Introduction & Epidemiology
Developmental Dysplasia of the Hip (DDH) encompasses a spectrum of conditions ranging from subtle acetabular dysplasia to complete dislocation of the femoral head. It represents a significant orthopedic challenge due to its potential for long-term morbidity, including premature osteoarthritis, pain, and functional limitations if not diagnosed and treated effectively. The incidence of DDH varies widely, generally estimated between 1 and 3 per 1,000 live births, but can be significantly higher in populations with specific risk factors such as breech presentation (up to 10-fold increased risk), female sex (4-6 times more common), first-born status, oligohydramnios, and a positive family history. Early diagnosis is paramount, as non-operative treatment is highly successful in the neonatal period, while delayed diagnosis often necessitates more invasive surgical interventions.
The diagnostic process for DDH relies heavily on a combination of clinical examination and advanced imaging modalities, tailored to the patient's age and clinical presentation.
Clinical Assessment:
*
Neonates and Infants:
Emphasis on hip stability tests:
*
Ortolani maneuver:
Reduces a dislocated hip with a palpable "clunk."
*
Barlow maneuver:
Dislocates an unstable hip from a reduced position.
*
Galeazzi sign (Allis sign):
Apparent leg length discrepancy with flexed hips and knees, indicating unilateral dislocation.
* Limited hip abduction.
* Asymmetry of gluteal or thigh folds (less reliable).
*
Older Children and Adolescents:
* Trendelenburg gait (positive Trendelenburg sign) due to abductor muscle weakness in cases of superior migration of the femoral head.
* Limb length discrepancy.
* Pain, particularly with activity.
* Limited range of motion.
Imaging Modalities for DDH Diagnosis:
-
Dynamic Hip Ultrasound: This is the gold standard for detecting hip dysplasia in very young infants (generally under 6 months of age), prior to significant ossification of the femoral head and acetabulum.
- Technique: Performed by a trained sonographer using high-frequency transducers. Graff's method (coronal and transverse views) assesses acetabular morphology and femoral head coverage. Dynamic maneuvers (Barlow, Ortolani) are performed to assess reducibility and stability.
-
Parameters:
- Alpha angle: Angle between the baseline (ilium) and the bony acetabular roof. A normal hip has an alpha angle > 60 degrees.
- Beta angle: Angle between the baseline (ilium) and the cartilaginous labrum. This helps assess the quality of the cartilaginous roof.
- Femoral head coverage: Percentage of the femoral head covered by the acetabulum (should be >50%).
- Utility: Detects subtle acetabular dysplasia, subluxation, and frank dislocation. Essential for guiding Pavlik harness treatment and monitoring its effectiveness.
- Limitations: Highly operator-dependent; becomes less useful as ossification progresses.
-
Plain Radiographs: The primary diagnostic tool for older children (typically >4-6 months) when the ossific nucleus of the femoral head has developed sufficiently.
-
Views:
- Anteroposterior (AP) Pelvis View: Standard view with hips in neutral rotation and extension. Crucial for assessing bilateral hip morphology.
- Frog-leg Lateral View: Less common for initial DDH diagnosis, but can demonstrate anterior acetabular coverage or femoral head position.
- False Profile View (Lequesne and de Sèze view): Patient standing with affected hip at 65 degrees to the cassette, contralateral hip abducted 25 degrees. Provides a sagittal view of the hip joint, specifically evaluating anterior acetabular coverage.
-
Radiographic Parameters to Evaluate:
- Acetabular Index (AI): Angle formed by Hilgenreiner's line (horizontal line connecting triradiate cartilages) and a line drawn from the medial aspect of the triradiate cartilage to the lateral margin of the bony acetabulum. Normal AI < 28-30 degrees in newborns, decreasing with age. An increased AI indicates acetabular hypoplasia/dysplasia.
- Lateral Center-Edge Angle (LCEA) of Wiberg: Angle formed by a vertical line through the center of the femoral head and a line from the center of the femoral head to the lateral edge of the bony acetabulum. Normal LCEA > 20 degrees in children > 5 years, increasing with age. A decreased LCEA indicates inadequate lateral acetabular coverage.
- Anterior Center-Edge Angle (ACEA) of Lequesne and de Sèze: Measured on the false profile view. Angle between a vertical line through the center of the femoral head and a line from the center of the femoral head to the anterior edge of the bony acetabulum. Normal ACEA > 20 degrees. A decreased ACEA indicates inadequate anterior acetabular coverage.
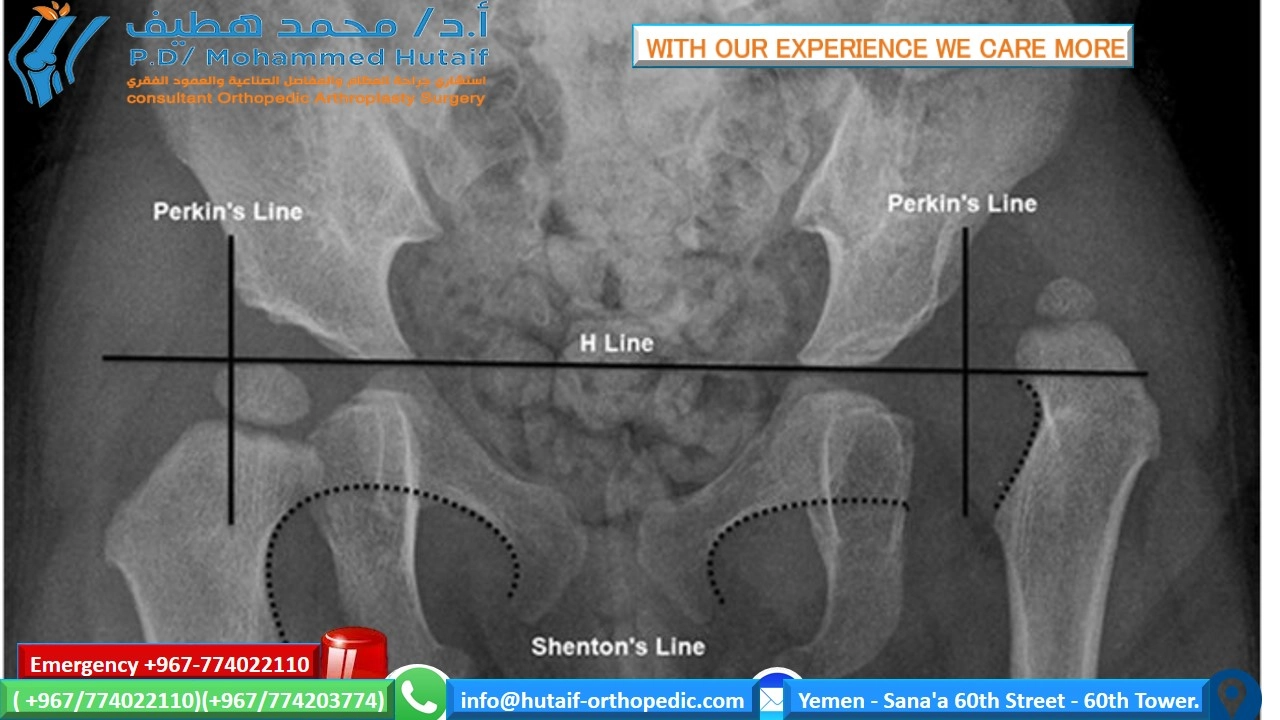
- Shenton's Line: A smooth, continuous arc formed by the medial margin of the femoral neck and the inferior margin of the superior pubic ramus. A break in Shenton's line (discontinuity) suggests subluxation or dislocation of the femoral head.
- Perkin's Line: A vertical line drawn from the lateral edge of the acetabulum, perpendicular to Hilgenreiner's line. The femoral head's ossific nucleus should lie inferomedial to the intersection of Hilgenreiner's and Perkin's lines.
- Ossific Nucleus: Location, size, and symmetry of the femoral head ossific nucleus are assessed. Delayed or lateralized ossification can indicate pathology.
- Sourcil (Roof of the Acetabulum): The superolateral margin of the acetabulum. Its shape and orientation are critical indicators of acetabular dysplasia. A flattened or oblique sourcil indicates inadequate containment.
- "Hip-at-risk" radiograph: A pelvic radiograph with the legs abducted and internally rotated can give some idea about the ability of the hip to reduce and the congruity of the joint, often performed pre-operatively for closed or open reduction planning, or to assess post-operative stability/coverage.
- Interpretation: Dislocation is detected by a complete lack of contact between the acetabulum and femoral head, with the femoral head typically superior and lateral to Perkin's line. Subluxation is characterized by partial contact, often with a break in Shenton's line. Acetabular dysplasia is indicated by an increased acetabular index, decreased LCEA, or decreased ACEA.
-
Views:
-
Computed Tomography (CT) Scan:
- Utility: Provides detailed three-dimensional assessment of bony anatomy, particularly useful for assessing femoral head reduction and acetabular coverage post-reduction (e.g., after closed reduction and spica cast application) or for complex pre-operative planning. It can precisely measure anterior and lateral coverage, femoral anteversion, and acetabular version.
- Limitations: Ionizing radiation exposure, particularly a concern in pediatric patients. Often reserved for specific indications where plain radiographs are insufficient or ambiguous.
-
Magnetic Resonance Imaging (MRI):
- Utility: Offers excellent visualization of soft tissues, including the acetabular labrum, articular cartilage, joint capsule, ligamentum teres, and psoas tendon. It can identify impediments to reduction (e.g., inverted labrum, hypertrophied pulvinar, constricted capsule) that are not visible on radiographs or CT.
- Indications: Increasingly used in pre-operative planning for open reduction, especially in older infants, to delineate soft tissue pathology and guide the surgical approach. It is also valuable in evaluating avascular necrosis (AVN) of the femoral head.
- Limitations: Requires sedation in young children, higher cost, and longer acquisition time compared to CT.
The choice of imaging modality depends critically on the child's age, the suspected pathology, and the specific clinical question. A systematic approach to imaging ensures timely and accurate diagnosis, which is fundamental to successful management.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the hip joint is paramount for any surgeon managing DDH.
Surgical Anatomy:
- Acetabulum: The socket of the hip joint. In DDH, it is typically shallow, anteverted, and/or superolaterally deficient. The labrum (fibrocartilaginous rim) deepens the socket; in DDH, it can be hypertrophied, everted, or inverted, acting as an impediment to reduction. The triradiate cartilage (epiphyseal plate where ilium, ischium, and pubis meet) is the growth center of the acetabulum and closes around 14-16 years of age; its status dictates the choice of pelvic osteotomy.
- Femoral Head and Neck: The femoral head is usually normal in early DDH but can become flattened or dysmorphic (e.g., coxa magna) with chronic dislocation. The femoral neck often exhibits excessive anteversion, which contributes to instability and gait abnormalities. The ossific nucleus appears around 4-6 months; its integrity is crucial for growth.
- Joint Capsule: Thickened and elongated in dislocated hips, often constricted at the waist (hourglass constriction) by the iliopsoas tendon. Redundant capsule can impede reduction.
- Ligamentum Teres: Often hypertrophied and elongated in DDH, acting as an impediment to reduction in older children.
- Iliopsoas Tendon: Can create an indentation in the anterior capsule, tightening across the joint and contributing to the hourglass constriction, preventing full reduction. It often requires tenotomy during open reduction.
-
Muscles:
- Abductors (Gluteus Medius, Minimus): Responsible for hip stability during gait. Their effective lever arm is compromised in dislocation, leading to Trendelenburg gait.
- Adductors (Adductor Longus, Brevis, Magnus, Gracilis, Pectineus): Often contracted in DDH, resisting reduction. Adductor tenotomy is a common adjunct to reduction.
- Flexors (Iliopsoas, Rectus Femoris): Iliopsoas plays a critical role in anterior stability and can be a significant deforming force.
- Nerves: Femoral nerve (anterior), obturator nerve (medial), sciatic nerve (posterior), superior gluteal nerve (lateral). Awareness of their course is critical to avoid iatrogenic injury during surgical approaches.
- Vessels: Femoral artery and vein (anterior), obturator artery and vein (medial). The medial femoral circumflex artery is the primary blood supply to the femoral head, particularly vulnerable during aggressive reduction maneuvers or extensive capsulotomy, leading to AVN.
Biomechanics:
- Hip Stability: Achieved through a combination of bony congruity (deep acetabulum, spherical femoral head), capsuloligamentous integrity (capsule, ligamentum teres, iliofemoral ligament), and muscle function (particularly abductors and deep external rotators).
-
DDH Pathomechanics:
- Acetabular Dysplasia: A shallow, vertically oriented acetabulum provides insufficient containment of the femoral head, leading to increased joint contact pressures on a smaller area, predisposition to subluxation, and premature cartilage wear.
- Femoral Anteversion: Excessive femoral anteversion (normal 10-15 degrees) causes the femoral head to be inherently unstable in extension and external rotation, often leading to a "pigeon-toed" gait as the child internally rotates to achieve stability.
- Capsular Laxity: Initial laxity allows for subluxation/dislocation. Over time, the capsule thickens and constricts.
- Muscle Imbalance: Contracture of adductors and iliopsoas, coupled with relative weakness of abductors, contributes to dislocation and restricts reduction.
- Joint Reaction Forces: In a dysplastic hip, the contact area is reduced, concentrating forces and leading to cartilage degradation over time. Surgical goals aim to normalize these forces by improving coverage and congruity.
Indications & Contraindications
The management of DDH is age-dependent and follows a progression from non-operative to increasingly complex operative interventions. The primary goal is to achieve and maintain concentric reduction of the femoral head within a well-formed acetabulum, minimizing morbidity, particularly avascular necrosis (AVN).
Non-Operative Indications:
*
Newborns (0-6 months):
* Unstable but reducible hips (Barlow positive, Ortolani positive/equivocal).
* Dysplastic but stable hips detected by ultrasound (e.g., Graf Type IIa hips).
* Initially treated with Pavlik harness or other abduction orthoses.
*
Failed Pavlik Harness/Orthosis:
*
Failure to reduce:
Persistent dislocation or inability to achieve concentric reduction after 3-4 weeks.
*
Failure to stabilize:
Persistent instability despite reduction.
*
Acetabular dysplasia:
Inadequate improvement in acetabular index on radiographs after 6-12 weeks of treatment.
Operative Indications:
*
Older infants (6 months to 18 months):
* Irreducible dislocation.
* Failed closed reduction.
* Persistent dysplasia after successful closed reduction.
*
Children (18 months to 8-10 years):
* Irreducible dislocation requiring open reduction.
* Persistent acetabular dysplasia and/or femoral deformity after open reduction or in previously undiagnosed cases.
* Symptomatic subluxation or pain due to dysplasia.
*
Adolescents/Young Adults (typically >8-10 years):
* Symptomatic acetabular dysplasia (pain, instability, impending osteoarthritis).
* Often managed with periacetabular osteotomy (PAO) for preservation of the native hip joint.
* Femoral deformities (e.g., excessive anteversion, valgus).
Contraindications:
*
Non-Operative:
* Irreducible dislocation in neonates.
* Failure of reduction or stabilization after a reasonable trial (e.g., 3-4 weeks for Pavlik).
* Frank dislocation in older infants (>6 months).
* Significant stiffness preventing proper harness application.
*
Operative:
*
Relative Contraindications:
* Severe systemic comorbidities that preclude general anesthesia.
* Active infection.
* Previous severe AVN with significant femoral head deformity.
* Very young age for certain osteotomies (e.g., PAO not performed if triradiate cartilage is open).
* Lack of adequate bone stock or joint space (for PAO, presence of osteoarthritis is a contraindication to joint preservation).
*
Absolute Contraindications:
* Skeletally mature patients with advanced degenerative joint disease (osteoarthritis) where joint preservation is no longer feasible; total hip arthroplasty (THA) is typically indicated.
Summary of Operative vs. Non-Operative Indications:
| Category | Non-Operative Treatment | Operative Treatment |
|---|---|---|
| Age Group | < 6 months: Primarily. | 6 months - 18 months: Closed reduction + spica cast (with adjuncts). |
| > 18 months: Open reduction + spica cast (with or without osteotomies). | ||
| Older children/Adolescents: Pelvic and/or femoral osteotomies. | ||
| Hip Status | Unstable but Reducible: Barlow positive, Ortolani positive/equivocal. | Irreducible Dislocation: On clinical exam or imaging. |
| Dysplastic but Stable: Graf Type IIa on ultrasound. | Failed Closed Reduction: Persistent subluxation/dislocation after attempts. | |
| Persistent Acetabular Dysplasia: After successful reduction, requiring bony correction. | ||
| Chronic Dislocation: Undiagnosed or late-presenting cases. | ||
| Treatment Response | Initial management for most cases. | Failure of non-operative treatment (e.g., Pavlik harness). |
| Imaging Findings | Mild dysplasia or unstable but reducible on ultrasound. | Significant dysplasia, subluxation, or dislocation on ultrasound/radiographs/CT/MRI. |
| Anatomical impediments to reduction identified on MRI. | ||
| Symptomatology | Asymptomatic infants. | Symptomatic dysplasia/subluxation/dislocation in older children/adolescents (pain, limp). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes and minimizing complications in DDH surgery.
Pre-Operative Planning:
1.
Comprehensive Imaging Review:
*
Plain Radiographs:
Review all available AP pelvic radiographs, false profile views, and hip-at-risk films. Measure acetabular index, LCEA, ACEA, identify Shenton's line, and assess sourcil morphology. Look for secondary signs of dysplasia (e.g., sclerosis of the acetabular roof). Assess femoral head ossification and symmetry.
*
CT/MRI:
When available, meticulously review 3D reconstructions (CT) for bony morphology, femoral anteversion, and acetabular version. MRI provides detailed information on soft tissue impediments (labrum, pulvinar, capsule, psoas), crucial for planning open reduction. Evaluate for signs of early AVN or chondral damage.
*
Templating:
For osteotomies, template on plain radiographs using appropriate scale images. Determine the required amount of acetabular redirection/coverage and the correction needed for femoral version/neck-shaft angle.
2.
Procedure Selection:
Based on age, degree of dysplasia/dislocation, reducibility, and presence of impediments, decide on the primary procedure (closed reduction, open reduction, pelvic osteotomy, femoral osteotomy, or a combination).
3.
Anesthesia Consultation:
Discuss potential challenges, including prolonged operative time, blood loss, and post-operative pain management, especially in younger patients.
4.
Blood Management:
Type and cross-match for potential blood transfusions, particularly for bilateral or extensive osteotomies.
5.
Instrument and Implant Preparation:
Ensure all necessary instruments (osteotomes, retractors, saws, drills, K-wires, screws, plates) and implants (spica cast materials) are available and sterilized.
6.
Team Briefing:
Review the surgical plan with the entire operating room team, including anticipated challenges and critical steps.
Patient Positioning:
Patient positioning varies significantly depending on the planned surgical approach and procedure.
-
Closed Reduction:
- Positioning: Supine on a radiolucent table.
- Preparation: Both lower extremities and pelvis prepped and draped freely to allow full manipulation.
- Considerations: Image intensifier access is critical. Adductor tenotomy may be performed through a small medial incision. After reduction, a spica cast is applied.
-
Open Reduction (Anterior Approach - Smith-Peterson/Ludloff):
- Positioning: Supine on a radiolucent table, usually with a bolster under the ipsilateral gluteal region to rotate the pelvis slightly and expose the anterior hip. The hip is often positioned near the break in the table to allow for flexion/extension during the case.
- Preparation: Entire lower extremity and pelvis prepped and draped, allowing for knee flexion and hip rotation.
- Incision: Usually a bikini incision (Pfirrmann approach) for improved cosmesis, or a longitudinal Smith-Peterson incision.
-
Pelvic Osteotomies (Salter, Dega, Pemberton, Steel, Ganz PAO):
- Positioning: Supine on a radiolucent table. For Salter, Dega, Pemberton, and Steel osteotomies, a bolster is often placed under the ipsilateral gluteal region to facilitate pelvic tilt. For Ganz PAO, specific positioning with pelvic support is crucial to allow complex cuts and fixation.
- Preparation: Entire ipsilateral lower extremity, hip, and flank prepped and draped to allow for wide exposure and manipulation.
- Incision: Varies with osteotomy type. For innominate osteotomies, typically an extended bikini incision or ilioinguinal approach. For PAO, a modified Smith-Peterson or true ilioinguinal approach (for more experienced surgeons).
-
Femoral Osteotomies:
- Positioning: Supine with the operative leg draped free. A small bump under the ipsilateral gluteal region may aid exposure for a proximal femoral osteotomy. Lateral decubitus position is also an option for more proximal approaches.
- Preparation: Entire ipsilateral lower extremity prepped and draped from the iliac crest to the foot.
- Incision: Lateral approach to the proximal femur (often using a bikini incision extension or separate incision).
For all procedures, careful padding of bony prominences and appropriate pressure distribution are essential to prevent nerve palsy and skin breakdown. The surgical team must ensure adequate access for the image intensifier to confirm reduction and fixation throughout the procedure.
Detailed Surgical Approach / Technique
Surgical intervention for DDH encompasses a range of procedures, from closed reduction with adductor tenotomy to complex osteotomies.
1. Closed Reduction
- Indications: Typically for infants 6-18 months with reducible dislocation where non-operative measures have failed. Contraindicated in older children (>18 months) due to high risk of AVN and irreducible soft tissue pathology.
-
Technique:
- Adductor Tenotomy: Performed first in almost all cases to release adductor contracture and facilitate reduction. A small incision is made over the adductor longus tendon, which is released. Often, the adductor brevis and gracilis are also partially released.
- Reduction Maneuver: With the patient deeply relaxed under anesthesia, the hip is gently flexed to 90 degrees, abducted, and externally rotated. Traction may be applied initially. Gentle pressure is applied to the greater trochanter while internally rotating and extending the hip to guide the femoral head into the acetabulum. A palpable "clunk" often signifies reduction.
- Stability Assessment: Once reduced, stability is assessed by taking the hip through its full range of motion. The "safe zone" is the range of abduction where the hip remains stable. Avoid excessive force or extremes of motion to prevent AVN.
- Image Intensifier Confirmation: AP and lateral fluoroscopic views confirm concentric reduction. Hilgenreiner's, Perkin's, and Shenton's lines are assessed.
- Spica Cast Application: If concentric and stable reduction is achieved, a hip spica cast is applied to maintain the reduced position. The cast typically includes the torso and one or both legs, holding the hip(s) in a position of maximal stability (usually 90-100 degrees flexion, 45-55 degrees abduction, neutral rotation). Avoid excessive flexion or abduction, which can increase pressure on the femoral head and risk AVN. The cast is typically changed at 6-week intervals for a total of 3-4 months.
2. Open Reduction (for Irreducible Dislocations)
- Indications: Failed closed reduction, irreducible dislocation in children >18 months, or older infants with significant soft tissue impediments.
-
Common Approaches:
-
Anterior Approach (Smith-Peterson/Ludloff modification):
Most common for open reduction of DDH in children.
- Incision: A bikini incision or a straight incision along the anterior iliac crest extending distally.
- Internervous Plane: Between the sartorius (femoral nerve) and tensor fascia lata (superior gluteal nerve) for the Smith-Peterson approach. More medially, the Ludloff approach utilizes the plane between the pectineus (femoral/obturator nerves) and adductor longus (obturator nerve).
- Dissection: Retract sartorius and rectus femoris medially, and tensor fascia lata laterally. Ligate ascending circumflex vessels. Expose the anterior hip capsule.
- Iliopsoas Tenotomy: The iliopsoas tendon often indents the capsule and must be released to allow full reduction. This is typically done extra-capsularly.
- Capsulotomy: An inverted T-shaped or H-shaped capsulotomy is performed.
-
Removal of Impediments:
- Inverted Labrum: Carefully evert and reposition the labrum using small hooks or elevators.
- Hypertrophied Ligamentum Teres: Excision is usually necessary.
- Hypertrophied Pulvinar: Debridement of excess fibrofatty tissue from the acetabular fossa.
- Constricted Capsule: Release any tight bands within the capsule.
- Reduction: Gentle traction, flexion, abduction, and external rotation maneuvers are used to seat the femoral head concentrically within the acetabulum.
- Capsulorrhaphy: The capsule is imbricated and repaired to tighten the joint and enhance stability, often taking a reefing stitch to pull redundant capsule.
- Spica Cast: Applied as per closed reduction.
-
Medial Approach (Ludloff):
Used for very young infants (typically <6-12 months) with irreducible dislocation. Less invasive.
- Incision: Longitudinal incision between the adductor longus and gracilis muscles.
- Internervous Plane: Between the adductor longus (obturator nerve) and pectineus (femoral nerve).
- Dissection: Retract muscles. Identify and ligate small vessels. Dissect to the joint capsule, releasing the iliopsoas tendon.
- Capsulotomy and Impediment Removal: Similar to the anterior approach, but limited visualization.
- Reduction and Closure: Reduce the hip and close. Spica cast application.
-
Anterior Approach (Smith-Peterson/Ludloff modification):
Most common for open reduction of DDH in children.
3. Pelvic Osteotomies (for Acetabular Dysplasia)
Performed to improve acetabular coverage of the femoral head.
-
Salter Innominate Osteotomy:
- Indications: Unilateral or bilateral acetabular dysplasia in children 18 months to 8 years, with a mobile triradiate cartilage, good femoral head congruity, and reducibility.
-
Technique:
- Approach: Anterior approach, exposing the outer table of the ilium.
- Osteotomy: A transverse osteotomy of the ilium is performed between the anterior superior iliac spine (ASIS) and the greater sciatic notch, just proximal to the acetabulum. The inner table is protected.
- Rotation: The distal fragment (containing the acetabulum) is rotated laterally, anteriorly, and distally to improve coverage.
- Grafting: A tricortical iliac crest bone graft (wedge) is inserted into the osteotomy site anteriorly to maintain the new position.
- Fixation: Two or three K-wires are typically used to stabilize the graft and osteotomy.
- Spica Cast: Applied post-operatively.
-
Dega Osteotomy:
- Indications: Unilateral acetabular dysplasia, often combined with open reduction, for children up to 8-10 years. Creates lateral and posterior coverage.
-
Technique:
- Approach: Anterior approach similar to Salter.
- Osteotomy: An osteotomy is performed through the outer table of the ilium, extending from the ASIS towards the sciatic notch, but stopping short of the inner table and triradiate cartilage. The outer table is then hinged inwards.
- Rotation: The lateral portion of the ilium is hinged down and in, providing inferolateral coverage.
- Grafting: A bone graft (e.g., tricortical iliac crest) is placed in the created gap to maintain the corrected position.
- Fixation: K-wires or screws.
- Spica Cast: Applied post-operatively.
-
Pemberton Pericapsular Osteotomy:
- Indications: Children 18 months to 10 years with significant acetabular dysplasia, usually with a good-quality femoral head. It hinges the acetabulum inferiorly through the triradiate cartilage.
-
Technique:
- Approach: Anterior approach, exposing the ilium and anterior capsule.
- Osteotomy: An osteotomy is made through the full thickness of the ilium, superior and parallel to the capsule, extending from the ASIS posteriorly to just above the posterior inferior iliac spine (PIIS). It passes through the triradiate cartilage.
- Hinging: The distal acetabular fragment is hinged inferiorly through the open triradiate cartilage, improving anterior, lateral, and posterior coverage.
- Grafting: A large wedge graft is placed into the osteotomy gap superiorly.
- Fixation: K-wires.
- Spica Cast: Applied post-operatively.
-
Triple Innominate Osteotomy (Steel, Ganz-Bernese):
- Indications: Older children (typically >8 years) and adolescents with a closed or closing triradiate cartilage, significant dysplasia, and minimal degenerative changes.
- Technique: Involves osteotomies of the ilium, ischium, and pubis to allow full mobilization and redirection of the acetabular fragment. More complex than single osteotomies. The Ganz periacetabular osteotomy (PAO) is a modification with specific cuts around the acetabulum, providing powerful correction without violating the weight-bearing integrity of the posterior column.
- Fixation: Typically with screws.
- Post-operative: Often non-weight-bearing for 6-8 weeks, followed by protected weight-bearing. No spica cast needed for Ganz PAO.
4. Femoral Osteotomies
- Indications: Excessive femoral anteversion, coxa valga, or leg length discrepancy contributing to instability or gait abnormalities. Often combined with open reduction or pelvic osteotomy.
-
Technique (Varus Derotational Osteotomy - VDRO):
- Approach: Lateral approach to the proximal femur, exposing the subtrochanteric or intertrochanteric region.
- Osteotomy: A transverse or oblique osteotomy is performed.
-
Correction:
- Derotation: The distal fragment is internally rotated to correct excessive anteversion. The degree of rotation is usually determined pre-operatively and confirmed intraoperatively by assessing the patellar alignment relative to the femoral condyles with the hip in neutral rotation.
- Varus: The osteotomy can be performed with a wedge resection to create a varus angle, decreasing the neck-shaft angle in cases of coxa valga. This improves mechanical advantage of abductors and increases femoral head containment.
- Shortening: A segment of bone may be resected to achieve limb length equalization in cases of significant discrepancy, or to reduce tension on soft tissues during reduction.
- Fixation: The osteotomy is stabilized with a blade plate, dynamic hip screw, or intramedullary nail.
- Spica Cast: May be used in younger children, often with an internal fixation device.
General Principles for All DDH Surgeries:
*
Gentle Tissue Handling:
Minimize soft tissue trauma, especially around the hip joint, to preserve blood supply to the femoral head and reduce the risk of AVN.
*
Concentric Reduction:
Always confirm concentric reduction under fluoroscopy. Non-concentric reduction leads to failure.
*
Stability:
Ensure adequate stability of the reduction and osteotomy fixation.
*
Avoid Over-correction/Over-abduction:
Can increase pressure on the femoral head, leading to AVN.
Complications & Management
Despite meticulous surgical technique, complications can occur after DDH surgery. Careful pre-operative planning, intra-operative vigilance, and appropriate post-operative care can mitigate these risks.
Common Complications and Management Strategies:
| Complication | Incidence | Management / Salvage Strategies |
|---|---|---|
| Avascular Necrosis (AVN) of Femoral Head | Highly variable (5-30%), depending on age, severity, procedure, and technique. Highest risk in older children undergoing open reduction or closed reduction with excessive force/positioning. |
Prevention:
Meticulous surgical technique, avoiding excessive force during reduction, limiting extreme abduction/flexion in casts, preserving vascular supply (medial femoral circumflex artery).
Management: Once diagnosed (radiographic signs: fragmentation, increased density, collapse), management is largely supportive. Salvage: Mild: Observation, activity modification, bracing. Moderate/Severe with deformity: Femoral osteotomy (varus/derotation), hip resurfacing, or eventually total hip arthroplasty (THA) if severe degenerative changes develop in adulthood. Distraction arthroplasty in some centers. |
| Redislocation/Subluxation | 5-15% after closed reduction, 2-10% after open reduction. |
Prevention:
Accurate reduction, stable fixation of osteotomies, appropriate cast application/positioning, adequate capsulorrhaphy.
Management: Early: Attempt repeat closed reduction (if appropriate), re-do open reduction, or revise osteotomy. Late: Evaluate for underlying residual dysplasia (acetabular or femoral), soft tissue impediments. May require revision open reduction with osteotomy. |
| Nerve Injury (Femoral, Sciatic, Obturator) | Rare (<1-2%). Often transient. Femoral nerve palsy from spica cast compression is more common. |
Prevention:
Careful surgical dissection, identification and protection of nerves, avoiding prolonged or excessive traction, correct cast padding and molding.
Management: Immediate: Release cast if nerve palsy is suspected. Conservative: Observation, physiotherapy. Most neurapraxias resolve spontaneously. Surgical: * Nerve exploration and repair for severe or persistent deficits (rare). |
| Infection (Superficial/Deep) | 1-5%. |
Prevention:
Strict aseptic technique, prophylactic antibiotics, careful wound closure.
Management: Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, irrigation, intravenous antibiotics, hardware removal if necessary (after osteotomy union). |
| Leg Length Discrepancy (LLD) | Variable, depending on initial pathology and growth disturbance (e.g., from AVN). |
Prevention:
Careful planning for femoral shortening osteotomies, minimizing AVN.
Management: Mild (<2cm): Shoe lift. Moderate/Severe: Epiphysiodesis of the longer limb (for younger patients), lengthening of the shorter limb (for older patients, significant LLD), or eventually THA with appropriate component selection. |
| Growth Disturbance | Secondary to AVN affecting growth plates, or iatrogenic damage to triradiate cartilage/femoral physis. |
Prevention:
Minimize AVN, protect physes during osteotomies and K-wire placement.
Management: Depends on the specific growth plate affected and severity. May lead to LLD or angular deformities requiring corrective osteotomies (e.g., contralateral epiphysiodesis, femoral osteotomy). |
| Hardware-Related Complications (Migration, Loosening, Breakage) | 5-10% for plates/screws, higher for K-wires. |
Prevention:
Appropriate size and type of hardware, stable fixation.
Management: Minor asymptomatic: Observation. Symptomatic or unstable: Hardware removal, revision osteotomy and re-fixation, or repeat reduction. |
| Stiffness / Reduced Range of Motion | Variable, common after open reduction or prolonged immobilization. |
Prevention:
Early mobilization (post-cast), careful surgical technique, avoiding excessive scarring.
Management: Physical therapy, gentle stretching. Occasionally, arthrolysis or surgical release of contractures may be required (rare). |
| Heterotopic Ossification (HO) | Rare in pediatric DDH surgery, more common in older patients undergoing hip reconstruction. |
Prevention:
Careful soft tissue handling, post-operative NSAIDs or radiation (rarely used in children).
Management: Observation if asymptomatic. Excision for symptomatic or functionally limiting HO (after maturation). |
| Residual Acetabular Dysplasia | Can occur even after successful reduction and initial surgery. |
Prevention:
Optimal initial reduction, adequate correction with pelvic osteotomies.
Management: Regular follow-up with radiographs. Re-do or additional pelvic osteotomy (e.g., Salter to Dega, or Ganz PAO if triradiate cartilage has closed) in skeletally immature patients. For mature patients, symptomatic residual dysplasia may lead to THA. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful DDH management, designed to protect the surgical repair, promote healing, and restore function. Protocols vary significantly based on the patient's age and the specific procedure performed.
1. After Closed Reduction (with/without Adductor Tenotomy) and Spica Cast:
*
Immobilization:
Hip spica cast maintained for 6-12 weeks, typically changed every 4-6 weeks under anesthesia for infants to reassess reduction and skin integrity. The cast position (flexion, abduction, rotation) is critical to maintain reduction without compromising blood supply to the femoral head.
*
Initial Phase (0-6 weeks):
*
Patient/Parent Education:
Crucial for cast care, skin checks, diapering, feeding, and transport.
*
Activity:
Non-weight-bearing (NWB) on the affected limb. Encourage age-appropriate upper body and core activities.
*
Intermediate Phase (6-12 weeks, after cast removal):
*
Mobilization:
Gentle, passive range of motion (ROM) exercises of the hip, avoiding extremes of motion initially. Progress to active-assisted ROM.
*
Strengthening:
Gentle isometric contractions of gluteal muscles and core.
*
Weight-Bearing:
Initiate protected weight-bearing (e.g., walker, crutches) progressing to full weight-bearing as tolerated and stability allows.
*
Bracing:
Many protocols transition to a removable abduction brace (e.g., Frejka pillow, Pavlik-like brace without harness straps) for several months, particularly at night, to maintain hip position during sleep.
*
Advanced Phase (3-6 months post-cast):
*
Full ROM and Strength:
Progress strengthening exercises, focusing on hip abductors, extensors, and core stability.
*
Gait Training:
Address any compensatory gait patterns.
*
Return to Activity:
Gradual return to age-appropriate activities and sports. Avoid high-impact activities for 6-12 months.
2. After Open Reduction (with/without Pelvic/Femoral Osteotomies) and Spica Cast:
*
Immobilization:
Hip spica cast for 6-12 weeks (sometimes longer for complex osteotomies or very young patients). Cast care as above.
*
Initial Phase (0-6/12 weeks):
*
NWB:
Strict NWB on the operative limb.
*
Cast Care:
As above. Monitor for wound complications.
*
Adjacent Joint Exercises:
Encourage active ROM of knee, ankle, and foot of the casted limb (if not included), and full activity of the contralateral limb.
*
Intermediate Phase (after cast removal, duration varies based on osteotomy healing):
*
Radiographic Assessment:
Confirm osteotomy healing prior to initiating full weight-bearing.
*
Mobilization:
Gradual, passive, and active-assisted ROM of the hip. Protect the surgical site.
*
Strengthening:
Gentle isometric exercises, progressing to isotonic strengthening of hip musculature (abductors, extensors, flexors, rotators) and core.
*
Weight-Bearing:
Initiate protected weight-bearing with crutches/walker, gradually advancing to full weight-bearing over several weeks/months.
*
Bracing:
May use a removable abduction brace, especially for young children or persistent mild dysplasia.
*
Advanced Phase (3-12 months post-cast):
*
Full ROM and Strength:
Progressive strengthening, proprioceptive training, balance exercises.
*
Gait Training:
Address any gait deviations.
*
Return to Activity:
Gradual return to sports and high-impact activities typically after 6-12 months, depending on osteotomy healing and clinical stability.
3. After Periacetabular Osteotomy (PAO) – for Adolescents/Young Adults:
*
Immobilization:
No spica cast. Often a soft brace or abduction pillow for comfort initially.
*
Initial Phase (0-6/8 weeks):
*
Weight-Bearing:
Strict NWB on the operative limb for 6-8 weeks to allow for initial osteotomy healing.
*
CPM/Passive ROM:
Continuous Passive Motion (CPM) device or gentle passive ROM exercises may be initiated within a few days, maintaining precautions (e.g., avoiding extreme flexion/internal rotation to protect the anterior capsule and osteotomy site).
*
Strengthening:
Gentle isometric exercises (gluteal sets, quad sets).
*
Intermediate Phase (6/8-12 weeks):
*
Radiographic Assessment:
Confirm early signs of osteotomy healing.
*
Weight-Bearing:
Progressive weight-bearing, initially partial weight-bearing with crutches, advancing to full weight-bearing over several weeks.
*
ROM and Strengthening:
Active-assisted and active ROM exercises, progressive strengthening of hip and core musculature. Focus on regaining flexibility without overstressing the osteotomy.
*
Advanced Phase (3-6 months+):
*
Full Weight-Bearing:
Typically achieved by 3-4 months.
*
Functional Training:
Proprioception, balance, gait training, sport-specific exercises.
*
Return to Activity:
Gradual return to low-impact activities at 4-6 months, progressing to higher-impact sports by 9-12 months, contingent on pain, strength, and clinical/radiographic healing.
General Rehabilitation Considerations:
*
Pain Management:
Adequate post-operative pain control is essential to facilitate early mobilization and patient cooperation.
*
Patient Education:
Detailed instructions for families and patients regarding activity restrictions, exercises, and warning signs are critical.
*
Compliance:
Adherence to rehabilitation protocols directly impacts long-term outcomes.
*
Individualization:
Protocols should be tailored to the individual patient's age, bone quality, specific procedure, and progress.
*
Long-Term Follow-up:
Continued radiographic and clinical surveillance is necessary into skeletal maturity to monitor for residual dysplasia, AVN, or early degenerative changes.
Summary of Key Literature / Guidelines
The management of DDH is guided by extensive research and consensus guidelines from major orthopedic societies. The evolution of diagnostic imaging and surgical techniques has significantly improved outcomes.
-
Early Diagnosis and Screening:
- The American Academy of Pediatrics (AAP) and the Pediatric Orthopaedic Society of North America (POSNA) recommend universal clinical screening of newborns for DDH. Selective ultrasound screening is recommended for infants with risk factors (e.g., breech presentation, positive family history, female sex, first-born).
- International Hip Dysplasia Institute (IHDI) provides comprehensive resources and guidelines for diagnosis and treatment, emphasizing early detection.
- Graf's Classification System for hip ultrasound remains the gold standard for standardizing ultrasound interpretation in infants, guiding non-operative treatment decisions.
-
Non-Operative Management (Pavlik Harness):
- The Pavlik harness is the treatment of choice for infants <6 months with reducible DDH. Success rates range from 85-95% when initiated early and used correctly.
- Literature highlights the importance of proper application and parental education to avoid complications like femoral nerve palsy or AVN.
- Failure criteria for Pavlik harness (e.g., persistent dislocation after 3 weeks) are well-defined, indicating a need for alternative treatment.
-
Closed Reduction:
- Optimal age for closed reduction is generally 6-18 months. Beyond 18-24 months, the risk of AVN significantly increases, and the likelihood of successful soft tissue reduction decreases, favoring open reduction.
- Adjunctive adductor tenotomy is routinely performed to aid reduction and decrease forces across the hip.
- The safe zone concept in spica casting (avoiding extremes of abduction and flexion) is critical to minimize AVN risk.
-
Open Reduction:
- Indicated for irreducible dislocations or older children.
- The anterior approach (Smith-Peterson or its modifications) is most commonly employed, allowing direct visualization and removal of impediments (inverted labrum, hypertrophied ligamentum teres, constricted capsule, iliopsoas tendon).
- MRI is increasingly used pre-operatively to identify these impediments and guide surgical planning.
-
Pelvic Osteotomies:
- Salter, Dega, Pemberton osteotomies are well-established procedures for acetabular dysplasia in skeletally immature patients (up to 8-10 years), with long-term studies demonstrating their efficacy in improving acetabular coverage and reducing the risk of osteoarthritis. Choice depends on specific morphological defect (e.g., Pemberton for global deficiency, Dega for posterolateral).
- The Ganz Periacetabular Osteotomy (PAO) is the gold standard for symptomatic acetabular dysplasia in adolescents and young adults with an open or recently closed triradiate cartilage and minimal degenerative changes. Numerous long-term studies have shown excellent pain relief and preservation of the native hip, with low rates of conversion to THA at 20+ years. The concept of joint-preserving surgery for symptomatic dysplasia has been strongly validated.
-
Femoral Osteotomies:
- Varus Derotational Osteotomy (VDRO) is frequently combined with open reduction or pelvic osteotomies to correct excessive femoral anteversion, coxa valga, or significant leg length discrepancy. It improves hip biomechanics and stability.
- The optimal degree of correction for femoral anteversion is debated but generally aims for 10-20 degrees.
-
Complications and Long-Term Outcomes:
- Avascular Necrosis (AVN) remains the most feared complication, with rates varying significantly across studies and procedures. Careful technique and adherence to safe zones are paramount. Severity of AVN directly correlates with long-term risk of degenerative changes.
- Long-term follow-up studies confirm that successful treatment of DDH, particularly with early intervention, significantly reduces the incidence and severity of secondary osteoarthritis. However, even successfully treated hips may show radiographic signs of dysplasia or develop early degenerative changes, necessitating lifelong surveillance.
-
Evidence-Based Practice:
- Multicenter studies and registries (e.g., from IHDI, POSNA) continuously refine treatment algorithms and provide data on outcomes and complication rates for various DDH interventions.
- The shift towards individualized treatment plans based on comprehensive imaging (ultrasound, X-ray, CT, MRI) and clinical assessment is emphasized in modern practice.
