Introduction and Biomechanics
The hip joint (acetabulofemoral joint) is a highly congruent, diarthrodial ball-and-socket joint. It is inherently stable due to its deep bony architecture, the augmenting fibrocartilaginous labrum, and a formidable capsuloligamentous envelope comprising the iliofemoral (ligament of Bigelow), pubofemoral, and ischiofemoral ligaments. Because of this profound intrinsic stability, hip dislocations generally require high-energy trauma to occur.
Often, these injuries are not isolated; they are frequently associated with multiple injuries to different organ systems, including closed head injuries, blunt chest trauma, and intra-abdominal visceral injuries. Motor vehicle accidents (MVAs) remain the most common mechanism of hip dislocation, followed by falls from a significant height, industrial crush accidents, and, more rarely, high-impact sports such as American football, rugby, or wrestling.
Clinical Pearl: Always adhere to Advanced Trauma Life Support (ATLS) protocols when evaluating a patient with a hip dislocation. The distracting nature of a deformed, shortened limb must not delay the primary survey. Once life-threatening injuries are stabilized, the dislocated hip takes absolute precedence over other orthopedic injuries due to the time-sensitive risk of osteonecrosis.
Mechanism of Injury and Clinical Presentation
Posterior Dislocations
Posterior dislocations occur much more frequently than anterior dislocations (accounting for approximately 85% to 90% of cases). The classic mechanism is a posteriorly directed force applied to the anterior aspect of a flexed knee with the hip also in a flexed position—commonly referred to as a "dashboard injury."
The exact position of the hip at the moment of impact dictates the resulting injury pattern:
* Pure Dislocation: Occurs when the hip is in a high degree of flexion and adduction.
* Fracture-Dislocation: Lesser degrees of hip flexion and increasing amounts of hip abduction with a similarly applied force often result in an associated posterior wall or column acetabular fracture.
Clinical Presentation: Patients with an isolated posterior hip dislocation classically present with the affected lower extremity in a position of hip flexion, adduction, internal rotation, and shortening.
Anterior Dislocations
Anterior dislocations are caused by a forceful abduction and external rotation applied to the affected limb. The degree of hip flexion at the time of injury determines whether the femoral head dislocates superiorly (pubic) or inferiorly (obturator).
Clinical Presentation: Anterior dislocations cause the leg to be held in a position of abduction and external rotation. Superior (pubic) dislocations present with the hip extended, while inferior (obturator) dislocations present with the hip flexed.
Surgical Warning: Although isolated hip dislocations are easily recognized by their classic resting postures, associated lower extremity injuries (e.g., ipsilateral femoral shaft fractures) may distract the examining physician or alter the classic position of the dislocated limb. Careful physical examination is crucial, with particular attention paid to the sciatic nerve examination and ipsilateral knee ligamentous integrity.
Radiographic Evaluation
Radiographic assessment of patients with a suspected hip dislocation must be prompt and systematic.
- Pre-Reduction Imaging: An anteroposterior (AP) view of the pelvis is mandatory before any reduction attempt to confirm the direction of the dislocation and identify any gross associated fractures of the femoral neck, head, or acetabulum.
- Post-Reduction Imaging: Following reduction, a repeat AP pelvis radiograph is required to confirm concentric reduction. Additionally, 45-degree oblique Judet views (iliac and obturator obliques) of the pelvis are obtained to evaluate the acetabular columns.
- Computed Tomography (CT): A CT scan of the pelvis with 2-mm to 3-mm fine cuts and bone windows is universally recommended after reduction. CT is the gold standard to rule out associated femoral head or acetabular fractures, identify incarcerated intra-articular osteochondral fragments, and definitively assess joint congruency.

Axial CT imaging is critical for assessing joint congruency and identifying subtle osteochondral fragments or associated subluxations that plain radiographs may miss.
Understanding the vectors of subluxation and dislocation is essential. High-energy trauma can cause complex multi-directional instability patterns across various joints, necessitating advanced cross-sectional imaging.
Classification Systems
Hip dislocations are classified according to the position of the femoral head in relation to the acetabulum and the presence of associated fractures.
Thompson and Epstein Classification (Posterior Dislocations)
This system categorizes posterior dislocations based on associated bony injuries:
* Type I: Simple dislocation with or without a minor neurological deficit or minor posterior wall fracture.
* Type II: Dislocation with a large, single fracture of the posterior acetabular rim.
* Type III: Dislocation with a comminuted fracture of the posterior acetabular rim, with or without a major fragment.
* Type IV: Dislocation with fracture of the acetabular rim and floor.
* Type V: Dislocation with an associated fracture of the femoral head.
Epstein Classification (Anterior Dislocations)
Anterior dislocations are subdivided based on the superior/inferior position of the femoral head:
1. Type I: Pubic (Superior)
* IA: With no fracture (simple)
* IB: With fracture of the head of the femur
* IC: With fracture of the acetabulum
2. Type II: Obturator (Inferior)
* IIA: With no fracture (simple)
* IIB: With fracture of the head of the femur
* IIC: With fracture of the acetabulum

Fig. 57-9 Bilateral obturator dislocations of the hip. Note the profound abduction and inferior displacement of the femoral heads.
Historical Note: The term central dislocation historically referred to a medial position of the femoral head following a fracture involving the medial wall of the acetabulum. This subtype is not purely a dislocation but rather a fracture-dislocation and is more accurately classified and managed under the Letournel and Judet classification of acetabular fractures.
Principles of Emergency Management
A hip dislocation constitutes a true orthopedic emergency. Delaying reduction exponentially increases the risk of osteonecrosis (avascular necrosis) of the femoral head due to prolonged kinking, stretching, or compression of the medial circumflex femoral artery and its retinacular branches.
Hougaard and Thomsen established the critical "6-hour rule." They reported an osteonecrosis rate of 4.8% if reduction occurred within 6 hours of injury, compared with a staggering 53% if reduction was delayed for more than 6 hours.
Closed reduction should initially be attempted in the emergency department under deep intravenous sedation or general anesthesia. Complete muscle relaxation is paramount to prevent iatrogenic chondral damage or femoral neck fracture during reduction. If other life-threatening injuries require emergency operative intervention (e.g., exploratory laparotomy), the initial hip reduction can be performed simultaneously in the operating room.
Closed Reduction Techniques
The following guidelines apply primarily to simple hip dislocations without significant associated femoral neck or large acetabular fractures (Thompson and Epstein Type I).
The fundamental principle of all closed reduction methods is to recreate the injurious deforming force to unlock the femoral head, followed by traction and gentle rotation to guide the head back into the acetabulum.
* For Posterior Dislocations: Flexion, adduction, and internal rotation, followed by longitudinal traction.
* For Anterior Dislocations: Longitudinal traction in extension, followed by internal rotation and adduction.
Pitfall: Regardless of the method chosen, only two or three gentle attempts should be made at closed reduction. Multiple, increasingly forcible attempts can lead to iatrogenic femoral head, neck, or shaft fractures, or devastating cartilaginous shearing injuries.
1. The Allis Maneuver
Performed with the patient supine. The surgeon stands over the patient, flexing the patient's hip and knee to 90 degrees. While an assistant stabilizes the pelvis by applying downward pressure on the anterior superior iliac spines (ASIS), the surgeon applies steady, progressively increasing longitudinal traction in line with the femur. Gentle internal and external rotation helps clear the posterior acetabular lip.
2. The Stimson Maneuver
Performed with the patient prone. The affected leg hangs off the side of the stretcher, with the hip and knee flexed to 90 degrees. The surgeon applies downward pressure on the proximal calf, utilizing gravity to assist with longitudinal traction, while an assistant stabilizes the pelvis.
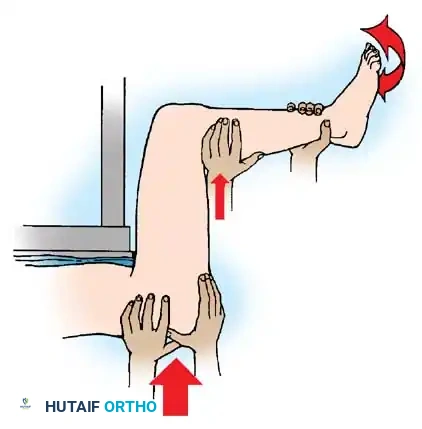
Fig. 57-10 A, Allis maneuver. B, Stimson maneuver. Both rely on 90 degrees of hip flexion and longitudinal traction.
3. The Lefkowitz Maneuver
The surgeon places their own knee beneath the patient's flexed knee to act as a fulcrum. The surgeon's hand levers the ipsilateral ankle downward, translating into upward traction on the femoral head, while simultaneously controlling rotation.

Fig. 57-11 Lefkowitz maneuver using the physician’s knee as a fulcrum for the affected limb. The left hand levers the ipsilateral ankle and controls rotation.
4. The East Baltimore Lift
This technique requires three providers. The patient is supine. The surgeon and an assistant stand on opposite sides of the patient, facing each other. They place their arms under the patient's flexed calf, resting their hands on each other's shoulders to create a human fulcrum. A second assistant stabilizes the pelvis. The surgeon uses their free hand to push downward on the patient's ankle, generating powerful, controlled upward traction on the femur.
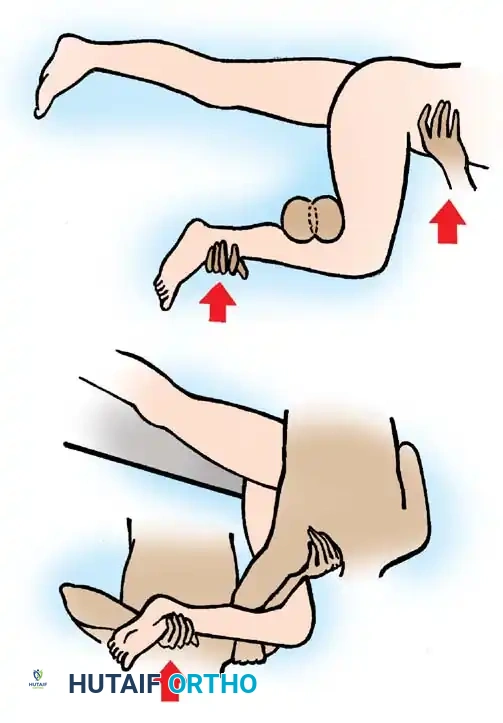
Fig. 57-12 A, East Baltimore lift shown with physician and assistant’s arms as a fulcrum and ankle as a lever. B, A second assistant stabilizes the pelvis.
Indications for Open Reduction
Failed closed reduction of the hip is a strict indication for immediate open reduction. Causes of an irreducible hip include:
* "Buttonholing" of the femoral head through a tight defect in the capsule.
* Inversion of the acetabular labrum into the joint space.
* Interposition of the piriformis muscle, gluteus maximus, or capsule into the acetabulum.
* Incarcerated osteochondral bone fragments from the femoral head or acetabulum.
If closed reduction fails, or if post-reduction CT reveals a non-concentric reduction (widened joint space), skeletal traction via a distal femoral pin should be applied to slightly distract the joint and prevent further cartilaginous abrasion until surgery can be performed.
Surgical Approaches and Technique
The choice of surgical approach is dictated by the direction of the dislocation and the location of any associated pathology (e.g., posterior wall fracture vs. anterior femoral head fracture).
- Posterior Dislocations: Best addressed via the posterior Kocher-Langenbeck approach. This allows direct visualization of the posterior capsule, sciatic nerve, and posterior column.
- Anterior Dislocations: Can be reduced via the direct anterior approach (Smith-Petersen) or the anterolateral/direct lateral approaches (Watson-Jones or Hardinge). The anterolateral approach offers better access to the superior capsule, while the direct anterior approach provides excellent visualization of femoral head fractures.
🔪 Surgical Technique 57-3: Open Reduction of Hip Dislocation
- Positioning and Approach: Position the patient appropriately (lateral decubitus for Kocher-Langenbeck; supine for Smith-Petersen). Perform the standard dissection down to the joint capsule.
- Capsular Assessment: Regardless of the direction of the dislocation, once the deep approach has been made, assess the capsule first. Identify the rent in the capsule caused by the trauma.
- Capsulotomy Extension: If the femoral head is buttonholed, extend the traumatic capsulotomy in a T-shaped fashion along the acetabular rim. Crucial: Carefully preserve the labrum during this extension.
- Joint Inspection: Inspect the joint meticulously for intervening capsule, inverted labrum, incarcerated piriformis muscle, or loose osteochondral bony fragments.
- Distraction: If necessary, retract or distract the hip manually. Alternatively, skeletal traction applied through a fracture table or a femoral distractor (pins in the ilium and distal femur) can provide excellent visualization of the deep acetabulum.
- Debridement and Reduction: Once the joint has been cleared of all debris and interposed tissue, reduce the hip joint by releasing the traction and gently manipulating the leg.
- Repair: Repair the capsule along with the labrum using heavy non-absorbable sutures. A robust capsular repair helps prevent recurrent instability.
- Closure: Close the wound in layers over a suction drain to prevent hematoma formation.
Postoperative Protocol and Rehabilitation
Postoperative management focuses on protecting the joint while preventing stiffness.
* Immobilization: An abduction pillow is highly useful in the immediate postoperative period, especially in sedated, polytraumatized, or noncompliant patients with a previous posterior dislocation, to prevent adduction and internal rotation.
* Weight Bearing: Some authors advocate for a period of protected weight-bearing (toe-touch or partial) for 4 to 6 weeks to theoretically decrease the incidence of femoral head collapse from osteonecrosis, though the definitive biomechanical benefits of this remain debated in the literature.
* Physical Therapy: Gait training is initiated once the patient regains motor control. Patients are strictly advised to avoid putting the hip in the position of the original dislocation. Gentle active and active-assisted range-of-motion exercises, along with hip abductor and flexor strengthening, are initiated early.
Complications
1. Osteonecrosis (Avascular Necrosis)
Osteonecrosis occurs in 4% to 22% of hip dislocations without associated fractures. The time to reduction is the single most critical modifiable risk factor. However, even under optimal circumstances (reduction < 3 hours), approximately 10% of patients may still develop radiographic signs of osteonecrosis due to the initial vascular insult.
Most patients who develop osteonecrosis become symptomatic within 2 years of the injury, though late presentations up to 5 years post-injury have been documented. Routine MRI at 3 to 6 months post-injury is often utilized to detect early avascular changes before subchondral collapse occurs.

Fig. 57-13 A, Posterior dislocation of the hip. B, Osteonecrosis of the femoral head 8 months after closed reduction. Note the profound subchondral sclerosis, narrowed joint space, and early femoral head collapse.
2. Post-Traumatic Osteoarthritis
Osteoarthritis is the most common long-term complication following hip dislocation. While a percentage of this is secondary to late-stage osteonecrosis, a significant number of patients develop primary post-traumatic osteoarthritic changes due to the initial chondral shear injury at the time of impact. Upadhyay and Moulton reported a 26% prevalence of osteoarthritis in patients with simple posterior dislocations at an average follow-up of 12.5 years. Transchondral fractures larger than 4 mm significantly increase this risk.
3. Sciatic Nerve Palsy
Sciatic nerve palsy complicates simple posterior hip dislocations in approximately 10% to 13% of patients. Neurological sequelae are virtually non-existent in anterior dislocations.
The peroneal division of the sciatic nerve is disproportionately affected compared to the tibial branch. This is due to its anatomical tethering at the sciatic notch and fibular neck, its more lateral position making it vulnerable to the posteriorly displaced femoral head, and its internal morphology (larger fascicles with less supportive connective tissue).
Management: If a deficit is noted pre-reduction, the hip should be reduced promptly. At least partial recovery of nerve function can be expected in approximately two-thirds of patients over 12 to 18 months. Ankle-foot orthoses (AFO) are prescribed for foot drop.
Surgical Exploration: Tornetta and Mostafavi recommend immediate surgical exploration of the sciatic nerve only if sciatic function was completely normal before reduction and acutely deteriorated after closed reduction, suggesting iatrogenic entrapment of the nerve within the joint.
4. Recurrent Instability
Recurrent instability is exceedingly rare after a simple hip dislocation without fracture. When it does occur, it is typically caused by massive unhealed capsular defects, labral avulsions, or generalized capsular laxity. Surgical management involves open capsular shift, labral repair, and occasionally bone block augmentation if soft-tissue repair alone is insufficient to restore intraoperative stability.
📚 Medical References
- hip dislocation, J Pediatr Orthop 11:542, 1991.
- Taylor GR, Clarke NM: Surgical release of the “snapping iliopsoas tendon,” J Bone Joint Surg 77B:881, 1995.
- Painful Paraarticular Calcifi cations, Bursitis, and Tendinitis Ark TW, Flock TJ, Flatow EL, et al: Arthroscopic treatment of calcifi c tendinitis of the shoulder, Arthroscopy 8:183, 1992.
- Baker CL, Cummings PD: Arthroscopic management of miscellaneous elbow disorders, Oper Tech Sports Med 6:16, 1998.
- Baker WM: On the formation of synovial cysts in the leg in connection with disease in the knee joint, St Bartholomew Hosp Rep 13:245, 1877.
- Breck LW, Higinbotham NL: Patellar and olecranon bursitis: with the report of an improved operative procedure, Milit Surg 98:396, 1946.
- Bryan RS, DiMichele JD, Ford GL Jr: Popliteal cysts: arthrography as an aid to diagnosis and treatment, Clin Orthop Relat Res 50:203, 1967.
- Burleson RJ, Bickel WH, Dahlin DC: Popliteal cysts: a clinicopathological survey, J Bone Joint Surg 38A:1265, 1956.
- Childress HM: Posterior medial meniscal lesions and popliteal cysts, J Bone Joint Surg 47A:1272, 1965.
- Cooperman MB: Acute hematogenous bursitis, Ann Surg 108:1094, 1938.
- Crenshaw AH, Kilgore WE: Surgical treatment of bicipital tenosynovitis, J Bone Joint Surg 48A:1496, 1966.
- DePalma AF: Surgery of the shoulder, Philadelphia, 1950, JB Lippincott. DePalma AF: The painful shoulder, Postgrad Med 21:368, 1957.
- Dirschl DR, Lachiewicz PF: Dissecting popliteal cyst as the presenting symptom of a malfunctioning
