Comprehensive Introduction and Patho-Epidemiology
Haglund deformity, colloquially and historically referred to as a "pump bump" or "winter heel," represents a complex triad of hindfoot pathologies encompassing an abnormal osseous prominence of the posterosuperior calcaneal tuberosity, profound retrocalcaneal bursitis, and an adventitious superficial pretendinous Achilles bursitis. Originally described by the Swedish orthopedic surgeon Patrick Haglund in 1927, this condition has evolved in our understanding from a simple osseous anomaly to a dynamic, mechanically induced soft-tissue and bony impingement syndrome. Understanding the intricate interplay between the calcaneal morphology and the Achilles tendon insertion is paramount for the orthopedic surgeon evaluating and treating this recalcitrant condition.
The cellular pathophysiology of Haglund syndrome is driven by repetitive mechanical microtrauma rather than a primary systemic inflammatory process. Chronic irritation, classically from a rigid shoe heel counter, aggressively compresses the superficial bursa, the Achilles tendon substance, and the deeper retrocalcaneal bursa against the prominent posterosuperior calcaneus. This relentless compression during the gait cycle induces a cascade of localized tissue hypoxia, microvascular proliferation, and angiofibroblastic hyperplasia within the tendon and bursal tissues. Over time, this repetitive microtrauma leads to chronic inflammation, profound bursal hypertrophy, and eventually, insertional Achilles tendinopathy characterized by mucoid degeneration and intratendinous calcification.
Demographically, the classical presentation of this deformity exhibits a distinct bimodal distribution. It occurs most frequently in young women in their second and third decades of life, correlating strongly with the use of restrictive, rigid-heeled footwear—hence the colloquial moniker. However, a second distinct peak occurs in middle-aged, active individuals, particularly runners and jumping athletes, where the repetitive dorsiflexion of the ankle against a morphologically prominent calcaneus precipitates the impingement triad independently of restrictive footwear. Furthermore, underlying biomechanical foot variants, such as a rigid cavovarus foot structure or a compensated forefoot valgus, can exacerbate the mechanical lever arm of the calcaneus, significantly increasing the vector forces applied to the retrocalcaneal space.
Differentiating pure Haglund deformity with isolated retrocalcaneal bursitis from advanced insertional Achilles tendinopathy is critical for both preoperative surgical planning and accurate patient prognostication. Patients presenting solely with bursal inflammation and an osseous prominence generally experience a more predictable surgical outcome with isolated exostectomy and bursectomy. Conversely, those with extensive intrasubstance tendinosis or intratendinous ossification require aggressive tendon debridement, detachment, and potential reconstruction, which significantly alters the rehabilitative timeline and the ultimate functional ceiling of the patient.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the posterior hindfoot anatomy is non-negotiable for the orthopedic surgeon undertaking the correction of Haglund syndrome. The Achilles tendon, representing the confluence of the gastrocnemius and soleus aponeuroses, is the largest and strongest tendon in the human body. Unlike tendons traversing synovial joints, the Achilles lacks a true synovial sheath. Instead, it is enveloped by a highly vascularized paratenon composed of a single layer of cells that supplies its extrinsic vascularity. This blood supply is notably tenuous in the "watershed area," located approximately 2 to 6 cm proximal to its insertion, a region notoriously susceptible to non-insertional tendinopathy and spontaneous rupture, though insertional pathology is driven by a different vascular dynamic primarily supplied by the osseous footprint.
At the insertion site, the Achilles tendon exhibits a broad, crescentic footprint on the middle third of the posterior calcaneal tuberosity. The insertion is anatomically complex, with fibers spiraling approximately 90 degrees from their origin to their insertion, allowing for elastic energy storage and dynamic load distribution. Two distinct bursae dictate the clinical pathology in Haglund syndrome. The retrocalcaneal bursa is a constant, anatomically native, horseshoe-shaped synovial bursa situated between the anterior aspect of the distal Achilles tendon and the posterosuperior calcaneal tuberosity. Its physiological role is to reduce friction and dissipate compressive forces between the tendon and the bone during extreme ankle dorsiflexion.
Conversely, the superficial pretendinous bursa is an adventitious structure that develops between the posterior aspect of the Achilles tendon and the overlying skin. According to anatomical studies by Jones, this bursa is not universally present; it is found in approximately 50% of patients and forms primarily as a physiological, hyperkeratotic response to chronic external friction, such as that caused by shoe wear. When inflamed, this bursa becomes a thick, fluid-filled sac that contributes significantly to the visible posterior heel prominence and the patient's acute pain profile.
Biomechanically, the posterosuperior prominence of the calcaneus acts as a fulcrum against the anterior fibers of the Achilles tendon during ankle dorsiflexion. In a normal gait cycle, as the tibia advances over the plantigrade foot (terminal stance phase), the ankle passively dorsiflexes, pulling the Achilles tendon tightly against the posterosuperior calcaneus. If the calcaneal pitch is abnormally high (as seen in cavus feet) or if the posterosuperior tuberosity is structurally enlarged, the retrocalcaneal bursa is violently compressed. This mechanical impingement generates sheer forces that fray the anterior tendon fibers, initiating the degenerative cascade that culminates in insertional tendinosis, cartilaginous metaplasia, and eventual heterotopic ossification within the tendon substance.
Exhaustive Indications and Contraindications
Surgical intervention for Haglund deformity and retrocalcaneal bursitis is strictly reserved for patients who have demonstrably failed a comprehensive, structured, and prolonged course of non-operative management. The orthopedic surgeon must exercise extreme prudence, as the posterior heel is a notoriously unforgiving anatomical region characterized by tenuous vascularity, thin soft-tissue envelopes, and high mechanical demands. Conservative measures must be exhausted over a minimum of 3 to 6 months. These include rigid shoe wear modification (transitioning to open-heeled or soft-backed footwear), the utilization of heel lifts (to subtly plantarflex the ankle and decompress the retrocalcaneal space), targeted eccentric loading physical therapy protocols, and judicious use of nonsteroidal anti-inflammatory drugs (NSAIDs). Corticosteroid injections within the retrocalcaneal bursa remain highly controversial due to the profound risk of iatrogenic Achilles tendon rupture and should generally be avoided or utilized with extreme caution under ultrasound guidance.
When conservative modalities fail to provide functional relief, surgical intervention becomes indicated. The primary goal of surgery is to eradicate the mechanical impingement by resecting the offending osseous prominence, excising the inflamed bursal tissues, and debriding any degenerative tendon substance. The specific surgical algorithm—ranging from isolated endoscopic calcaneal exostectomy to open extensive debridement with flexor hallucis longus (FHL) tendon transfer—is dictated by the degree of tendon involvement, the extent of intratendinous calcification, and the patient's functional demands.
Contraindications to surgical intervention must be rigorously evaluated during the preoperative assessment. Patients with severe peripheral vascular disease, uncontrolled diabetes mellitus with neuropathy, or active local skin infections are at an unacceptably high risk for catastrophic wound complications and deep infections. Furthermore, patients who are unwilling or unable to comply with the strict, prolonged postoperative non-weight-bearing and rehabilitative protocols are poor surgical candidates.
| Category | Absolute Parameters | Relative Parameters |
|---|---|---|
| Indications | Failure of >6 months of targeted conservative therapy; Intractable pain limiting activities of daily living; Impending skin necrosis over the prominence. | Failure of 3-6 months of conservative therapy in high-demand athletes; Progressive intratendinous calcification on serial imaging. |
| Contraindications | Active local or systemic infection; Severe peripheral arterial disease (ABI < 0.4); Medically unstable for anesthesia; Non-ambulatory status. | Uncontrolled diabetes mellitus (HbA1c > 8.0%); Heavy tobacco use (requires cessation protocol); Poor patient compliance; Chronic regional pain syndrome (CRPS). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment
A meticulous clinical assessment is the foundation of successful surgical planning. Patients typically present with a chief complaint of sharp, localized posterior heel pain that is unequivocally exacerbated by walking up inclines, running, or wearing closed-heel shoes. Physical examination routinely reveals a palpable, often erythematous, and indurated osseous prominence at the posterolateral aspect of the heel. The surgeon must precisely localize the maximal point of tenderness. In isolated Haglund syndrome, tenderness is usually localized anterior to the Achilles tendon—a finding best elicited by the "two-finger squeeze test," where the examiner compresses the retrocalcaneal space just anterior to the medial and lateral borders of the tendon. Tenderness within the tendon substance itself strongly suggests concomitant insertional Achilles tendinopathy, which will necessitate a more aggressive surgical debridement. The Silfverskiöld test must also be performed to evaluate for isolated gastrocnemius contracture, which may require a concurrent gastrocnemius recession to normalize hindfoot biomechanics.
Radiographic Templating
Standard weight-bearing radiographs of the foot and ankle (lateral, anteroposterior, and axial calcaneal views) are mandatory for all surgical candidates. The lateral weight-bearing radiograph is the cornerstone of preoperative templating. The surgeon should systematically evaluate several key radiographic parameters. The Fowler-Philip Angle, measured between the inferior border of the calcaneus and the posterior border of the calcaneal tuberosity, is historically significant; an angle greater than 75 degrees suggests a pathological posterosuperior prominence. However, modern orthopedic consensus favors the Parallel Pitch Lines (Chauveaux-Liet) as a more reliable indicator. In this method, a baseline is drawn along the plantar calcaneal tuberosity, and a parallel line is drawn through the posterior articular facet. If the osseous prominence extends superior to this upper parallel pitch line, a pathological Haglund deformity is confirmed. Furthermore, the presence of intratendinous calcification or enthesophytes must be documented, as this indicates chronic degenerative tendinopathy and dictates the extent of required surgical debridement.
Advanced imaging, specifically Magnetic Resonance Imaging (MRI) without contrast, is highly recommended and often considered standard of care if the surgeon suspects significant intrasubstance Achilles degeneration. MRI provides unparalleled visualization of the retrocalcaneal bursa, the extent of mucoid degeneration within the tendon, and the presence of partial-thickness or longitudinal split tears. If the MRI reveals that more than 50% of the tendon insertion is severely degenerated and requires excision, the surgeon must preoperatively plan for an FHL tendon transfer to augment the deficient Achilles footprint.
Patient Positioning and Anesthesia Setup
Flawless execution of the surgical procedure begins with optimal patient positioning and anesthesia. The procedure is typically performed under general anesthesia or a regional popliteal sciatic nerve block combined with deep intravenous sedation. The regional block provides excellent intraoperative muscle relaxation and profound postoperative analgesia, significantly reducing opioid consumption.
The patient is placed in the prone position on a standard operating table. Generous padding must be applied to all bony prominences, particularly the anterior superior iliac spines, the patellae, and the contralateral limb. The operative lower extremity is prepped and draped in a standard sterile fashion to above the knee. A pneumatic thigh or calf tourniquet is applied to provide a pristine, bloodless surgical field, which is critical for identifying the sural nerve and assessing the quality of the tendon tissue. The tourniquet is inflated to standard pressures (typically 250-300 mmHg) only after meticulous exsanguination of the limb using an Esmarch bandage.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Exposure
The gold standard for addressing Haglund deformity involves a meticulously planned open approach. The surgeon makes a longitudinal lateral incision approximately 1 cm lateral to the lateral border of the Achilles tendon. The incision should extend distally from 3 to 4 cm proximal to the superior tuberosity of the calcaneus, down to 2 to 3 cm distal to the superior tuberosity. Strict adherence to a lateral approach is imperative; a medial approach places the posterior tibial artery and tibial nerve at unwarranted risk. However, the lateral approach requires meticulous superficial dissection to identify, mobilize, and protect the sural nerve, which predictably crosses the lateral border of the Achilles tendon in the proximal aspect of the incision.
Once the subcutaneous tissues are carefully parted, the ankle joint is plantarflexed to reduce tension on the Achilles tendon and the posterior soft tissues. By sharp and blunt dissection, the lateral border of the Achilles tendon is definitively identified. The paratenon is incised longitudinally and gently retracted using fine stay sutures or atraumatic forceps. Preserving the paratenon is critical, as it must be repaired during closure to prevent catastrophic skin adhesions and to optimize tendon gliding. A right-angle or Hohmann retractor is then placed between the anterior aspect of the Achilles tendon and the posterior/superior borders of the calcaneal tuberosity. With the foot held in maximal plantar flexion, this maneuver usually affords sufficient exposure to visualize the retrocalcaneal bursa and the Haglund lesion without raising the Achilles tendon off its calcaneal footprint.
The Calcaneal Exostectomy and Bursectomy
With the posterosuperior calcaneal tuberosity adequately exposed, a thorough retrocalcaneal bursectomy is performed. All inflamed, hypertrophic synovial tissue must be aggressively excised using a rongeur and electrocautery, ensuring clear visualization of the osseous impingement lesion. The Achilles tendon has an extensive, broad insertion into the posterior and plantar aspects of the calcaneal tuberosity. If exposure of the bone remains inadequate, raising a 1- to 2-cm-long portion of the lateral tendon insertion may be necessary to resect the bone safely.
The osteotomy is the most critical step of the procedure. The surgeon removes the superior aspect of the tuberosity (the Haglund lesion) using a microsagittal saw or a sharp, broad osteotome. A critical technical pearl is the placement of several transverse drill holes (using a 2.0 mm or 2.5 mm drill bit) along the proposed osteotomy site to create a perforation line. This technique prevents the osteotomy from inadvertently propagating distally into the body of the calcaneus, which could create a dangerous stress riser and subsequent calcaneal fracture. The resection must be generous; under-resection is the most common cause of persistent postoperative pain and surgical failure. The final cut should slope anteriorly and distally, ensuring no sharp medial or lateral cortical ridges remain that could abrade the anterior tendon fibers during dorsiflexion. The raw cancellous bone surface is then smoothed with a rasp and sealed with bone wax to minimize postoperative hematoma formation.
Addressing Intratendinous Calcification and Tendon Repair
If preoperative imaging or intraoperative inspection reveals an area of ossification or severe mucoid degeneration within the tendon substance, the Achilles tendon must be split longitudinally in a coronal plane distally. The surgeon elevates the anterior third or half of the tendon to free up enough tissue to meticulously excise the calcified, necrotic, and degenerative tendon elements until healthy, bleeding tendon margins are achieved.
Following aggressive debridement, the integrity of the remaining Achilles tendon must be assessed. If less than 50% of the tendon was detached or debrided, primary repair is sufficient. The split tendon is repaired with heavy, non-absorbable synthetic sutures (e.g., #2 FiberWire or similar ultra-high-molecular-weight polyethylene suture) using a Krackow or similar locking stitch technique. Double-loaded suture anchors (typically 4.5 mm to 5.5 mm in diameter) are placed into the calcaneal footprint to firmly reattach any reflected portion of the tendon, ensuring a robust, knotless, or securely knotted fixation that compresses the tendon against the bleeding bone bed to facilitate biological healing.
Advanced Reconstruction: FHL Tendon Transfer
In cases of severe, chronic Haglund syndrome with concomitant advanced insertional Achilles tendinopathy, the surgeon may be forced to debride more than 50% of the Achilles tendon insertion to achieve healthy tissue margins. In such scenarios, the remaining Achilles tendon is biomechanically insufficient. Augmentation is absolutely required to prevent catastrophic postoperative rupture and to restore functional plantar flexion power. The Flexor Hallucis Longus (FHL) tendon is the ideal, gold-standard transfer candidate due to its anatomical proximity, its in-phase firing pattern with the gastroc-soleus complex, and its robust cross-sectional area. The modified Mann technique is highly recommended for this augmentation.
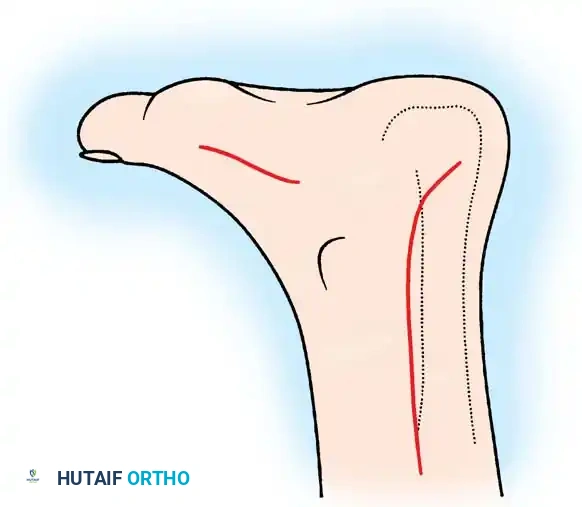
Incisions for exposure and harvest of the flexor hallucis longus tendon. A medial midfoot incision is utilized to harvest the tendon at the Master Knot of Henry, while the posterior incision is used for the calcaneal transfer.
The FHL harvest begins with a longitudinal incision along the medial arch of the foot to expose the plantar fascia and the underlying musculature. Deep dissection is carried out to identify the Master Knot of Henry, the anatomical crossroad where the FHL crosses dorsal to the Flexor Digitorum Longus (FDL).
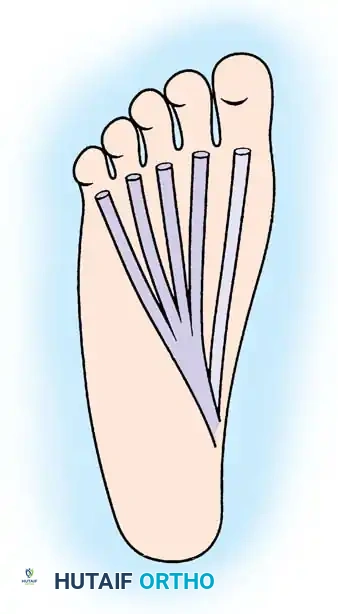
Plantar view demonstrating the anatomical relationship between the flexor digitorum longus (FDL) and the adjacent flexor hallucis longus (FHL) tendon prior to harvest.
Once identified, the FHL tendon is transected as distally as possible to maximize graft length. To prevent the loss of active interphalangeal joint flexion of the hallux—a complication that can lead to toe-off weakness during gait—a tenodesis is performed by anastomosing the distal stump of the FHL to the adjacent intact FDL tendon using non-absorbable sutures.
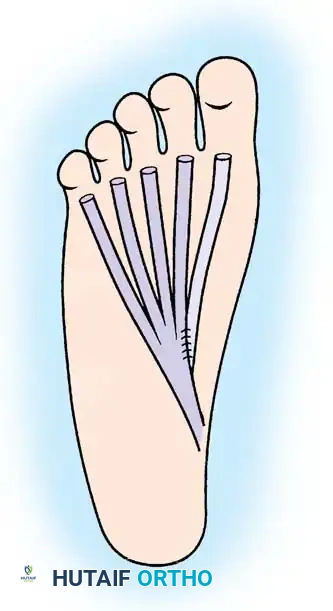
Anastomosis of the distal stump of the FHL tendon to the FDL tendon, ensuring preservation of distal toe flexion.
The proximal stump of the FHL tendon is then withdrawn into the posterior ankle incision. A transverse drill hole (typically 6.0 mm to 7.0 mm, depending on graft diameter) is created through the calcaneus, positioned anterior to the Achilles footprint. The FHL tendon is passed through this drill hole from medial to lateral.
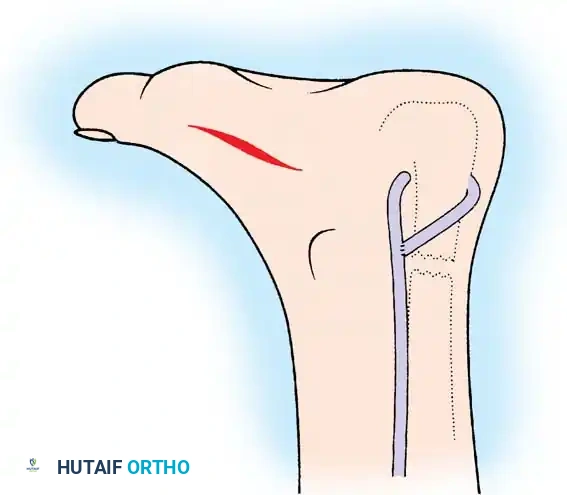
The FHL tendon is pulled through the transverse drill hole in the calcaneus and tensioned appropriately to augment plantar flexion.
With the ankle held in approximately 15 to 20 degrees of plantar flexion to set the appropriate resting tension, the FHL tendon is tensioned and either sutured back onto itself (if length permits) or, more commonly in modern practice, secured with a bio-tenodesis interference screw directly within the calcaneal tunnel. The wound is then copiously lavaged, the paratenon is closed over the Achilles tendon, and the skin is closed meticulously using a non-strangulating technique (e.g., Allgöwer-Donati sutures) to respect the tenuous posterior heel vascularity.
Complications, Incidence Rates, and Salvage Management
Surgical management of the posterior heel is fraught with potential complications, primarily due to the thin soft-tissue envelope, poor vascularity, and extreme mechanical forces exerted across the ankle joint. The orthopedic surgeon must be intimately familiar with these risks, actively employ preventative intraoperative strategies, and possess the technical acumen to execute salvage procedures when necessary.
Wound breakdown and superficial infection are the most common postoperative complications, occurring in up to 10% of open procedures. The posterior heel skin is supplied by small calcaneal branches of the peroneal and posterior tibial arteries, which are easily devascularized by aggressive retraction or strangulating suture techniques. Sural nerve injury is another significant risk, particularly with the lateral approach. Neuromas of the sural nerve can be devastatingly painful and often require subsequent surgical excision and burying of the nerve stump into local muscle or bone.
Mechanical failures, such as under-resection of the Haglund deformity or iatrogenic Achilles tendon rupture, represent severe technical errors. Under-resection is the leading cause of persistent postoperative pain and requires revision exostectomy. Over-resection or failure to utilize drill holes can lead to an iatrogenic avulsion fracture of the calcaneal tuberosity, a catastrophic complication requiring immediate open reduction and internal fixation (ORIF).
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 5% - 10% | Meticulous soft-tissue handling; Avoid excessive retraction; Use Allgöwer-Donati skin sutures; Strict postoperative elevation. | Local wound care; Negative pressure wound therapy (VAC); Sural artery fasciocutaneous flap for deep, exposed tendon defects. |
| Sural Nerve Neuroma | 2% - 5% | Careful superficial dissection; Identify and protect the nerve early; Avoid blind retractor placement laterally. | Gabapentinoids; Ultrasound-guided nerve blocks; Surgical excision of neuroma and proximal burying into the soleus muscle. |
| Persistent Pain (Under-resection) | 5% - 8% | Use intraoperative fluoroscopy; Ensure osteotomy slopes anteriorly; Resect superior to parallel pitch lines. | Revision surgery for further aggressive exostectomy and bursectomy. |
| Achilles Tendon Rupture / Avulsion | < 2% | FHL augmentation if >50% debrided; Secure anchor fixation; Strict adherence to postoperative NWB and bracing protocols. | Revision reconstruction with FHL transfer, V-Y advancement flap, or allograft reconstruction (e.g., Achilles or semitendinosus). |
Phased Post-Operative Rehabilitation Protocols
The postoperative management of Haglund deformity correction is arguably as critical as the surgical execution itself. The rehabilitative protocol must carefully balance the biological need for tissue healing and tendon incorporation with the biomechanical necessity of preventing profound joint stiffness and muscle atrophy. The protocol is strictly phased, and patient compliance is paramount to avoid catastrophic construct failure.
Phase I: Maximum Protection and Immobilization (Weeks 0-3)
Immediately following wound closure, the patient is placed in a well-padded, short leg, non-weight-bearing (NWB) cast or rigid splint. The ankle must be immobilized in approximately 15 to 20 degrees of equinus (plantar flexion). This specific positioning is critical as it minimizes tension on the repaired Achilles tendon insertion and reduces sheer stress on the posterior skin incision, thereby optimizing local perfusion. Strict elevation of the operative limb above the level of the heart is mandated for the first 7 to 10 days to control edema and mitigate the risk of wound dehiscence. Deep vein thrombosis (DVT) prophylaxis should be considered based on patient risk stratification. At the 2- to 3-week mark, the cast is bi-valved, and the surgical site is inspected. Sutures are typically removed at this stage, provided the incision is fully epithelialized, but the strict non-weight-bearing status must be maintained.
Phase II: Transitional Weight-Bearing and Early Motion (Weeks 3-6)
Once the soft tissues are secure, the patient is transitioned into a removable controlled ankle motion (CAM) walker boot. Crucially, the boot must initially be fitted with stacked heel wedges (typically 2 to 3 wedges) to maintain the ankle in slight plantar flexion, protecting the healing tendon footprint. During this phase, the patient is permitted to initiate active plantar flexion and gentle, active, gravity-assisted dorsiflexion exercises out of the boot. However, passive dorsiflexion stretching is strictly prohibited, as it places excessive tensile loads on the immature tendon repair. Weight-bearing is progressively advanced from touch-down to partial, and eventually to full weight-bearing as tolerated, strictly within the protective confines of the wedged CAM boot.
Phase III: Strengthening and Normalization of Gait (Weeks 6-12)
At the 6-week postoperative mark, the heel wedges are sequentially removed from the CAM boot (typically one wedge every 5 to 7 days) until the patient reaches a neutral plantigrade position. Once neutral is achieved without pain, the patient is weaned from the CAM boot into a supportive, slightly elevated athletic shoe (e.g., a running shoe with a 10mm heel drop). Formal physical therapy is initiated with a heavy emphasis on progressive eccentric strengthening of the gastrocnemius-soleus complex, proprioceptive retraining, and gait normalization. Closed-kinetic-chain exercises, such as seated heel raises progressing to standing bilateral heel raises, are introduced.
Phase IV: Return to High-Impact Function (Months 3-6+)
The final phase of rehabilitation focuses on plyometrics, sport-specific agility drills, and the restoration of explosive plantar flexion power. Return to high-impact sports, running, or heavy manual labor is typically delayed until 4 to 6 months postoperatively. Clearance for these activities is strictly contingent upon the recovery of symmetrical calf strength (assessed via single-leg heel raise endurance), full pain-free range of motion, and the complete absence of localized insertional pain.
Preoperative counseling regarding this timeline is an absolute imperative. The surgeon must explicitly manage the expectations of the patient, particularly young women presenting with a classic "pump bump." It must be clearly articulated that it may take a minimum of 3 to 6 months before they can even attempt to wear a stylish, closed-heel shoe. Furthermore, the surgeon must explicitly state that there is no physiological guarantee they will ever be able to wear rigid-heeled footwear comfortably again. Setting these firm expectations preoperatively prevents profound postoperative dissatisfaction, even in the setting of a technically flawless and biologically successful surgery.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of Haglund deformity and insertional Achilles tendinopathy is heavily guided by a robust body of orthopedic literature that has evolved significantly over the past three decades. Understanding these landmark studies is essential for the academic surgeon to justify their surgical algorithm and predict patient outcomes accurately.
The critical distinction
