Developmental Dislocation Dysplasia: What Its Natural History Means
Introduction & Epidemiology
Developmental Dysplasia of the Hip (DDH), often previously termed congenital dislocation of the hip, encompasses a spectrum of conditions ranging from subtle acetabular dysplasia, characterized by an abnormally shallow or anteverted acetabulum, to complete irreducibility of the femoral head from the acetabulum. The critical understanding is that DDH represents a continuum of abnormal development rather than a static entity. The term "dysplasia" accurately reflects this developmental process, which can manifest in utero , perinatally, or even postnatally.
The natural history of untreated DDH is largely one of progressive deterioration of the hip joint. In cases of mild acetabular dysplasia, the hip may remain stable but is predisposed to developing secondary degenerative changes, including labral tears, articular cartilage damage, and femoroacetabular impingement (FAI), ultimately leading to early onset osteoarthritis. In instances of hip subluxation or frank dislocation, the femoral head and acetabulum undergo significant compensatory and maladaptive changes. The acetabulum becomes progressively shallower, more vertical, and often anteverted or retroverted, failing to develop its characteristic cup shape. The femoral head can flatten, develop an irregular shape, and the femoral neck may become increasingly anteverted. The capsule becomes hypertrophied and redundant, while the ligamentum teres elongates and thickens. The labrum, often inverted, can form a significant impediment to reduction. Over time, the dislocated hip leads to muscular contractures (e.g., adductors, iliopsoas), soft tissue scarring, and a false acetabulum forming on the ilium, typically superoposterior to the true acetabulum. This maladaptive remodeling places abnormal stresses across the developing joint, culminating in articular incongruity, chronic pain, and severe degenerative arthropathy requiring arthroplasty at a young age.
Epidemiologically, DDH is one of the most common musculoskeletal anomalies in neonates and infants, with an incidence varying from 0.1% to 2.0% in the general population, depending on diagnostic criteria and screening practices. There is a notable female predilection, with females affected 4 to 6 times more often than males. The left hip is more commonly involved than the right, with bilateral involvement occurring in approximately 20-30% of cases.
Key risk factors for DDH include:
*
Breech presentation:
Particularly frank breech, significantly increases risk due to sustained hip flexion and knee extension.
*
Firstborn status:
May be related to relatively tight uterine environment.
*
Oligohydramnios:
Restricts fetal movement and increases mechanical forces on the hips.
*
Positive family history:
Suggests a genetic predisposition, though the exact genetic markers are complex and multifactorial.
*
Concomitant congenital anomalies:
Such as metatarsus adductus, calcaneovalgus foot, or congenital muscular torticollis.
The understanding of DDH pathogenesis has evolved. While often considered present at birth, its development can extend into a child's first year of life. Recent research underscores the role of postnatal environmental factors, particularly improper swaddling practices. The seed content correctly notes that "babies whose legs are swaddled tightly with the hips and knees straight are at a notably higher risk for developing DDH after birth." This mechanical constraint in an adducted and extended position impedes normal hip development, which optimally occurs in a position of flexion and abduction. This highlights the interplay between genetic predisposition, in utero positioning, and postnatal environmental influences on the formation and stability of the hip joint. The initial statement from the seed content, "In utero, the hip with DDH is thought to form normally during the fetal period of development and to undergo abnormal growth of the chondroosseous components during the embryonic period," reflects one theory of pathogenesis, suggesting that while initial formation might be undisturbed, subsequent growth and maturation, particularly of the cartilage and bone, are aberrant, leading to the spectrum of dysplasia observed. This reinforces the "developmental" aspect of DDH.
Surgical Anatomy & Biomechanics
A comprehensive understanding of the normal and pathological anatomy of the hip is paramount for effective diagnosis and surgical management of DDH.
Normal Hip Anatomy:
The hip is a diarthrodial, ball-and-socket joint designed for stability and mobility.
*
Bony Anatomy:
The acetabulum, formed by the fusion of the ilium, ischium, and pubis, is a hemispherical socket providing coverage for the femoral head. The triradiate cartilage, which fuses between ages 12-16, is crucial for acetabular growth. The femoral head is spherical, and the femoral neck connects it to the shaft, typically with 10-20 degrees of anteversion (angle between the femoral neck axis and the transcondylar axis of the distal femur) and a neck-shaft angle of approximately 130 degrees in adults.
*
Articular Cartilage:
Covers the weight-bearing surfaces of the femoral head and acetabulum, providing a low-friction surface.
*
Acetabular Labrum:
A fibrocartilaginous rim that deepens the acetabular socket and contributes to negative intra-articular pressure, enhancing stability.
*
Capsule and Ligaments:
The strong fibrous capsule extends from the acetabular rim to the femoral neck. Key ligaments reinforce the capsule:
*
Iliofemoral ligament (Y-ligament of Bigelow):
Anteriorly, limits hip extension.
*
Pubofemoral ligament:
Anteromedially, limits abduction and extension.
*
Ischiofemoral ligament:
Posteriorly, limits extension and internal rotation.
*
Ligamentum Teres:
Intracapsular, connects the fovea capitis to the acetabular notch, containing a branch of the obturator artery (artery of the ligamentum teres). Its role in adult hip stability is minor, but it can hypertrophy and impede reduction in DDH.
*
Musculature:
The iliopsoas, gluteal muscles (maximus, medius, minimus), adductors, and hamstrings provide dynamic stability and motion.
Pathoanatomy of DDH:
In DDH, multiple structures can be affected, often compounding the instability or irreducibility.
*
Acetabular Dysplasia:
This is the hallmark of DDH. The acetabulum is typically shallow, more vertical, and often deficient in its lateral and anterior coverage. This can be quantified by radiographic parameters such as:
*
Acetabular Index (AI):
Angle between a line from the triradiate cartilage to the lateral acetabular edge and a horizontal line through the triradiate cartilage. Increased AI indicates a more shallow acetabulum.
*
Center-Edge (CE) Angle of Wiberg:
Angle between a vertical line through the center of the femoral head and a line from the center of the femoral head to the lateral edge of the acetabulum. Reduced CE angle signifies inadequate lateral coverage.
*
Acetabular Anteversion:
The acetabulum can be abnormally anteverted or retroverted, contributing to instability or impingement.
*
Femoral Head and Neck Dysplasia:
* In a dislocated hip, the femoral head often flattens posteromedially due to pressure against the ilium.
* The femoral neck may exhibit excessive anteversion, which can lead to hip instability and contribute to an 'in-toeing' gait.
* There may be coxa valga, an increased femoral neck-shaft angle, further compromising stability.
*
Capsular Changes:
The hip capsule becomes hypertrophied, thickened, and redundant, particularly in chronic dislocations. The inferomedial capsule may constrict, creating an 'hourglass' deformity that prevents concentric reduction.
*
Acetabular Labrum:
Inverted or hypertrophied labrum is a common soft tissue impediment to reduction, particularly in dislocated hips. It can fold into the acetabulum, blocking the femoral head from seating.
*
Ligamentum Teres and Pulvinar:
In dislocated hips, the ligamentum teres often hypertrophies and elongates. The pulvinar, a fatty pad within the acetabular notch, can also hypertrophy, filling the acetabulum and hindering reduction.
*
Muscle Contractures:
With chronic dislocation, the adductor muscles, iliopsoas, and often hamstrings become severely contracted and shortened, contributing to the difficulty of reduction.
Biomechanics:
The biomechanics of a normal hip involve efficient load transfer and stability. The spherical femoral head articulates precisely within the acetabulum, distributing forces evenly across the articular cartilage. In DDH, this biomechanical equilibrium is disrupted. Inadequate acetabular coverage leads to increased stress concentrations on a smaller portion of the femoral head and acetabulum, predisposing to early cartilage degeneration. The altered lever arms and muscle imbalances result in inefficient gait patterns and compensatory mechanisms, further accelerating the degenerative process. Surgical interventions for DDH aim to restore normal anatomy and biomechanics by achieving stable, concentric reduction and improving acetabular coverage to normalize joint reaction forces and promote healthy joint development.
Indications & Contraindications
The decision-making process for DDH management is complex, relying heavily on the patient's age, hip stability, degree of dysplasia, and the presence of associated deformities. The overall goal is to achieve and maintain a concentric, stable, and anatomically correct reduction of the femoral head within the acetabulum, thereby promoting normal hip development and preventing long-term sequelae such as osteoarthritis.
Non-Operative Indications:
Non-operative management is the cornerstone of treatment for neonates and young infants with unstable or reducible hips.
*
Neonates (0-6 weeks):
Observation is often indicated for Graf type IIa hips (physiologic immaturity) that are clinically stable. Serial ultrasound monitoring is crucial.
*
Infants < 6-9 months:
The primary non-operative treatment for unstable or reducible hips (subluxation or dislocation) is the
Pavlik harness
. This dynamic abduction brace maintains the hips in a position of flexion (100-110 degrees) and abduction (40-60 degrees), which is within the "safe zone" for hip reduction, while allowing knee and some hip motion.
*
Indications for Pavlik harness:
Clinically positive Ortolani or Barlow maneuvers, ultrasound-confirmed reducible subluxation or dislocation (Graf type IIb, IIc, D, IIIa), or persistent dysplasia (Graf type IIa-) after 3 weeks of age.
*
Failure of non-operative management:
Persistent instability or lack of reduction after 3-4 weeks in a Pavlik harness typically mandates progression to operative intervention.
Operative Indications:
Operative management is considered when non-operative methods fail, when the hip is irreducible, or when the patient presents at an older age with established deformity.
-
Closed Reduction with Spica Cast:
- Age: Primarily for infants 6 months to 18 months, or younger infants where Pavlik harness failed.
- Hip Status: Reducible dislocation that cannot be managed with a Pavlik harness, often due to soft tissue contractures (e.g., adductor tightness) necessitating preliminary adductor tenotomy.
- Technique: Performed under general anesthesia. May involve adductor tenotomy and/or iliopsoas release. Gentle manipulation to reduce the hip. Reduction confirmed by arthrography and fluoroscopy. Spica cast applied to maintain reduction.
-
Open Reduction with Spica Cast:
- Age: Typically for children > 18 months of age, or younger children with irreducible dislocations (e.g., due to inverted labrum, hypertrophied pulvinar, hourglass constriction of the capsule, or significant muscle contractures).
- Hip Status: Irreducible dislocation or failure of closed reduction.
- Technique: Direct visualization of the joint allows for removal of all soft tissue impediments to reduction (e.g., labral inversion, pulvinar excision, ligamentum teres resection, capsulotomy/capsulorrhaphy). Spica cast applied post-reduction.
-
Combined Open Reduction with Femoral Osteotomy and/or Pelvic Osteotomy:
- Age: Generally for children > 18-24 months of age, where established bony deformities (acetabular dysplasia, excessive femoral anteversion, coxa valga) are present alongside dislocation.
- Femoral Shortening/Derotation Osteotomy: Indicated in older children with significant femoral head displacement and shortening of surrounding soft tissues. This reduces tension on neurovascular structures, facilitates reduction, and reduces the risk of iatrogenic avascular necrosis (AVN). Derotation addresses excessive femoral anteversion.
-
Pelvic Osteotomies (Acetabuloplasty):
Used to improve acetabular coverage and containment of the femoral head. Choice of osteotomy depends on age, triradiate cartilage status, and specific acetabular deficiency.
- Salter Innominate Osteotomy: For children 1-8 years with open triradiate cartilage. Redirection of the entire acetabulum.
- Dega Osteotomy / Pemberton Pericapsular Osteotomy: For children with open triradiate cartilage, addressing specific areas of acetabular deficiency, creating a more congruent socket.
- Periacetabular Osteotomy (PAO) (Ganz Osteotomy): For adolescents and young adults with closed triradiate cartilage, good joint congruency, and minimal to no degenerative changes. Allows multidirectional correction of acetabular orientation.
-
Total Hip Arthroplasty (THA):
- Age: Adults with severe, symptomatic degenerative arthritis secondary to long-standing DDH or failed previous surgical attempts, particularly in cases where salvage osteotomies are no longer viable.
Contraindications (Relative and Absolute):
*
Absolute:
Active infection (systemic or local), severe underlying medical comorbidities precluding anesthesia or surgery, severe neurological impairment where surgical benefits are unlikely to improve function.
*
Relative:
* Severe avascular necrosis (AVN) of the femoral head may contraindicate certain osteotomies, as the goal is joint preservation.
* Extremely severe, chronic dislocations in older children/adolescents where successful reduction carries very high risk of AVN, nerve injury, or severe stiffness; sometimes a staged approach or palliative care is chosen.
* Failure to adhere to post-operative protocols (e.g., spica cast care) can be a relative contraindication to complex procedures.
Summary of Operative vs. Non-Operative Indications:
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Age | Neonates to ~9 months | > 6-9 months, or failure of non-op, or late presentation |
| Hip Status | Reducible instability/dysplasia (Graf types IIa-, I, IIb, IIc, D) | Irreducible dislocation (Graf III, IV), persistent subluxation, significant acetabular/femoral dysplasia |
| Imaging | Ultrasonography (0-6 months) for diagnosis and monitoring; Radiographs for confirmation. | Radiographs (AP pelvis, Frog-leg lateral) for bony anatomy; CT/MRI for detailed bony/soft tissue assessment (impede reduction) |
| Treatment Goals | Achieve stable concentric reduction, promote acetabular remodeling via dynamic bracing | Achieve and maintain stable, concentric reduction; restore normal anatomy; correct bony deformities; prevent future degenerative changes |
| Examples | Observation, Pavlik harness, abduction orthosis | Closed reduction + spica; Open reduction + spica; Femoral shortening osteotomy; Pelvic osteotomies (Salter, Dega, Pemberton, PAO); Total Hip Arthroplasty (adults with advanced arthritis) |
| Primary Risks | Failure to achieve reduction, AVN from prolonged extreme abduction, skin irritation | AVN, redislocation, nerve injury, infection, leg length discrepancy, hardware complications, stiffness |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for optimizing outcomes and minimizing complications in DDH surgery.
Pre-Operative Planning:
1.
Clinical Assessment:
* Thorough history: Age of presentation, risk factors (breech, family history, swaddling), previous treatments and their efficacy.
* Physical examination: Assess hip stability (Ortolani, Barlow in infants), range of motion, presence of Galeazzi sign, skin creases, leg length discrepancy, Trendelenburg gait in older children. Document neurovascular status.
2.
Imaging Review:
*
Radiographs:
Anteroposterior (AP) pelvis and frog-leg lateral views are standard. Evaluate for Hilgenreiner's line, Perkin's line, Shenton's line, acetabular index, CE angle, femoral head ossification, and morphology. Serial films are essential for monitoring.
*
Ultrasound (for infants < 6-9 months):
Gold standard for diagnosis and monitoring of early DDH. Evaluates femoral head coverage (alpha and beta angles), labral position, and dynamic stability.
*
CT Scan:
Provides detailed 3D bony anatomy, excellent for pre-operative planning of osteotomies (e.g., femoral derotation, PAO) to accurately measure femoral anteversion, acetabular version, and assess precise fragment repositioning. Crucial for understanding bony constraints.
*
MRI:
Best for visualizing soft tissue impediments (labrum, pulvinar, ligamentum teres, capsule) and assessing femoral head vascularity or early AVN, especially in cases of suspected challenging reduction or persistent instability. MR arthrography can further delineate intra-articular pathology.
3.
Surgical Strategy & Templating:
*
Procedure Selection:
Based on age, degree of dislocation, reducibility, and associated bony deformities (acetabular dysplasia, femoral anteversion/coxa valga).
*
Osteotomy Planning:
If pelvic or femoral osteotomies are indicated, precise templating using CT reconstructions helps determine the amount of correction needed, the osteotomy cuts, and appropriate hardware (plates, screws, K-wires). Consider potential for bone graft harvest (iliac crest autograft) for pelvic osteotomies.
*
Soft Tissue Releases:
Anticipate the need for adductor tenotomy, iliopsoas release, or rectus femoris lengthening.
*
Hardware Selection:
Select appropriate-sized K-wires, screws, and plates for osteotomies based on patient age and bone size.
4.
Blood Management:
For older children or complex osteotomies, discuss potential blood loss and ensure availability of cross-matched blood products.
5.
Pre-operative Traction:
In older children (>2 years) with high, chronic dislocations, a period of skeletal traction (e.g., 2-3 weeks) may be employed to gradually stretch contracted soft tissues, descend the femoral head, and reduce the tension required for reduction, thereby potentially reducing the risk of AVN or nerve injury. This is a topic of ongoing debate and not universally practiced.
Patient Positioning:
1.
Operating Table:
A radiolucent operating table is essential for intraoperative fluoroscopic imaging. A specialized pediatric orthopedic table may be beneficial for complex osteotomies requiring specific hip positioning.
2.
Supine Position:
Most open reductions and pelvic osteotomies (e.g., Salter, Dega, Pemberton, PAO) are performed with the patient in a supine position.
*
Padding:
All pressure points (heels, sacrum, occiput, elbows, ulnar nerves) must be meticulously padded to prevent pressure sores or nerve palsies.
*
C-arm Access:
Ensure unrestricted C-arm access for AP and lateral views of the hip and pelvis throughout the procedure. The affected hip is typically positioned near the edge of the table.
*
Leg Preparation:
The affected limb (and often the contralateral limb) is prepped and draped freely to allow for full range of motion, manipulation, and access to potential bone graft sites (e.g., ipsilateral iliac crest).
*
Contralateral Limb:
The contralateral limb can be placed in a frog-leg position or abducted slightly to allow C-arm access for AP views of the affected hip without obstruction.
*
Spica Cast Preparation:
For procedures requiring post-operative spica casting, ensure the patient is positioned to facilitate cast application without repositioning after draping and osteotomy. Special spica cast tables may be used at the end of the procedure.
3.
Temperature Management:
Especially in infants and young children, maintain normothermia with warming blankets and fluid warmers.
4.
Urinary Catheter:
Usually inserted for longer procedures to monitor output.
Detailed Surgical Approach / Technique
Surgical techniques for DDH are diverse, tailored to the patient's age, reducibility, and the specific pathoanatomy. The overarching principles are to achieve a stable, concentric reduction, address all soft tissue and bony constraints, preserve femoral head vascularity, and promote normal hip development.
Closed Reduction with Adductor Tenotomy (for infants 6-18 months)
This is typically the first operative step for older infants who fail Pavlik harness or present with a reducible but tight hip.
1.
Anesthesia and Examination:
Under general anesthesia, a thorough examination of hip stability and range of motion is performed.
2.
Adductor Tenotomy:
A small transverse or longitudinal incision is made in the groin crease. The adductor longus tendon is identified and tenotomized near its origin. If needed, the adductor brevis or gracilis may also be partially released. Hemostasis is achieved. This releases adductor contracture, facilitating reduction.
3.
Reduction Maneuver:
The hip is gently flexed to 90 degrees, gradually abducted, and externally rotated while applying gentle longitudinal traction. An audible "clunk" or palpable click may indicate reduction. Excessive force is avoided to minimize AVN risk.
4.
Arthrography:
A contrast agent is injected into the hip joint under fluoroscopic guidance to confirm concentric reduction. The teardrop sign, position of the femoral head relative to the acetabulum, and absence of an inverted labrum or hourglass constriction are assessed. The "safe zone" of stability is identified.
5.
Spica Cast Application:
A one-and-a-half or double hip spica cast is applied, maintaining the hip in the identified safe zone, typically 90-100 degrees of flexion, 45-60 degrees of abduction, and slight internal rotation. Over-abduction must be avoided to prevent AVN.
Open Reduction (for irreducible hips, typically > 6 months)
A. Anteromedial Approach (Medial Ludloff Approach modified):
*
Indications:
Often used for infants <1 year with irreducible hip due to soft tissue constraints. Provides direct access to the joint's inferior aspects.
*
Incision:
Longitudinal incision in the adductor region, medial to the femoral neurovascular bundle.
*
Internervous Plane:
Between the adductor longus and pectineus muscles. The adductor longus is retracted medially, and the pectineus laterally.
*
Dissection:
The femoral vessels and nerve are identified and protected laterally. The obturator nerve is identified as it branches to the adductor muscles. The adductor longus and gracilis tendons are transected. The pectineus muscle origin may be released. The anterior branch of the obturator nerve can be a landmark.
*
Capsulotomy:
The anterior and inferior capsule is exposed. A T-shaped or inverted T-shaped capsulotomy is performed.
*
Soft Tissue Release:
Hypertrophied pulvinar and ligamentum teres are excised. An inverted labrum is identified and everted or partially resected if it impedes reduction. The "hourglass" constriction of the capsule is released.
*
Reduction:
The femoral head is gently reduced into the true acetabulum under direct vision.
*
Capsulorrhaphy:
The capsule is repaired and tightened (capsulorrhaphy) to enhance stability.
*
Closure:
Muscle layers are repaired, and skin is closed. Spica cast applied.
B. Anterolateral Approach (Smith-Petersen / Iliofemoral Approach):
*
Indications:
Most common approach for open reduction and pelvic osteotomies in children >1 year. Provides excellent exposure of the hip joint and acetabulum.
*
Incision:
Oblique incision originating from the anterior superior iliac spine (ASIS), extending distally and slightly laterally.
*
Internervous Plane:
Between the sartorius (femoral nerve) and the tensor fascia lata (superior gluteal nerve).
*
Dissection:
The superficial fascia is incised. The interval between the sartorius and tensor fascia lata is developed. The sartorius and rectus femoris are retracted medially (care with lateral femoral cutaneous nerve). The tensor fascia lata and gluteus medius/minimus are retracted laterally. The ascending branch of the lateral femoral circumflex artery is typically ligated.
*
Iliopsoas Release:
The iliopsoas tendon, which often constricts the femoral neck and can impede reduction, is identified and released from its insertion on the lesser trochanter. This may be done as a Z-lengthening.
*
Capsulotomy:
The capsule is incised (often an inverted T-capsulotomy) to expose the femoral head and acetabulum.
*
Soft Tissue Release & Reduction:
Same as medial approach: removal of pulvinar, ligamentum teres, eversion/resection of inverted labrum, release of hourglass constriction. The femoral head is reduced.
*
Capsulorrhaphy:
The capsule is repaired and tightened to prevent redislocation.
*
Closure:
Muscle layers are repaired, and skin is closed. Spica cast is applied. This approach often transitions directly into a pelvic osteotomy if indicated.
Pelvic Osteotomies (Performed via Anterolateral Approach)
-
Salter Innominate Osteotomy:
- Indications: Children aged 1-8 years with significant acetabular dysplasia, stable reduction, and open triradiate cartilage. Redirectional osteotomy.
- Technique: After open reduction and capsulorrhaphy (if performed), the inner and outer tables of the ilium are exposed from the ASIS to the greater sciatic notch. The osteotomy line is marked from the ASIS to the greater sciatic notch, just superior to the anterior inferior iliac spine (AIIS). A curved osteotome or saw is used to complete the osteotomy through the ilium. The distal fragment, containing the acetabulum, is then mobilized. The distal fragment is rotated laterally and anteriorly to cover the femoral head. A trapezoidal bone graft (typically harvested from the anterior superior iliac crest) is wedged into the gap created by the rotation, and the osteotomy is fixed with two or three K-wires or screws spanning the osteotomy.
-
Dega Osteotomy:
- Indications: For children with posterior-superior acetabular deficiency and an open triradiate cartilage. Pericapsular osteotomy creating a "shelf" effect.
- Technique: After exposure via anterolateral approach, the inner cortical table of the ilium is osteotomized from the greater sciatic notch to the ASIS, just above the anterior inferior iliac spine. The outer cortical table is then osteotomized along a similar line but is outfractured inferiorly, creating a flap that is hinged on the inner cortical table at the triradiate cartilage. A bone graft is inserted into the created gap to maintain the outfractured position, providing better lateral and posterior-superior coverage. Fixation with K-wires or screws.
-
Pemberton Pericapsular Osteotomy:
- Indications: For children with open triradiate cartilage, aiming to create a more spherical acetabulum.
- Technique: Exposure via anterolateral approach. The osteotomy begins at the ASIS, extends curvedly just superior to the AIIS, and proceeds posteriorly, passing through the ilium superior to the hip capsule, to terminate at the triradiate cartilage. The acetabular fragment is then pivoted downwards on the triradiate cartilage, effectively deepening the socket. A bone graft is wedged into the superior aspect of the osteotomy, and fixation is achieved with K-wires.
-
Periacetabular Osteotomy (PAO) (Ganz Osteotomy):
- Indications: Adolescents and young adults (closed triradiate cartilage) with symptomatic acetabular dysplasia and good joint congruency, aiming to preserve the native hip joint.
-
Technique:
Requires extensive exposure, often through a modified Smith-Petersen approach (Bikini incision) or a two-incision approach. The ilioinguinal approach is sometimes used. Multiple osteotomies are performed:
- Through the ilium above the acetabulum (supra-acetabular).
- Through the ischium just below the acetabulum (ischial osteotomy).
- Through the superior pubic ramus (pubic osteotomy).
- Through the posterior column (sciatic notch osteotomy).
- The entire acetabular fragment is carefully mobilized, allowing for multiplanar correction of its orientation (lateralization, anteversion/retroversion, flexion/extension) to optimize femoral head coverage.
- Once optimal position is achieved, the fragment is fixed with multiple screws. The advantages include preservation of the posterior column, allowing earlier weight-bearing, and the ability to correct in multiple planes.
Femoral Osteotomies
- Indications: Often performed concurrently with open reduction and/or pelvic osteotomies in older children (>18-24 months) with high dislocations or excessive femoral anteversion/coxa valga.
-
Subtrochanteric Shortening and Derotation Osteotomy:
- Technique: A lateral incision is made over the proximal femur. The vastus lateralis is incised and elevated. A transverse or oblique osteotomy is performed in the subtrochanteric region. A segment of bone is resected to achieve shortening (typically 1.5-3 cm, to reduce tension on neurovascular structures and facilitate reduction). The distal fragment is then derotated to correct excessive femoral anteversion. The osteotomy is fixed with a pediatric hip plate and screws. This procedure is crucial to prevent excessive tension on the femoral neurovascular bundle, which is a major risk factor for AVN.
-
Varus Derotation Osteotomy (VDRO):
- Indications: To correct excessive femoral anteversion and/or coxa valga, or to offload a specific area of AVN.
- Technique: Similar approach, but involves a wedge resection to create a varus correction, combined with derotation.
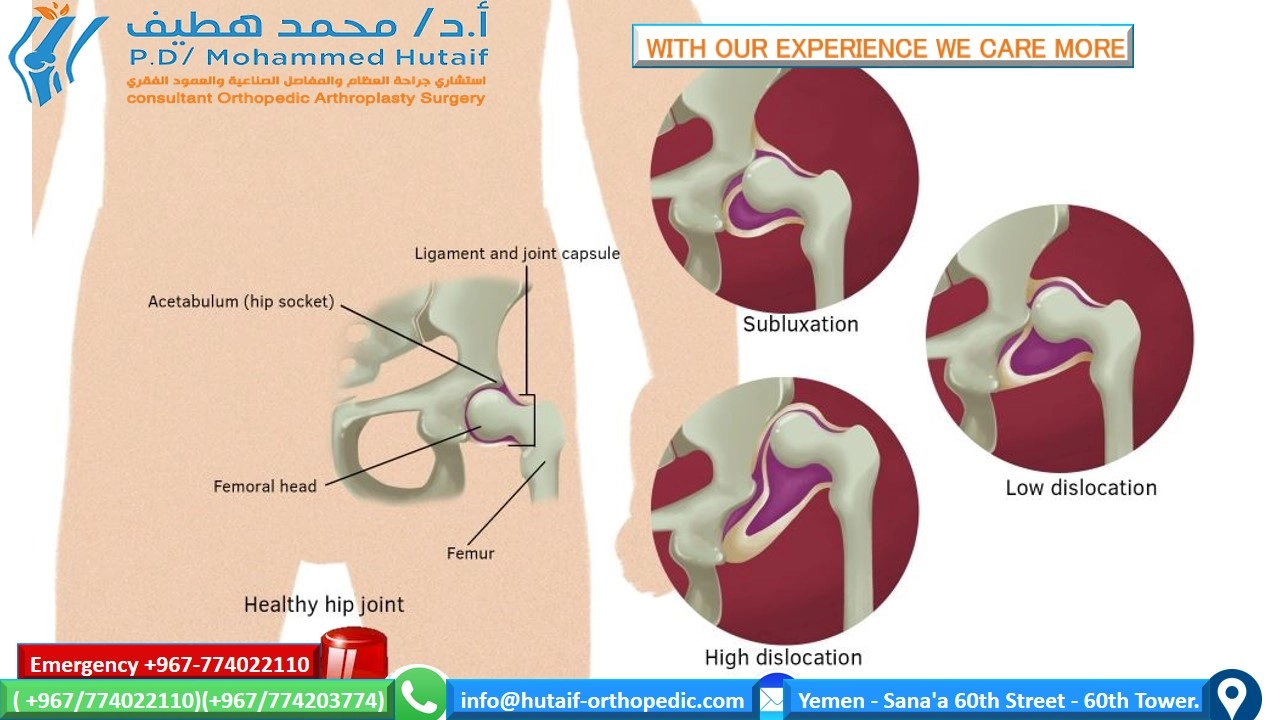
Image Integration:
The provided image

can be interpreted as a diagram depicting the basic pathology of DDH, potentially showing a dislocated or dysplastic hip joint with an abnormally shallow acetabulum and superiorly migrated femoral head. This serves to illustrate the fundamental anatomical alterations that guide the surgical planning and execution described above.
Complications & Management
Despite advancements in surgical techniques, complications associated with DDH surgery remain a significant concern, particularly avascular necrosis of the femoral head.
-
Avascular Necrosis (AVN) of the Femoral Head:
- Incidence: Varies widely (5-70%), influenced by patient age, severity of dislocation, initial reduction force, degree of femoral shortening, vascular anatomy, and post-operative casting position. Children >1 year undergoing open reduction have a higher risk.
- Pathophysiology: Ischemia of the femoral head epiphysis, typically due to compromise of the lateral epiphyseal vessels.
- Diagnosis: Radiographic signs (ossification delay, fragmentation, sclerosis, collapse) on serial follow-up. MRI is sensitive for early detection.
-
Management:
- Prevention is key: Gentle reduction maneuvers, adequate soft tissue release (e.g., femoral shortening), avoiding extreme abduction in casts.
- Observation: For mild changes (Salter-Harris type I/II).
- Containment: Femoral varus derotation osteotomy (VDRO) to offload the necrotic segment and improve coverage. Pelvic osteotomy for better containment.
- Salvage: In severe collapse and incongruity, hip arthroscopy for FAI, possibly leading to hip fusion or total hip arthroplasty (THA) in young adulthood.
-
Redislocation/Subluxation:
- Incidence: 5-15% after open reduction, higher after closed reduction.
- Pathophysiology: Inadequate reduction, insufficient soft tissue release, improper cast application, or failure of capsulorrhaphy/osteotomy fixation.
-
Management:
- Early: Adjust cast, repeat closed reduction (if stable).
- Late/Persistent: Revision open reduction, revision pelvic/femoral osteotomy to achieve stable containment.
-
Nerve Palsy (Femoral, Sciatic, Lateral Femoral Cutaneous):
- Incidence: Rare (1-5%), typically transient. Femoral nerve palsy can occur with excessive traction or limb lengthening. Sciatic nerve palsy is less common but more severe. Lateral femoral cutaneous nerve irritation is common with ilioinguinal approaches or retractors.
- Pathophysiology: Stretch injury, direct compression, or entrapment.
-
Management:
- Prevention: Careful positioning, controlled lengthening (femoral shortening osteotomy).
- Post-op: Observe, supportive care. Most resolve spontaneously. Surgical exploration rarely indicated for persistent deficits.
-
Infection:
- Incidence: Low (<1-2%).
- Management: Antibiotics (broad-spectrum, then culture-directed). Surgical debridement for deep infections. Hardware removal if persistent.
-
Leg Length Discrepancy (LLD):
- Incidence: Common, especially in unilateral cases, or with AVN affecting the physis. Femoral shortening osteotomy can also lead to LLD if not perfectly symmetrical.
-
Management:
- Mild (<2 cm): Shoe lift.
- Moderate/Severe: Contralateral epiphysiodesis (for growing children) or limb lengthening procedures.
-
Hardware Complications:
- Incidence: Pin migration, breakage, loosening, screw prominence, irritation.
- Management: Symptomatic hardware removal after osteotomy healing. Revision fixation if osteotomy fails due to hardware.
-
Stiffness/Limited Range of Motion:
- Incidence: Variable, due to capsular scarring, heterotopic ossification, or inadequate rehabilitation.
- Management: Aggressive physiotherapy. Manipulation under anesthesia or arthrolysis may be considered for refractory cases.
-
Growth Disturbances:
- Incidence: Direct trauma to epiphyses during surgery or AVN affecting the growth plates can lead to growth arrest or deformity.
- Management: Monitor growth. Guided growth techniques or corrective osteotomies if significant deformity develops.
-
Future Osteoarthritis:
- Incidence: Even with successful treatment, the risk of early osteoarthritis remains elevated, especially if residual dysplasia or AVN is present.
- Management: Palliative care, activity modification, eventually THA for severe, symptomatic arthritis.
Table of Common Complications, Incidence, and Salvage Strategies:
| Complication | Incidence | Salvage/Management Strategies |
|---|---|---|
| Avascular Necrosis (AVN) | 5-70% (variable) |
Prevention:
Gentle reduction, femoral shortening, safe cast position.
Management: Observation, protected weight-bearing, VDRO, pelvic osteotomy, THA (severe). |
| Redislocation/Subluxation | 5-15% |
Prevention:
Meticulous reduction, stable fixation, appropriate cast.
Management: Cast adjustment, repeat reduction (closed/open), revision osteotomy. |
| Nerve Palsy (Femoral/Sciatic) | 1-5% (transient) |
Prevention:
Controlled lengthening, careful retraction.
Management: Observation, supportive care; rarely surgical exploration. |
| Infection | <1-2% |
Prevention:
Aseptic technique, prophylactic antibiotics.
Management: Antibiotics, debridement, hardware removal (if persistent). |
| Leg Length Discrepancy (LLD) | Common |
Prevention:
Consider femoral shortening in older children.
Management: Shoe lift, contralateral epiphysiodesis, limb lengthening. |
| Hardware Complications | Variable |
Prevention:
Correct sizing, proper placement.
Management: Hardware removal, revision fixation (if failed osteotomy). |
| Stiffness/ROM limitation | Variable |
Prevention:
Early, controlled mobilization.
Management: Physiotherapy, manipulation under anesthesia, arthrolysis. |
| Growth Disturbances | Variable |
Prevention:
Avoid physeal damage.
Management: Monitor, guided growth, corrective osteotomies. |
| Future Osteoarthritis | High (if poor outcome) |
Prevention:
Achieve optimal reduction and anatomy.
Management: Palliative care, THA. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as crucial as the surgery itself in achieving optimal long-term outcomes in DDH management. Protocols vary based on patient age, the specific surgical procedure, and surgeon preference, but generally follow a structured approach emphasizing protection, healing, and gradual return to function.
1. Spica Cast Management (Following Closed or Open Reduction, often with Osteotomies):
*
Duration:
Typically 6-12 weeks, depending on the patient's age and stability of reduction. Younger infants may require shorter periods (e.g., 6 weeks), while older children or those undergoing osteotomies may need 8-12 weeks.
*
Position:
The hip is maintained in the "safe zone" of flexion and abduction determined at the time of reduction. Over-abduction must be strictly avoided due to the increased risk of AVN.
*
Cast Care:
*
Neurovascular Checks:
Frequent monitoring of sensation, motor function, capillary refill, and pulse in the toes and feet is paramount to detect compartment syndrome or nerve compression.
*
Skin Care:
Daily inspection for pressure areas, irritation, or breakdown. Padding of cast edges and diaper changes are critical.
*
Hygiene:
Education of caregivers on sponge bathing, diapering, and cast cleaning.
*
Cast Changes:
May be performed periodically (e.g., every 3-4 weeks) for hygiene, skin inspection, or if cast becomes soiled/loose.
*
Weight-Bearing:
Non-weight-bearing is typically maintained in the spica cast.
2. After Spica Cast Removal:
*
Gradual Mobilization:
The hip will likely be stiff initially. Gentle passive and active range of motion exercises are initiated immediately. Avoid forced or aggressive stretching, especially into abduction or internal rotation, which could jeopardize the healing capsule or osteotomy.
*
Protected Weight-Bearing:
Gradual progression to weight-bearing, often starting with non-weight-bearing with crutches or walker for 2-4 weeks, followed by partial weight-bearing for another 2-4 weeks. Full weight-bearing is typically allowed after radiographic evidence of osteotomy healing (if performed), usually 8-12 weeks post-cast removal.
*
Physical Therapy Program:
*
Range of Motion:
Focus on regaining full, pain-free flexion, extension, abduction, adduction, and rotation.
*
Strengthening:
Progressive strengthening of hip abductors (gluteus medius, minimus), extensors (gluteus maximus, hamstrings), and core muscles to restore dynamic stability.
*
Gait Training:
Re-education of gait pattern, addressing any Trendelenburg or compensatory mechanisms.
*
Functional Activities:
Gradual return to age-appropriate activities and sports.
*
Bracing:
Some protocols advocate for a temporary abduction brace (e.g., Scottish Rite brace, abduction pillow) after cast removal, particularly in younger children or those with concerns for residual instability. This helps maintain a reduced position during sleep or non-weight-bearing periods.
3. Specific Considerations for Osteotomies:
*
Pelvic Osteotomies (Salter, Dega, Pemberton, PAO):
*
Bone Healing:
Radiographic follow-up is essential to monitor bone healing at the osteotomy site.
*
Weight-Bearing Restrictions:
Typically prolonged non-weight-bearing or protected weight-bearing for 6-12 weeks after cast removal, depending on the osteotomy and its stability, before progressing to full weight-bearing.
*
Hardware Removal:
K-wires are usually removed 6-8 weeks post-op. Plates and screws for PAO or Salter osteotomies may be removed 12-18 months post-op, or later, once bone healing is complete and if symptomatic.
*
Femoral Osteotomies:
*
Bone Healing:
Radiographic checks are critical for osteotomy union.
*
Weight-Bearing:
Similar protected weight-bearing protocols until healing is confirmed.
*
Hardware Removal:
Plates and screws are typically removed 12-18 months post-op or once bone is mature and remodeled.
4. Long-Term Follow-up:
*
Until Skeletal Maturity:
Patients require long-term clinical and radiographic follow-up until skeletal maturity to monitor for residual dysplasia, progression of AVN, development of LLD, femoral head deformity, and early degenerative changes.
*
Patient Counseling:
Ongoing education of patients and families regarding activity modifications, potential for future interventions (e.g., THA), and the importance of maintaining hip strength and flexibility.
*
MRI/CT Surveillance:
In select cases, MRI or CT scans may be indicated to evaluate for subtle residual anatomical abnormalities, early AVN, or to plan further interventions.
The goal of rehabilitation is not just to heal from surgery, but to foster optimal hip development, restore strength and function, and mitigate the long-term risks associated with DDH.
Summary of Key Literature / Guidelines
The management of DDH is continuously refined through ongoing research and the development of evidence-based guidelines. Key literature and professional society recommendations guide clinical practice.
1. Screening Guidelines:
*
American Academy of Pediatrics (AAP) and American Academy of Orthopaedic Surgeons (AAOS):
Both organizations emphasize selective screening based on risk factors rather than universal ultrasound screening, which is common in some European countries.
*
Physical Examination:
Crucial role of serial physical examinations (Ortolani and Barlow maneuvers in neonates/infants) at birth, well-child visits, and throughout the first year of life.
*
Risk Factors:
Universal screening for risk factors (breech presentation, family history of DDH, female sex, firstborn, congenital foot deformities, torticollis) with targeted imaging.
*
Imaging:
*
Ultrasound:
Recommended for infants with risk factors (e.g., breech presentation, positive family history) or equivocal physical exams from 4-6 weeks of age until femoral head ossification impedes visualization (around 6-9 months). Early imaging (<4 weeks) can lead to overdiagnosis of physiologic immaturity (Graf type IIa).
*
Radiographs:
Become the primary imaging modality after 6-9 months of age when ossification centers are well developed, allowing for reliable measurement of bony parameters (Acetabular Index, CE angle).
2. Treatment Algorithms and Key Studies:
*
Pavlik Harness:
The cornerstone of non-operative treatment for infants <6 months with reducible DDH.
*
Sucato et al. (POSNA/SRS 2017 Consensus Statement):
Emphasized specific safe zone positioning (hip flexion 100-110°, abduction 40-60°) to minimize AVN risk. Failure rates range from 5-20% and are higher in older infants or complete dislocations.
*
Weinstein et al. (J Bone Joint Surg Am, 1997):
Classic study highlighting long-term outcomes of Pavlik harness treatment, demonstrating high success rates when applied appropriately.
*
Closed Reduction:
For infants 6-18 months who fail Pavlik harness or present late. Success rates around 70-80%.
*
Optimal Cast Position:
Maintenance within the "safe zone" identified by arthrography or fluoroscopy to minimize AVN.
*
Open Reduction:
For irreducible hips or failure of closed reduction.
*
Coleman et al. (J Bone Joint Surg Am, 1956):
Described key soft tissue impediments to reduction (inverted labrum, hypertrophied pulvinar, hourglass capsule).
*
Geralis et al. (J Pediatr Orthop, 2011):
Review of techniques and outcomes for open reduction.
*
Pelvic Osteotomies (Salter, Dega, Pemberton, PAO):
*
Salter et al. (J Bone Joint Surg Am, 1961):
Original description of the innominate osteotomy.
*
Ganz et al. (J Bone Joint Surg Am, 1988):
Introduction of the Periacetabular Osteotomy (PAO), demonstrating its ability to preserve the posterior column and allow multiplanar correction, expanding surgical options for adolescents/young adults.
*
Leunig et al. (Clin Orthop Relat Res, 2009):
Extensive work on the PAO, defining indications, technique, and outcomes for hip preservation.
*
Femoral Osteotomies:
Primarily subtrochanteric shortening and derotation osteotomies.
*
Maarten et al. (J Pediatr Orthop, 2015):
Studies highlighting the reduction in AVN risk with femoral shortening in older children undergoing open reduction.
3. Complication Management:
*
Avascular Necrosis (AVN):
Remains the most dreaded complication.
*
Salter et al. Classification:
Often used to describe the severity and pattern of AVN.
*
Risk Factors:
Forceful reduction, extreme abduction in cast, older age at reduction, higher dislocation.
*
Management:
VDRO to prevent collapse, containment osteotomies.
*
Redislocation:
Indicates need for re-evaluation and potentially more aggressive surgical intervention.
4. Long-Term Outcomes:
*
Terminal Outcomes:
Numerous studies have shown that despite successful early treatment, patients with DDH have a higher risk of developing early hip osteoarthritis and requiring total hip arthroplasty at a younger age compared to the general population.
*
Schoenecker et al. (J Bone Joint Surg Am, 1984):
Long-term follow-up studies emphasize the importance of achieving and maintaining concentric reduction to optimize outcomes and delay onset of degenerative changes.
*
Wenger et al. (J Bone Joint Surg Am, 2011):
Review of long-term prognosis after surgical treatment of DDH.
*
Residual Dysplasia:
Even after successful reduction, residual acetabular dysplasia or femoral head/neck deformity can persist and may require secondary procedures (e.g., late pelvic osteotomies or femoral osteotomies) to improve hip mechanics and delay arthritis.
5. Current Trends and Debates:
*
Swaddling Practices:
Growing evidence links improper swaddling to increased DDH incidence, leading to public health campaigns for "hip-healthy swaddling."
*
Role of MRI:
Increasing use of MRI for complex cases, assessment of soft tissue pathology, and early detection of AVN.
*
Arthroscopy:
Emerging role of hip arthroscopy in identifying and treating soft tissue impediments to reduction in some cases, and for managing sequelae like FAI post-DDH treatment.
*
Best Time for Intervention:
The ongoing debate about the optimal age for specific interventions to balance success rates with complication risks (especially AVN).
This comprehensive review highlights the complex nature of DDH, its natural history of progressive degeneration if untreated, and the multi-faceted surgical approaches aimed at restoring hip anatomy and function. Continuous adherence to established guidelines and a critical appraisal of new literature are essential for providing optimal care.
