthetic tissue is most likely to reveal which of the following?
A patient presents with persistent groin pain 3 years following a metal-on-metal hip resurfacing. Radiographs show well-fixed components without signs of loosening. Serum cobalt is 9.5 ppb. Which of the following is the most appropriate next step in the diagnostic workup?
None
