Introduction & Epidemiology
Developmental Dysplasia of the Hip (DDH) represents a spectrum of conditions ranging from mild acetabular dysplasia to irreducible dislocation of the femoral head from the acetabulum. This developmental anomaly affects the normal formation and stability of the hip joint. Its etiology is multifactorial, involving a complex interplay of genetic predisposition, intrauterine positioning, and postnatal environmental factors.
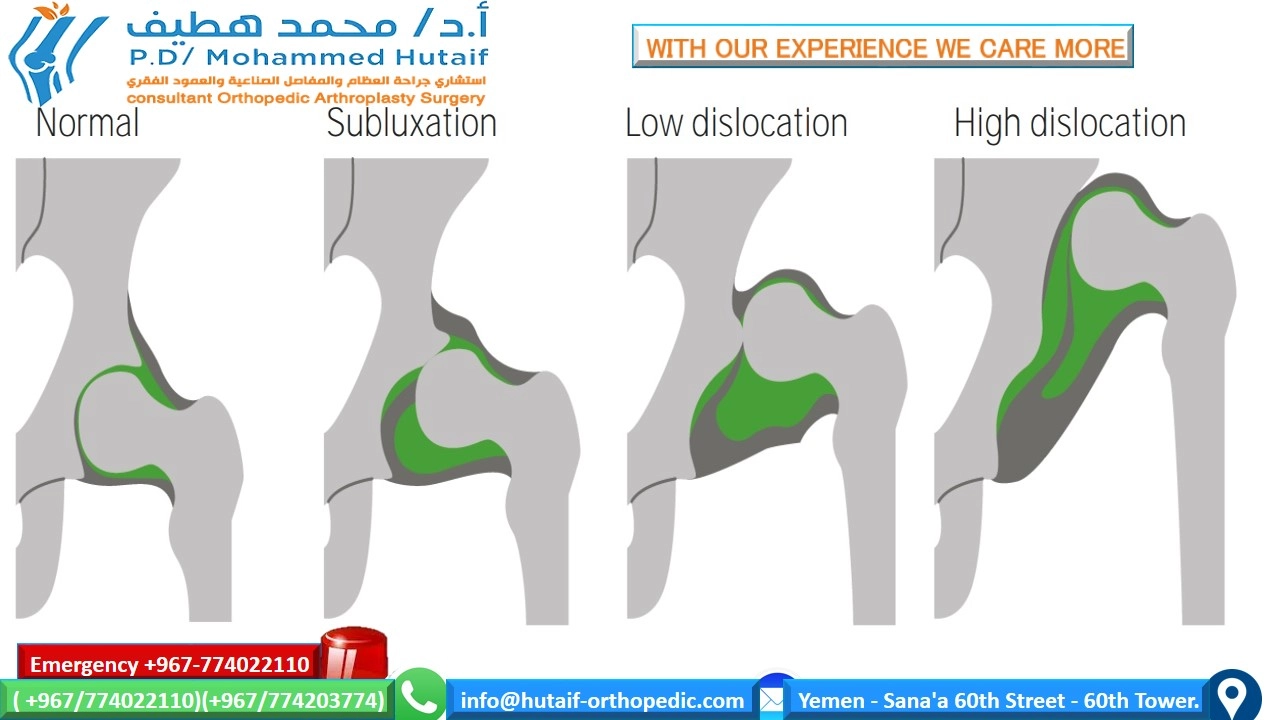
Definition and Spectrum
DDH encompasses:
*
Acetabular Dysplasia:
An abnormally shallow, steeply inclined, or poorly developed acetabulum, leading to inadequate coverage of the femoral head.
*
Subluxation:
Partial displacement of the femoral head from the acetabulum.
*
Dislocation:
Complete loss of contact between the femoral head and acetabulum.
Incidence and Demographics
The reported incidence of DDH varies widely based on screening practices and diagnostic criteria, typically ranging from 1 to 3 per 1,000 live births for frank dislocation, and up to 10-15 per 1,000 for acetabular dysplasia requiring intervention. DDH tends to run in families and can manifest unilaterally or bilaterally, though the left hip is more commonly affected.
Key Risk Factors
Identification of risk factors is paramount for targeted screening and early intervention, which significantly influences outcomes. The principal risk factors include:
*
Female Sex:
Girls are disproportionately affected, with a 4:1 to 9:1 female-to-male ratio, likely due to increased ligamentous laxity influenced by maternal hormones (e.g., relaxin).
*
Firstborn Children:
Primiparity may lead to a relatively constrained intrauterine environment, potentially increasing mechanical forces on the fetal hip.
*
Breech Presentation:
Babies born in the breech position, particularly those with frank breech (feet up by the shoulders), have a significantly elevated risk (up to 10-fold). The American Academy of Pediatrics (AAP) now recommends ultrasound DDH screening for all female breech babies.
*
Family History of DDH:
A positive family history in parents or siblings increases the risk considerably. If one child has DDH, subsequent siblings have an approximate 6% risk; if a parent has DDH, the risk for offspring is 12%; if a parent and a sibling both have DDH, the risk rises to 36%.
*
Oligohydramnios:
Low levels of amniotic fluid can contribute to a more confined intrauterine space, mechanically stressing the fetal hip.
*
Congenital Foot Deformities:
Metatarsus adductus and congenital torticollis are often associated with DDH, suggesting shared mechanisms of intrauterine constraint.
*
Postnatal Positioning:
Traditional swaddling practices that restrict hip abduction and extension have been implicated in promoting hip instability, particularly in cultures where DDH was previously less common.
The understanding of these risk factors underscores the critical need for systematic screening programs, as highlighted by the clinical recommendation: "Risk factors for DDH should be identified in all children" (Evidence Rating: C1). This involves careful clinical examination (Ortolani and Barlow maneuvers in neonates, assessment of limited abduction, leg length discrepancy, and gait abnormalities in older infants and children) and selective imaging protocols.
Surgical Anatomy & Biomechanics
A thorough understanding of the pediatric hip's anatomy and biomechanics is fundamental for effective surgical management of DDH. The key anatomical features include the acetabulum, femoral head, capsule, ligaments, and surrounding musculature, all of which undergo significant developmental changes.
Acetabulum
The acetabulum in DDH is typically shallow, anteverted, and steeply inclined, offering inadequate coverage for the femoral head.
*
Acetabular Index (AI):
A radiographic measure reflecting acetabular inclination, typically >30° in dysplastic hips.
*
Acetabular Depth:
Reduced, leading to decreased contact area and increased stress on cartilage.
*
Acetabular Anteversion:
Often excessive, contributing to anterior instability.
*
Triradiate Cartilage:
The primary growth center of the acetabulum, critical for guiding acetabular development. Its status (open or closed) dictates the choice of pelvic osteotomy.
*
Labrum:
In dysplastic hips, the labrum can be hypertrophied, inverted, or everted, creating a barrier to concentric reduction ("limbus").
*
Pulvinar:
A fibrofatty pad within the acetabular fossa that can hypertrophy and impede reduction.
Femoral Head and Proximal Femur
The femoral head in DDH can be small, flattened, or misshapen (dysplastic).
*
Femoral Head Sphericity:
Loss of sphericity can occur secondary to chronic subluxation or dislocation.
*
Femoral Neck Anteversion:
Often increased in DDH, contributing to an "out-toeing" gait and requiring derotational osteotomy. Normal anteversion decreases with age (approximately 40° at birth, 15° in adulthood).
*
Femoral Neck-Shaft Angle:
Can be increased (coxa valga) in dislocated hips due to lack of normal weight-bearing forces.
*
Greater Trochanter:
Often high-riding due to superior migration of the femoral head, leading to abductor insufficiency.
Joint Capsule and Ligamentous Structures
- Joint Capsule: In DDH, the capsule is often elongated and redundant, particularly inferiorly, allowing superior migration. With chronic dislocation, it can become thickened and constrictive ("hourglass" constriction) at the level of the femoral neck, preventing reduction.
- Ligamentum Teres: Often hypertrophied and elongated, or completely absent in chronically dislocated hips, acting as an impediment to reduction.
- Transverse Acetabular Ligament: Can be hypertrophied and contribute to the obstruction of reduction.
Musculature
- Adductor Muscles (Pectineus, Adductor Longus, Brevis, Magnus, Gracilis): Shortened and contracted in dislocated hips, pulling the femoral head inferomedially. Release is often necessary for reduction.
- Iliopsoas Tendon: Can be tight and anteriorly displaced, impinging on the femoral neck or acetabular rim, acting as an additional barrier to reduction.
- Gluteal Muscles (Gluteus Medius, Minimus): Can be shortened and superiorly displaced, contributing to abductor contracture and weakness post-reduction.
Biomechanics of Dysplasia
A dysplastic hip has altered biomechanics:
*
Reduced Contact Area:
The shallow acetabulum results in decreased surface area for load transmission, increasing stress on the articular cartilage.
*
Abnormal Joint Reaction Forces:
The femoral head is not optimally centered, leading to eccentric loading and abnormal shear forces across the joint.
*
Progressive Instability:
The lack of proper containment allows micro-movements, which can contribute to labral and cartilage damage, perpetuating instability.
*
Early Osteoarthritis:
The long-term consequence of untreated or inadequately treated DDH is premature degenerative arthritis due to chronic abnormal loading and cartilage wear. This is a primary indication for reconstructive surgery to restore normal mechanics.
Indications & Contraindications
The management of DDH is highly dependent on the patient's age, the degree of instability or dislocation, the presence of associated deformities, and the reducibility of the hip. Treatment strategies range from non-operative bracing to complex surgical reconstruction.
Non-Operative Indications
Non-operative management is the mainstay for infantile DDH, particularly for reducibility detected early.
*
Age:
Neonates and infants up to 6 months of age with reducible instability or subluxation are typically managed non-operatively.
*
Reducible Dislocation/Subluxation:
Hips that can be concentrically reduced manually and maintained in a stable position with bracing.
*
Acetabular Dysplasia:
Mild dysplasia without frank instability in young infants.
*
Pavlik Harness:
The preferred initial treatment for infants up to 6 months with reducible DDH. It allows flexion and abduction while limiting extension and adduction, facilitating femoral head molding of the acetabulum.
*
Abduction Bracing:
For infants older than 6 months or those who fail Pavlik harness treatment, rigid abduction orthoses (e.g., Tübingen, Rhino, Frejka pillows) may be used.
Operative Indications
Surgical intervention becomes necessary when non-operative measures fail, for late-presenting DDH, or for hips that are irreducible.
*
Failed Non-Operative Treatment:
Persistent instability or dislocation after an adequate trial of Pavlik harness or other bracing, typically 3-6 weeks.
*
Late-Presenting DDH:
Dislocation detected in older infants (>6-18 months) or children where conservative management is unlikely to succeed due to anatomical barriers.
*
Irreducible Dislocation:
Hips that cannot be concentrically reduced by closed means due to soft tissue interposition (e.g., hypertrophied pulvinar, inverted labrum, tight psoas, constrictive capsule).
*
Residual Dysplasia:
Persistent acetabular dysplasia or inadequate femoral head coverage after successful closed or open reduction, often requiring pelvic osteotomy.
*
Recurrent Dislocation:
Despite previous successful reduction and immobilization.
*
Specific Surgical Procedures:
*
Closed Reduction:
For irreducible hips in children typically between 6-18 months, often preceded by traction.
*
Open Reduction:
For hips irreducible by closed means, often combined with capsulorrhaphy and sometimes femoral or pelvic osteotomies.
*
Pelvic Osteotomies (Salter, Dega, Pemberton, Steel, Periacetabular Osteotomy - PAO):
To improve acetabular coverage and redirection for residual dysplasia in children and adolescents.
*
Femoral Osteotomies (Varus Derotation Osteotomy - VDRO):
To address excessive femoral anteversion, coxa valga, or achieve stability for reduction. Often performed concurrently with open reduction or pelvic osteotomies.
Contraindications
-
Absolute Contraindications:
- Severe Medical Comorbidities: Conditions precluding general anesthesia or significant surgical stress.
- Active Infection: Local or systemic infection must be treated prior to elective surgery.
- Neuromuscular Conditions with Unfavorable Prognosis: In some cases, the goals of reconstruction may be limited, and different strategies (e.g., salvage procedures) may be considered, but primary reconstructive efforts might be contraindicated if the underlying condition makes stability unattainable.
-
Relative Contraindications:
- Advanced Degenerative Joint Disease: In older patients with significant arthritis, reconstructive osteotomies may be less effective, and total hip arthroplasty might be a more appropriate consideration.
- Skeletal Maturity (for certain osteotomies): Procedures relying on the open triradiate cartilage (e.g., Salter, Dega, Pemberton) are contraindicated once the triradiate cartilage has fused. PAO is designed for older adolescents/young adults with fused triradiate cartilage.
- Severe Avascular Necrosis (AVN) of the Femoral Head: While not an absolute contraindication, severe pre-existing AVN may alter the surgical plan and expected outcomes.
Table of Indications: Operative vs. Non-Operative
| Management Strategy | Indications |
|---|---|
| Non-Operative | - Neonates to 6 months with reducible DDH (Barlow/Ortolani positive, subluxation, mild dysplasia) |
| (Pavlik Harness, | - Failed Pavlik harness after adequate trial (for some cases, transitioning to more rigid bracing) |
| Abduction Bracing) | - Surveillance for mild dysplasia (e.g., shallow acetabulum) in absence of instability |
| - Initial management of reducible dislocations/subluxations | |
| Operative | - Failed non-operative treatment (persistent instability/dislocation after adequate trial of bracing) |
| (Closed Reduction) | - Irreducible DDH in infants typically 6-18 months of age (often with preceding traction) |
| (Open Reduction) | - Irreducible DDH in infants/children, especially >12-18 months (when soft tissue blocks are significant) |
| - Persistent subluxation or redislocation after closed reduction | |
| (Pelvic Osteotomies) | - Residual acetabular dysplasia (inadequate femoral head coverage) after successful reduction (open or closed) |
| - Primary acetabular dysplasia in older children/adolescents (Salter, Dega, Pemberton, Steel, PAO depending on age and skeletal maturity) | |
| (Femoral Osteotomies) | - Excessive femoral anteversion or coxa valga contributing to instability or subluxation (often combined with open reduction or pelvic osteotomies) |
| - Leg length discrepancy requiring correction | |
| (Salvage Procedures) | - Failed prior reconstructive surgery, severe AVN, or in cases where primary reconstruction is deemed unlikely to succeed (e.g., severe deformity, older age with significant degenerative changes – may include femoral shortening, arthrodesis, THA) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for successful surgical intervention for DDH, reducing intraoperative complications and optimizing outcomes.
Pre-Operative Assessment and Imaging
- Clinical Examination: Re-assess hip reducibility, range of motion, neurovascular status, and presence of associated deformities. In older children, assess gait and limb length discrepancy.
-
Radiographic Evaluation:
- Anteroposterior (AP) Pelvis Radiograph: Standard view. Assess Hilgenreiner's line, Perkin's line, Shenton's line, acetabular index, lateral coverage (femoral head extrusion index), and ossification of the femoral head and acetabulum.
- Frog-Leg Lateral Radiograph: Assess femoral head sphericity and relationship to the acetabulum in a different plane.
- Ultrasound (for infants < 6 months): Graf classification system. Assesses hip stability dynamically and acetabular morphology. Useful for identifying dynamic instability and monitoring non-operative treatment.
-
Computed Tomography (CT) Scan:
- Pre-operative 3D reconstruction provides precise spatial relationships of the femoral head and acetabulum, critical for planning complex osteotomies (e.g., PAO).
- Post-reduction CT confirms concentricity and determines cast position in closed reductions.
-
Magnetic Resonance Imaging (MRI):
- Provides detailed visualization of soft tissue obstructions (labrum, pulvinar, psoas, capsule), ligamentum teres.
- Evaluates the status of the articular cartilage.
- Assesses for early signs of avascular necrosis (AVN) of the femoral head.
-
Templating for Osteotomies:
- For pelvic osteotomies (e.g., Salter, PAO), use radiographic templates to estimate the desired correction (acetabular coverage, inclination) and the size/type of implants (screws).
- For femoral osteotomies, plan the amount of varus/valgus or derotation required and select appropriate plate and screw sizes.
- Neurovascular Assessment: Document baseline neurological and vascular status, especially important for procedures involving traction or significant dissection.
- Anesthesia Consultation: Evaluate the patient's suitability for general anesthesia, considering age and any comorbidities. Discuss regional anesthesia options for post-operative pain management.
- Informed Consent: Detailed discussion with parents/guardians regarding the nature of the condition, proposed procedure, potential benefits, risks (including AVN, infection, nerve injury, re-dislocation, need for further surgery), and post-operative course.
Patient Positioning and Surgical Preparation
- Operating Table: Utilize a radiolucent table with appropriate attachments for traction if required (e.g., for closed reduction or release of tight structures).
-
Positioning for Open Reduction/Osteotomies:
- Supine Position: Most common for open reductions via anterior approaches (Smith-Petersen, Watson-Jones) and pelvic osteotomies (Salter, Dega, Pemberton, PAO).
- Lateral Decubitus Position: Occasionally used for specific approaches or if bilateral procedures are planned in stages.
- Padding: Ensure adequate padding of all pressure points (heels, sacrum, elbows, head) to prevent nerve palsies or skin breakdown.
- Preparation: The entire affected limb, pelvis, and abdomen are surgically prepped and draped to allow extensive exposure, manipulation of the hip, and fluoroscopic imaging. For bilateral procedures, both hips are prepped.
- Sterile Tourniquet: May be used for femoral osteotomies to minimize blood loss, but less common for open reductions where extensive soft tissue release is required.
- Fluoroscopy Access: Confirm easy access for intraoperative fluoroscopy (C-arm) from the outset, essential for confirming reduction, assessing osteotomy cuts, and implant placement.
- Traction: For closed reductions, or occasionally prior to open reduction in older children, gentle skin or skeletal traction may be applied pre-operatively or intraoperatively to stretch contracted soft tissues and facilitate reduction. Excessive force must be avoided to prevent AVN or nerve injury.
- Urinary Catheterization: May be considered for longer procedures to monitor urine output and keep the bladder decompressed.
Detailed Surgical Approach / Technique
The surgical management of DDH varies significantly based on age, reducibility, and the underlying pathology. This section details common surgical techniques for open reduction and various osteotomies.
1. Open Reduction of the Hip
Indicated for hips irreducible by closed means, typically in children older than 6-12 months. The goal is concentric, stable reduction with removal of anatomical barriers.
A. Anterior Approach (Smith-Petersen / Watson-Jones)
- Patient Position: Supine.
-
Incision:
- Smith-Petersen: Oblique incision along the anterior iliac crest extending distally parallel to the sartorius muscle, or a bikini incision.
- Watson-Jones: Straight incision extending from the anterior superior iliac spine (ASIS) distally and laterally, parallel to the femoral shaft, usually 8-10 cm.
-
Dissection & Internervous Plane:
- Smith-Petersen: Interval between the sartorius (innervated by femoral nerve) and the tensor fascia lata (innervated by superior gluteal nerve) is developed. The rectus femoris is retracted medially or detached from ASIS and anterior inferior iliac spine (AIIS).
- Watson-Jones: Interval between the tensor fascia lata and the gluteus medius (both supplied by superior gluteal nerve). This is a safe internervous plane.
- Exposure: The hip capsule is exposed. The iliopsoas tendon is identified. In a dislocated hip, it often courses anterior to the acetabulum and can be hypertrophied.
-
Soft Tissue Release & Capsule Management:
- Iliopsoas Tenotomy: The iliopsoas tendon is released from its insertion on the lesser trochanter (or elongated) to prevent impingement.
- Capsulotomy: An inverted T-shaped or H-shaped capsulotomy is performed. The anterior limb extends from the acetabular rim distally towards the femoral neck.
-
Identification of Barriers to Reduction:
- Ligamentum Teres: Often hypertrophied and elongated; usually excised.
- Transverse Acetabular Ligament: May be hypertrophied and needs to be incised.
- Pulvinar: Hypertrophied fibrofatty pad within the acetabular fossa; debulked or excised.
- Inverted Labrum (Limbus): The cartilaginous labrum may be inverted into the acetabulum, acting as a significant barrier. It must be released from the acetabular rim or partially excised.
- Inferior Capsular Constriction: The inferior capsule can form an "hourglass" constriction around the femoral neck; it needs to be incised and released.
- Reduction: With careful traction and external rotation, the femoral head is gently guided into the acetabulum. Intraoperative fluoroscopy confirms concentric reduction.
- Capsulorrhaphy: The capsule is then plicated and tightened, typically by excising redundant capsule (especially inferiorly) and repairing the remaining capsule to provide stability. This "vest-over-pants" repair aims to prevent re-dislocation.
- Closure: Layered closure of fascia, subcutaneous tissue, and skin.
- Post-Reduction Immobilization: A hip spica cast is applied to maintain reduction, usually in 20-30° flexion, 30-45° abduction, and neutral rotation. Excessive abduction should be avoided to minimize the risk of AVN. The cast is typically worn for 6-12 weeks, with potential for cast changes.
B. Medial Approach (Ludloff)
- Indication: Primarily for very young infants (<18 months, preferably <6 months) with reducible dislocations, offering direct access to the adductor tendons and psoas.
- Patient Position: Supine, hip abducted and externally rotated.
- Incision: Longitudinal incision in the groin, distal to the pubic tubercle, medial to the adductor longus.
- Dissection: Develops the interval between the adductor longus and gracilis (medially) and the pectineus (laterally). Neurovascular bundle (femoral artery, nerve, vein) is identified and protected laterally.
- Structures Released: Adductor longus, brevis, and gracilis tenotomies. Pectineus is released or retracted. The iliopsoas tendon is identified and released. The anterior branch of the obturator nerve must be protected.
- Capsulotomy/Reduction: The anterior capsule is exposed. Barriers similar to the anterior approach are addressed. Reduction and capsulorrhaphy are performed.
- Advantages: Less muscle dissection, minimal scarring, direct access to release key contractors.
- Disadvantages: Limited exposure in older children, higher risk of nerve injury (obturator, femoral), difficulty with capsular repair.
2. Pelvic Osteotomies (for Acetabular Dysplasia)
These procedures aim to redirect, deepen, or augment the acetabulum to improve femoral head coverage.
A. Salter Innominate Osteotomy
- Indication: Acetabular dysplasia in children aged 1-8 years with an open triradiate cartilage.
- Goal: Redirection of the entire acetabulum to improve anterior and lateral coverage.
- Approach: Smith-Petersen or similar anterior approach to the iliac wing.
-
Technique:
- Subperiosteal exposure of the inner and outer tables of the ilium.
- Osteotomy cut made just above the acetabulum, extending from the greater sciatic notch to the anterior inferior iliac spine.
- A trapezoidal bone graft (typically from the anterior superior iliac spine) is inserted into the osteotomy gap, holding the distal fragment (containing the acetabulum) rotated anterolaterally.
- Fixation with two large Steinmann pins or screws across the osteotomy site into the ischium and pubis.
- Post-op: Spica cast for 6-8 weeks.
B. Dega Osteotomy
- Indication: Acetabular dysplasia, often combined with open reduction, for children up to 10-12 years with an open triradiate cartilage.
- Goal: Lateralization and anteriorization of the lateral acetabular wall, creating a more horizontal roof.
- Approach: Similar to Salter osteotomy.
-
Technique:
- An osteotomy is performed from the anterior superior iliac spine extending posteriorly and inferiorly above the acetabulum, through the outer cortex.
- The inner cortex is left intact and hinged. The osteotomy does not involve the triradiate cartilage directly but rather the supra-acetabular region.
- The lateral fragment is "shelfed" downward and outward to cover the femoral head.
- The gap is filled with a bone graft, creating a deeper, more horizontal acetabular roof.
- Fixation with pins or screws.
- Post-op: Spica cast.
C. Pemberton Pericapsular Osteotomy
- Indication: Acetabular dysplasia in children up to 10-12 years with an open triradiate cartilage.
- Goal: Deepening the acetabulum and improving coverage, particularly posteriorly and superiorly.
- Approach: Anterior approach.
-
Technique:
- An osteotomy is made above the acetabulum, extending posteriorly and inferiorly, entering the triradiate cartilage.
- The distal fragment is hinged through the triradiate cartilage.
- A wedge graft is inserted into the superior gap, depressing the acetabular roof and increasing coverage.
- Fixation with pins or screws.
- Post-op: Spica cast.
D. Periacetabular Osteotomy (PAO) - Ganz Osteotomy
- Indication: Acetabular dysplasia in adolescents and young adults with closed triradiate cartilage, and an intact, spherical femoral head without significant arthritis.
- Goal: Preserve the joint by correcting the orientation of the acetabulum in all three planes while maintaining the integrity of the posterior column.
- Approach: Modified Smith-Petersen or Bernese approach (Sartorius-Tensor interval).
-
Technique (Complex, requires precise execution):
- Exposure: Extensive subperiosteal exposure of the innominate bone, including the anterior column, posterior column, and pubic ramus.
-
Osteotomy Cuts:
- Iliac Osteotomy: Transverse cut above the anterior inferior iliac spine (AIIS) towards the sciatic notch, avoiding damage to the superior gluteal neurovascular bundle.
- Ischial Osteotomy: Cut the ischial ramus just below the acetabulum.
- Pubic Osteotomy: Cut the superior pubic ramus near the pubic symphysis.
- Posterior Column Osteotomy: The most critical and challenging cut. This osteotomy extends from the iliac cut inferiorly, just medial to the hip joint, freeing the acetabular fragment while preserving the posterior column continuity. Careful attention to the obturator nerve and vessels is vital.
- Mobilization and Reorientation: The acetabular fragment is mobilized and reoriented (rotated, translated) to achieve optimal femoral head coverage and reduce impingement. Intraoperative fluoroscopy or navigation is used to confirm optimal positioning.
- Fixation: The repositioned acetabular fragment is secured to the stable posterior column with 3-4 cortical screws.
- Advantages: Preserves the posterior column, allows for correction in multiple planes, preserves acetabular volume.
- Post-op: Early mobilization with protected weight-bearing for 6-12 weeks.
3. Femoral Osteotomies
Performed to address femoral deformities (anteversion, valgus) that contribute to instability or incongruity.
A. Proximal Femoral Varus Derotation Osteotomy (VDRO)
- Indication: Excessive femoral anteversion or coxa valga, often combined with open reduction or pelvic osteotomies to achieve hip stability and improve joint mechanics.
- Approach: Lateral approach to the proximal femur (between vastus lateralis and gluteus medius).
-
Technique:
- Subperiosteal exposure of the proximal femur.
- Osteotomy performed typically below the lesser trochanter.
- The distal fragment is derotated (internally) to correct excessive anteversion and/or brought into varus to decrease the neck-shaft angle (correct coxa valga). The amount of correction is carefully pre-planned.
- Fixation with a pediatric hip plate and screws (e.g., blade plate, dynamic hip screw, or locking plate).
- Post-op: Spica cast or restricted weight-bearing, depending on fixation stability.
Complications & Management
Surgical treatment of DDH, despite its benefits, carries significant risks. Understanding these complications, their incidence, and appropriate management strategies is crucial for all orthopedic surgeons.
Common Complications and Management Strategies
| Complication | Incidence | Pathophysiology / Risk Factors | Salvage Strategies / Management |
|---|---|---|---|
| Avascular Necrosis (AVN) of Femoral Head | 5-20% (variable) | Forceful reduction, extreme positioning (excessive abduction), age >1 year at reduction, multiple attempts, hematoma/capsular compromise of retinacular vessels. |
- Non-operative for mild cases (observation, protected weight-bearing).
- Containment surgery (osteotomies) for moderate/severe cases to reshape head and improve coverage. - Valgus osteotomy to relieve mechanical stress. - Core decompression (controversial). - Total Hip Arthroplasty (THA) for end-stage arthritis. |
| Re-dislocation / Subluxation | 5-15% (variable) | Incomplete reduction, inadequate capsulorrhaphy, poor quality acetabulum, persistent soft tissue barriers, failure of cast immobilization, inadequate post-operative protection. |
- Revision open reduction with more aggressive soft tissue release/capsulorrhaphy.
- Concomitant femoral or pelvic osteotomy to improve stability. - Repeat spica casting. - Addressing underlying biomechanical issues. |
| Nerve Palsy | 1-5% | Traction injury (femoral, sciatic, obturator nerves), direct surgical trauma, hematoma, nerve compression in cast. |
- Immediate cast change or reduction of traction if identified early.
- Observation for spontaneous recovery (most cases resolve). - Nerve exploration and neurolysis for persistent deficits. - Management of foot drop (AFO). |
| Infection (Superficial/Deep) | <1-2% | Surgical site contamination, prolonged surgery, hematoma. |
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical debridement, intravenous antibiotics, removal of hardware if infected. - Close monitoring for septic arthritis. |
| Hardware-Related Complications | 5-10% (variable) | Prominence, migration, breakage, loosening (pins, screws, plates). |
- Symptomatic hardware removal.
- Revision surgery for non-union or loss of correction if hardware failure leads to instability. - Re-fixation with different implants. |
| Growth Disturbance | <1% | Damage to epiphyseal plates (femoral head, greater trochanter, triradiate cartilage), particularly with osteotomies in young children. |
- Leg length discrepancy management (e.g., epiphysiodesis of the longer limb, lengthening of the shorter limb).
- Revision osteotomy if significant deformity develops. |
| Leg Length Discrepancy (LLD) | 5-15% (variable) | Over-correction of femoral shortening, AVN leading to growth arrest, asymmetric growth after osteotomies, chronic subluxation. |
- Shoe lift for mild LLD.
- Epiphysiodesis of the longer limb. - Femoral lengthening of the shorter limb (complex, high complication rate). |
| Stiffness / Limited ROM | 5-10% (variable) | Prolonged immobilization, heterotopic ossification, extensive capsular scarring, inadequate post-operative physical therapy. |
- Aggressive physical therapy, stretching, continuous passive motion (CPM).
- Manipulation under anesthesia. - Surgical release of adhesions or heterotopic ossification (rare). |
| Heterotopic Ossification (HO) | <1-5% | Post-traumatic, often around the operative site; risk increased with extensive muscle dissection, multiple procedures, specific genetic predispositions. |
- Prophylaxis (NSAIDs, radiation) in high-risk patients.
- Observation for asymptomatic HO. - Surgical excision for symptomatic HO (e.g., limiting ROM) after maturation. |
| Residual Dysplasia | Up to 20% | Inadequate initial correction, persistent growth abnormalities, progressive deformity over time. |
- Secondary pelvic osteotomy (e.g., PAO in adolescents, Dega/Salter in younger children).
- Femoral osteotomy if significant femoral deformity. |
| Premature Osteoarthritis | Long-term (high) | Primary underlying dysplasia, AVN, residual incongruity, altered joint mechanics. The ultimate long-term complication if treatment fails. |
- Activity modification, pain management.
- Arthroscopy for labral tears or impingement. - Peri-acetabular osteotomy (if hip still salvageable) to delay progression. - Total Hip Arthroplasty (THA) as a definitive salvage procedure. |
Management Principles
- Early Recognition: Prompt identification of complications facilitates timely intervention and improves prognosis.
- Preventive Measures: Careful surgical technique, avoidance of excessive force during reduction, appropriate cast positioning, strict aseptic technique, and judicious use of prophylactic antibiotics.
- Patient Education: Comprehensive discussion of potential complications with families pre-operatively helps manage expectations and ensures compliance with post-operative instructions.
- Multidisciplinary Approach: Involving physical therapists, pain specialists, and other specialists as needed.
- Long-Term Follow-up: Essential for monitoring for late complications such as residual dysplasia, AVN, growth disturbances, and the development of osteoarthritis.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical phase following surgical correction of DDH, aiming to restore hip function, maintain reduction, prevent stiffness, and facilitate appropriate musculoskeletal development. Protocols vary depending on the specific procedure performed, patient age, and surgeon preference.
1. Immediate Post-Operative Period (Day 0-7)
-
Immobilization:
- Spica Cast: For open reductions and many pelvic osteotomies (Salter, Dega, Pemberton). The cast typically maintains the hip in a safe position (e.g., 20-30° flexion, 30-45° abduction, neutral rotation) to minimize stress on the healing tissues and prevent re-dislocation. Excessive abduction must be avoided to mitigate AVN risk.
- External Fixation/Bracing: For some complex osteotomies or when early controlled motion is desired (e.g., after PAO, some femoral osteotomies where stable internal fixation allows).
-
Pain Management:
- Epidural analgesia, regional nerve blocks, and oral/intravenous opioid and non-opioid analgesics are used to manage post-operative pain.
-
Neurovascular Monitoring:
- Frequent assessment of distal pulses, capillary refill, skin color, temperature, and neurological function (e.g., dorsiflexion/plantarflexion of ankle, sensation) in the affected limb, especially with spica casts, to detect compartment syndrome or nerve impingement.
-
Cast Care (if applicable):
- Instructions for parents/caregivers on cast cleanliness, skin checks around cast edges, and recognizing signs of pressure sores or infection.
-
Positioning:
- Regular repositioning to prevent pressure sores and maintain respiratory function.
2. Early Rehabilitation Phase (Post-Cast Removal / Weeks 6-12)
- Cast Removal: Typically at 6-12 weeks, confirmed by radiographs showing signs of healing or stable reduction.
-
Gradual Mobilization:
- Range of Motion (ROM): Gentle, active-assisted and passive ROM exercises are initiated to restore hip flexion, abduction, and rotation. Avoid forced ROM.
-
Weight-Bearing:
Progression of weight-bearing is dictated by the stability of the surgical repair and osteotomy healing.
- Non-weight-bearing (NWB) or Toe-touch weight-bearing (TTWB): Common for the initial weeks after cast removal, particularly for osteotomies or if AVN risk is high.
- Partial Weight-Bearing (PWB): Gradually advanced with crutches or walker.
- Full Weight-Bearing (FWB): Progressed once bone healing is evident and pain allows.
-
Strengthening:
- Isometric exercises for gluteal muscles (abductors) and quadriceps, progressing to concentric and eccentric strengthening.
- Focus on core stability.
-
Physical Therapy (PT):
- Supervised PT sessions are crucial to guide the child through exercises, monitor progress, and educate families.
3. Intermediate Rehabilitation Phase (Months 3-6 Post-Surgery)
-
Functional Training:
- Gait Training: Focus on restoring a normal gait pattern, addressing any compensatory mechanisms. Use of crutches or canes is weaned off as strength and balance improve.
- Balance and Proprioception: Exercises to improve balance and coordination.
-
Advanced Strengthening:
- Resistance exercises using bands, bodyweight, and light weights.
- Sport-specific drills for older children/adolescents.
-
Activity Progression:
- Gradual return to age-appropriate activities and non-contact sports, avoiding high-impact activities initially.
- Avoidance of positions of extreme hip rotation and abduction for several months, depending on the stability of the hip.
4. Long-Term Follow-Up and Monitoring (Months 6 - Years)
-
Radiographic Monitoring:
- Regular follow-up radiographs (AP pelvis) to assess acetabular development, femoral head sphericity, signs of AVN, and hardware integrity.
- Annual or biennial checks until skeletal maturity for signs of residual dysplasia or AVN progression.
-
Clinical Assessment:
- Monitoring for pain, limping, leg length discrepancy, and hip range of motion.
-
Activity Modification:
- Counseling on appropriate activity levels and potential limitations in contact sports for some patients.
-
Addressing Residual Issues:
- If residual dysplasia or other complications arise, further interventions (e.g., revision osteotomy, epiphysiodesis for LLD) may be necessary.
-
Prevention of Osteoarthritis:
- Education on maintaining a healthy weight and avoiding high-impact activities to delay the onset of degenerative changes.
General Principles:
*
Individualization:
Rehabilitation protocols must be individualized based on the patient's age, surgical procedure, bone healing, and overall progress.
*
Gradual Progression:
Avoid pushing too quickly to prevent re-injury or loss of correction.
*
Parental Involvement:
Active participation and education of parents/caregivers are essential for successful rehabilitation, especially in younger children.
Summary of Key Literature / Guidelines
The management of DDH is guided by extensive research and consensus guidelines from major orthopedic societies. The evolution of diagnostic techniques and surgical approaches has significantly improved outcomes, although challenges remain.
Screening and Diagnosis
The importance of early identification cannot be overstated. Clinical guidelines, such as those from the American Academy of Pediatrics (AAP) and the American Academy of Orthopaedic Surgeons (AAOS), emphasize:
*
Universal Clinical Screening:
All neonates and infants should undergo repeated clinical examinations for hip instability (Ortolani and Barlow maneuvers) until walking.
*
Risk Factor-Based Imaging:
Ultrasound screening is recommended for infants with risk factors such as breech presentation (especially female breech babies), positive family history, or clinical suspicion. Timing is crucial; typically at 4-6 weeks of age to allow for resolution of physiological laxity.
*
Radiography:
Becomes the primary imaging modality after 4-6 months of age, once significant ossification of the femoral head and acetabulum has occurred.
Non-Operative Management
- Pavlik Harness: The gold standard for reducible DDH in infants up to 6 months of age. Success rates range from 80-95%. Prolonged bracing (>3 weeks) without improvement, or an irreducible hip in the harness, are indications for reassessment and potential alternative management.
- Abduction Bracing: For infants 6-12 months or failed Pavlik harness. More rigid braces are often used.
Surgical Management
- Closed Reduction: For irreducible hips typically aged 6-18 months, often preceded by traction. Success rates are high, but risk of AVN is a significant concern. Post-reduction CT is recommended to confirm concentricity and rule out impingement.
- Open Reduction: Indicated for irreducible dislocations or those failing closed reduction. Studies consistently show good long-term outcomes, especially when combined with appropriate pelvic or femoral osteotomies to address underlying deformities. The choice of surgical approach (anterior vs. medial) depends on the surgeon's preference and patient age, with the anterior approach being more versatile for older children and complex cases.
-
Pelvic Osteotomies:
- Salter, Dega, Pemberton: Effective for improving acetabular coverage in younger children with open triradiate cartilages. Outcomes are generally favorable, with good correction of acetabular dysplasia.
- Periacetabular Osteotomy (PAO) (Ganz): Considered the gold standard for symptomatic acetabular dysplasia in adolescents and young adults with a closed triradiate cartilage and a spherical, non-arthritic femoral head. Long-term studies demonstrate good pain relief and preservation of the native hip joint in a high percentage of patients, delaying or preventing total hip arthroplasty.
- Femoral Osteotomies: Commonly performed concurrently with open reduction or pelvic osteotomies to correct excessive femoral anteversion or coxa valga, contributing to joint stability and improved biomechanics.
Complications and Long-Term Outcomes
- Avascular Necrosis (AVN): Remains the most feared complication, with reported incidence varying significantly. Its occurrence correlates with age at reduction, the force of reduction, and extreme positioning. AVN can lead to femoral head deformity, growth arrest, and premature osteoarthritis.
- Residual Dysplasia: Requires ongoing surveillance and may necessitate secondary osteotomies to prevent premature degeneration.
- Osteoarthritis: The ultimate long-term outcome of untreated or inadequately treated DDH is the development of hip osteoarthritis, often requiring total hip arthroplasty in adulthood. The goal of early diagnosis and effective surgical reconstruction is to normalize hip mechanics and delay or prevent this progression.
Current Research and Future Directions
Ongoing research focuses on refining diagnostic methods, optimizing timing and methods of intervention, minimizing complications (especially AVN), and developing advanced imaging techniques to predict outcomes. Genetic studies are also exploring the molecular basis of DDH to identify at-risk individuals more precisely.
The consistent message across the literature reinforces that "Risk factors for DDH should be identified in all children" (Evidence Rating: C1), highlighting the importance of initial screening and comprehensive management strategies for optimal long-term joint health. Early detection and appropriate intervention across the spectrum of DDH are critical for preventing long-term morbidity and preserving native hip joint function.
