Introduction and Historical Context
In the modern era of highly successful total hip arthroplasty (THA), hip arthrodesis is an infrequently performed procedure. However, it remains a critical salvage operation and a primary option for a highly select demographic: young, active laborers with unilateral end-stage hip disease (e.g., post-traumatic osteoarthritis, sequelae of slipped capital femoral epiphysis, or chronic infection) who would rapidly wear out or loosen a prosthetic joint.
The first successful arthrodesis of the hip was reported in 1894 by Heusner in Germany, performed on a patient with an old congenital hip dislocation. While arthrodesis provides a stable, painless limb capable of enduring heavy physical labor, the long-term biomechanical consequences on adjacent joints are significant.
Long-Term Sequelae and Adjacent Segment Degeneration
The rigid lever arm of a fused hip transfers immense mechanical stress to the lumbar spine, the ipsilateral knee, and the contralateral hip. Long-term follow-up studies reveal a predictable pattern of adjacent segment degeneration:
* Lumbar Spine: Symptomatic degenerative changes occur in 55% to 100% of patients. Hyperlordosis compensates for the lack of hip extension, leading to facet arthropathy and spinal stenosis.
* Ipsilateral and Contralateral Knee: Problems occur in 45% to 68% of patients, largely due to altered gait mechanics and increased valgus/varus thrusts during the stance phase.
* Contralateral Hip: Degenerative changes are reported in 25% to 63% of patients.
Callaghan et al. and Sponseller et al. noted that while ipsilateral knee pain and contralateral hip pain occur less frequently than low back pain, they more often require operative intervention—usually in the form of total knee or hip arthroplasty. Patient satisfaction varies widely. Roberts and Fetto reported good or excellent functional results and high patient satisfaction at an average 8.5-year follow-up in 10 patients. Conversely, Barnhardt and Stiehl reported that only three of their six patients would choose arthrodesis over THA retrospectively, citing debilitating low back pain, limited ambulation, and sexual dysfunction.
💡 Clinical Pearl: Future Conversion to THA
When performing a hip arthrodesis today, the surgeon must anticipate the eventual need for conversion to a total hip arthroplasty (takedown of fusion) 15 to 20 years later. Surgical techniques that preserve the abductor musculature (gluteus medius and minimus) and minimize distortion of the proximal femoral anatomy are strongly preferred.
Biomechanics and Optimal Positioning
Regardless of the surgical technique selected, the three-dimensional spatial orientation of the fused hip is the single most critical factor in determining the patient's postoperative gait efficiency and long-term adjacent joint survival.
The hip must be fused in:
* Flexion: 25 to 30 degrees. This allows the patient to sit comfortably without excessive posterior pelvic tilt while permitting a relatively normal stride length during ambulation.
* Adduction/Abduction: Neutral (0 degrees) to 5 degrees of adduction. Excessive abduction forces the pelvis to tilt downward on the contralateral side, creating an apparent leg-length discrepancy and severe strain on the lumbar spine.
* Rotation: 0 to 15 degrees of external rotation. Internal rotation is poorly tolerated and leads to a clumsy, toe-in gait that exacerbates knee pathology.
Surgical Techniques for Hip Arthrodesis
Successful arthrodesis can be achieved through a variety of methods. The choice of technique depends on the patient's age, bone quality, presence of the femoral head, and the surgeon's familiarity with the implants.
Arthrodesis with Cancellous Screw Fixation
Benaroch et al. described a straightforward, minimally disruptive method of hip arthrodesis particularly suited for adolescent patients. This technique utilizes simple cancellous screws and a subtrochanteric osteotomy to neutralize deforming forces.
Surgical Steps:
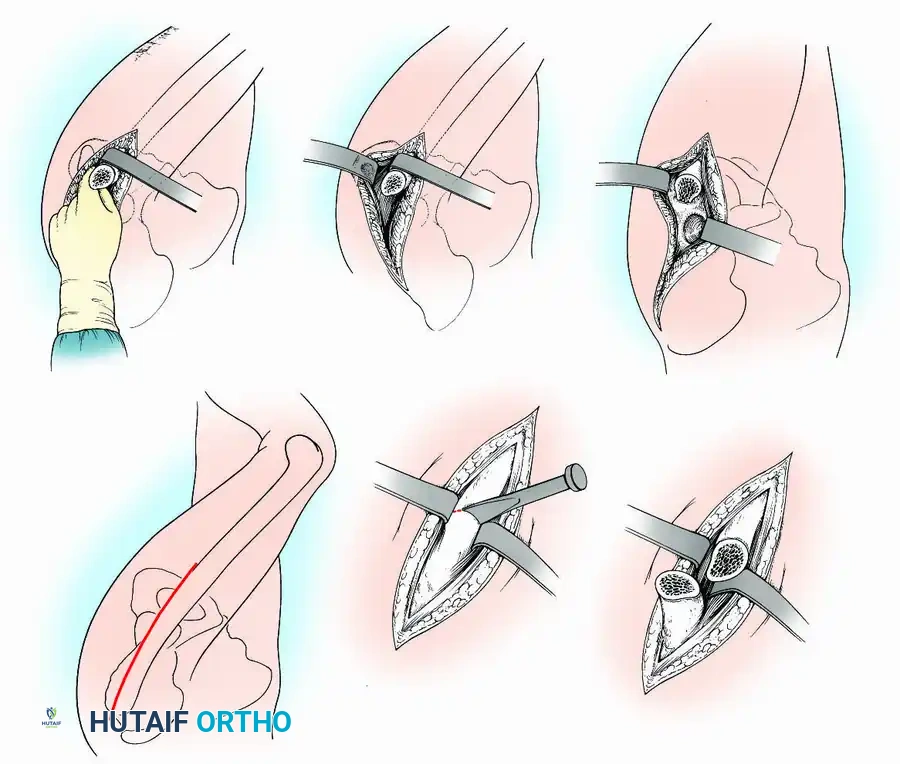
1. Approach: An anterolateral approach is utilized. An anterior capsulotomy is performed to expose the joint.
2. Joint Preparation: The femoral head is dislocated anteriorly. Both the acetabulum and the femoral head are aggressively denuded of all articular cartilage and necrotic bone down to bleeding subchondral bone.
3. Positioning and Fixation: The limb is positioned to allow maximal congruency between the prepared femoral head and acetabulum. One or two large-diameter cancellous screws are passed from the inner surface of the ilium, across the joint space, to engage the femoral head.
4. Subtrochanteric Osteotomy: Before final tightening and compression of the screws, a subtrochanteric osteotomy is performed. This is a critical step; it decompresses the long biomechanical lever arm of the femur, protecting the intra-articular fusion site from micromotion and shear forces.
⚠️ Surgical Warning: Adduction Drift
Benaroch et al. noted a progressive drift into adduction averaging 7 degrees, mostly occurring within the first 2 years postoperatively. To counteract this, they recommend fusing the hip in 20 to 25 degrees of flexion and neutral or 1 to 2 degrees of abduction initially, anticipating the drift.
Radiographic confirmation of screw trajectory and joint compression in cancellous screw fixation.
Arthrodesis with a Muscle-Pedicle Bone Graft
Described by Davis in 1954, this technique transfers a portion of the anterior ilium—along with its vascularized muscle pedicle (tensor fascia lata and anterior fibers of the gluteus medius/minimus)—to bridge the hip joint. While the original technique included an intertrochanteric osteotomy, modern iterations often omit this step, relying instead on rigid internal fixation with Knowles pins or cannulated screws.
Surgical Technique 3-14:
* Incision: Begin an anterior iliofemoral incision 7.5 cm posterior to the anterior superior iliac spine (ASIS). Extend it along the anterior crest of the ilium to the ASIS, then curve it distally and posteriorly to end near the base of the greater trochanter.
* Exposure: Deepen the incision to the iliac crest. Identify the internervous plane between the sartorius and tensor fasciae latae. Detach the sartorius from its origin and retract it medially.
* Graft Harvest: By subperiosteal dissection, separate the abdominal aponeurosis and iliacus minor from the superior and medial ilium. Direct an osteotome longitudinally, then laterally, to cut a graft from the anterior crest. The graft remains attached to its muscle pedicle (tensor fasciae latae, anterior gluteus medius/minimus).
* Joint Preparation: Detach the straight head of the rectus femoris, open the capsule, and dislocate the joint. Perform a routine intra-articular denudation of cartilage. Reduce the hip.
* Slot Creation: Make a slot in the ilium above the acetabulum and in the anterior part of the head and neck of the femur to receive the graft.
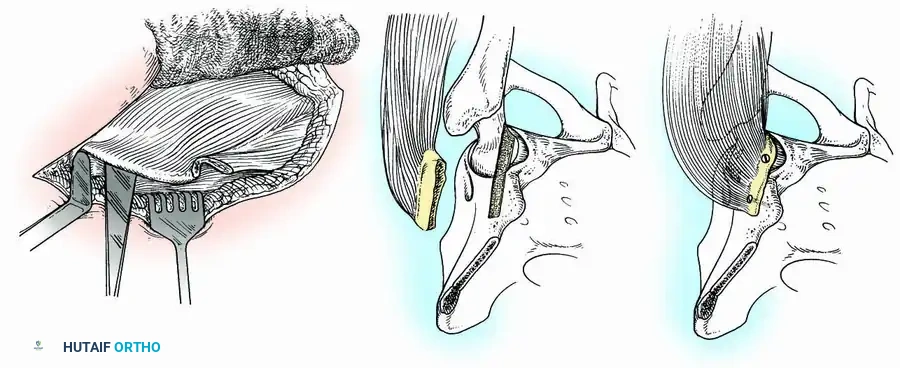
Fig. 3-34: Arthrodesis of hip with muscle-pedicle bone graft. (A) Osteotome placement. (B) Slot creation in ilium and femoral head. (C) Graft fixed with screws.
- Fixation: Place the graft into the slot and secure it with screws (one in the ilium, one in the femoral neck). Alternatively, place the wide free surface of the graft on a flat bed prepared on the ilium and femur, fixing it with several pins.
- Closure: Close the wound in layers over a suction drain.
Postoperative Protocol: Historically, this required 12 weeks of spica cast immobilization. Modern rigid fixation may allow for a modified orthosis, but strict non-weight-bearing is maintained until radiographic union is evident.
Arthrodesis with Cobra Plate Fixation
Developed by Schneider and modified by Murrell and Fitch, the cobra-head plate provides exceptionally rigid internal fixation. Crucially, this technique involves a greater trochanteric osteotomy to preserve the abductor mechanism, facilitating future conversion to a THA. It also utilizes a medial displacement osteotomy of the pelvis to improve biomechanics.
⚠️ Pitfall: High BMI and Pseudarthrosis
Klemme et al. reported that adolescent patients ranking at or above the 90th percentile for weight-for-age are at a significantly higher risk of pseudarthrosis with cobra plating. In these patients, supplementary stabilization (e.g., anterior column screws or a spica cast) is mandatory. Furthermore, the distal end of the rigid plate creates a stress riser, increasing the risk of periprosthetic femoral fractures from minor trauma.
Surgical Technique 3-15:
* Positioning: Place the patient supine with a sandbag under the ipsilateral buttock. Drape to allow access to both iliac crests and ankles for alignment checks.
* Approach: Make a linear longitudinal midlateral incision along the femoral diaphysis, extending 8 cm distal to the greater trochanter. Open the fascia lata and protect the sciatic nerve.
* Trochanteric Osteotomy: Incise the vastus lateralis origin. Use an oscillating saw to perform a greater trochanteric osteotomy, ensuring the proximal fragment retains the insertion of the gluteus medius and minimus. Elevate this fragment superiorly and pin it temporarily to the iliac wing.
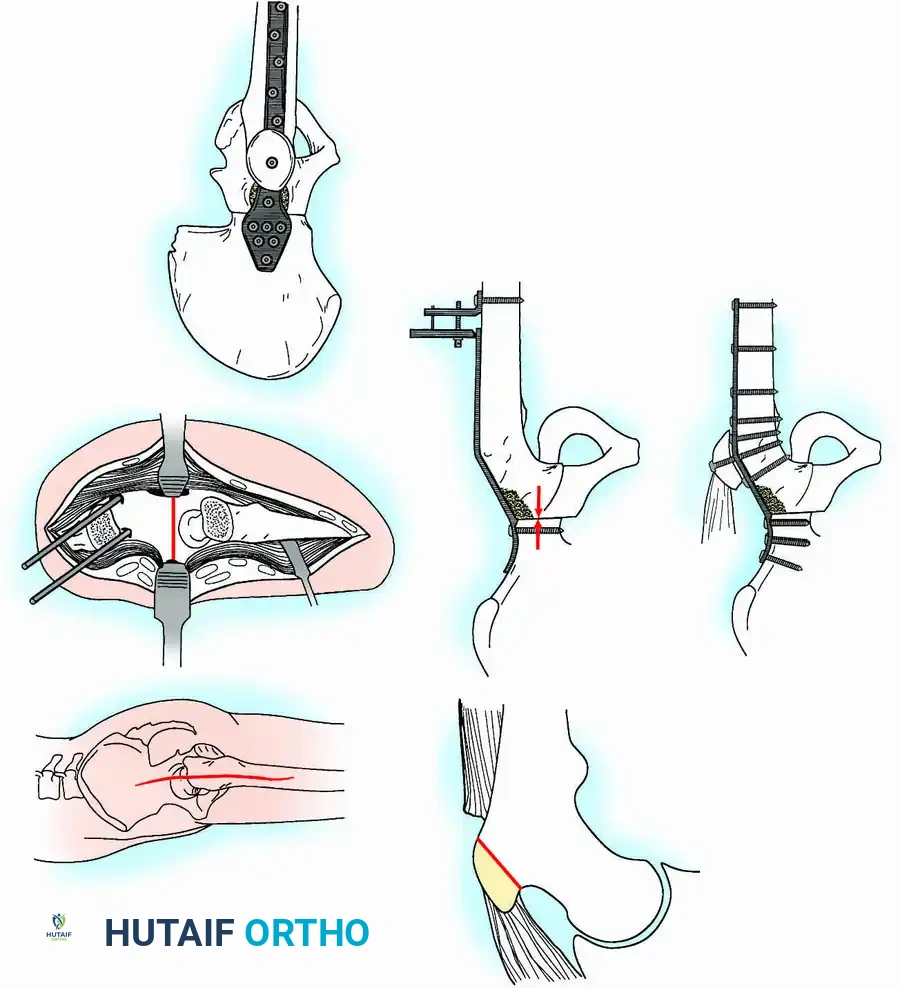
Fig. 3-35 (A-F): Hip arthrodesis with cobra plate fixation. Note the trochanteric osteotomy and transverse innominate osteotomy.
- Innominate Osteotomy: Perform a superior hip capsulotomy. Make a transverse innominate osteotomy between the iliopectineal eminence and the sciatic notch. Remove a 0.5-cm wafer of bone from the superior femoral head.
- Medial Displacement: Displace the distal hemipelvic fragment and proximal femur medially by 100% of the thickness of the innominate bone. This medialization reduces the joint reaction force.
- Alignment: Remove the sandbag. Insert Steinmann pins into both ASIS to act as a reference plane. Position the hip in 25 degrees of flexion, neutral rotation, and neutral adduction/abduction.
- Plating and Compression: Contour a nine-hole cobra plate. Secure the proximal portion to the ilium with a 4.5-mm cortical screw. Distal to the plate, attach an AO tensioner to the lateral femur. Apply compression force across the hip joint to ensure rigid bony apposition.
- Final Fixation: Secure the plate to the femur with 4.5-mm bicortical screws. Reattach the greater trochanter over the plate using a 4.5-mm cortical screw and washer.
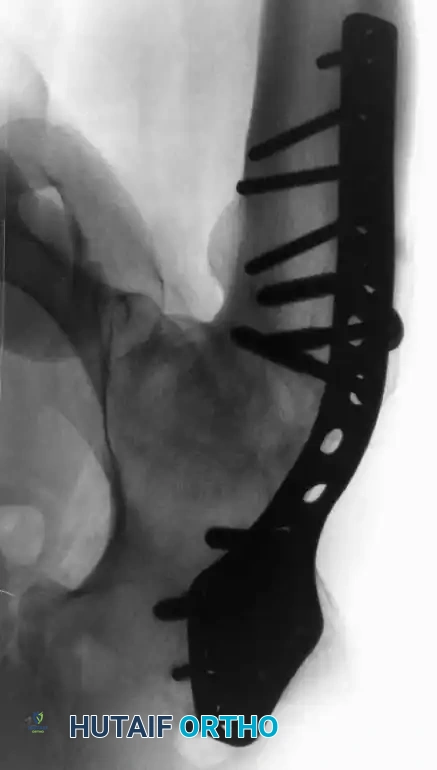

Fig. 3-35 (G): Final radiographic and diagrammatic appearance of the cobra plate construct with reattached greater trochanter.
Postoperative Protocol: No postoperative immobilization is strictly required. Ambulation with partial weight-bearing (two crutches) is encouraged on day 2 or 3 and continued for 6 weeks.
Arthrodesis with Hip Compression Screw Fixation
Pagnano and Cabanela popularized the use of a sliding hip compression screw (dynamic hip screw) supplemented by cancellous screws. This construct offers several distinct advantages:
1. It ensures the hip is fused in the proper position, minimizing low back pain.
2. It provides dynamic compression across the fusion site, promoting primary bone healing.
3. It avoids bulky hardware that might damage the abductor muscles, preserving them for future THA.
4. It minimizes the need for postoperative spica casting.

Intraoperative fluoroscopy demonstrating the trajectory of the sliding hip compression screw across the denuded joint space.
Technique Overview:
Following standard joint denudation, the hip is positioned optimally. A guide wire is passed from the lateral proximal femur, through the femoral neck, and deep into the thickest portion of the ilium (above the acetabular dome). The tract is reamed, and a large lag screw is inserted. A side plate is applied to the lateral femur, and compression is achieved. Two or three additional cancellous screws are placed proximal to the hip screw to provide rotational stability.

Final construct showing the dynamic hip screw and supplementary anti-rotation cancellous screws.
Postoperative Protocol: Patients are evaluated at 12 to 14 weeks. If stable union is questionable, a removable polypropylene orthosis is used for another 4 to 6 weeks. Full recovery often takes 6 months. Routine removal of the hardware is advisable after 18 months to promote bone remodeling and facilitate future conversion to THA.
Arthrodesis in the Absence of the Femoral Head
In cases of severe infection, osteonecrosis, nonunion of the femoral neck, or failed total hip arthroplasty, the femoral head may be completely absent or destroyed. In 1931, Abbott and Fischer designed a salvage method for these complex scenarios.
Surgical Technique 3-16:
* Positioning: Position the patient supine on a fracture table.
* Approach: Utilize a Watson-Jones (anterolateral) approach to the hip. Develop the interval between the gluteus medius and the tensor fasciae latae.
* Exposure: Detach the anterior third of the gluteus medius from the greater trochanter to improve access. Externally rotate the leg and detach the reflected head of the rectus femoris.
* Debridement: Perform a complete anterior capsulectomy. Dislocate the proximal femur and place the leg in a figure-four position. Use aggressive curettage and motorized reamers to remove all remaining cartilage, fibrous tissue, and necrotic bone from the acetabulum until a bleeding cancellous bed is obtained.
* Preparation of the Femur: If the femoral neck is present, it is shaped to fit the acetabulum. If absent, the greater trochanter is decorticated and levered into the acetabulum.
* Staging: This procedure is often done in stages. The first stage involves placing the proximal femur into the acetabulum in wide abduction to ensure contact. A subsequent subtrochanteric osteotomy is performed weeks later to bring the femoral shaft into the functional alignment (25° flexion, neutral adduction).
Conclusion
Hip arthrodesis is a technically demanding procedure that requires a profound understanding of pelvic and lower extremity biomechanics. While the advent of highly durable arthroplasty implants has narrowed its indications, it remains an indispensable tool in the orthopedic surgeon's armamentarium for the young, heavy-laboring patient or as a salvage for intractable infection. Meticulous attention to the three-dimensional position of the fusion, rigid internal fixation, and preservation of the abductor musculature are paramount to achieving a successful, durable outcome that leaves the door open for future reconstructive options.
