Surgical Management of Haglund Deformity, Retrocalcaneal Bursitis, and Achilles Tendinosis
Key Takeaway
Haglund deformity, often presenting with retrocalcaneal bursitis and insertional Achilles tendinosis, requires meticulous surgical intervention when conservative measures fail. Operative management typically involves a calcaneal osteotomy to resect the posterosuperior prominence. In cases of severe chronic tendinosis with significant tendon compromise, an adjunctive flexor hallucis longus (FHL) transfer is indicated to restore plantar flexion strength and provide vascularized tissue to the deficient Achilles insertion.
PATHOPHYSIOLOGY AND CLINICAL PRESENTATION
Haglund deformity, colloquially referred to as a "pump bump," represents a prominent posterosuperior calcaneal tuberosity that leads to mechanical impingement against the anterior aspect of the Achilles tendon. This osseous prominence, combined with repetitive ankle dorsiflexion, creates a pathologic triad known as Haglund syndrome: insertional Achilles tendinopathy, retrocalcaneal bursitis, and the physical Haglund deformity itself.
The retrocalcaneal bursa, situated between the anterior Achilles tendon and the bare area of the posterosuperior calcaneus, becomes inflamed and hypertrophic due to chronic friction. Over time, this mechanical attrition leads to intrasubstance degeneration of the Achilles tendon, mucoid degeneration, and the formation of intratendinous calcifications or osteophytes at the tendon insertion.
Patients typically present with posterior heel pain that is exacerbated by walking, running, or wearing rigid-heeled footwear. Clinical examination often reveals a palpable, tender prominence at the posterolateral aspect of the heel, accompanied by localized erythema and swelling.
INDICATIONS FOR SURGERY AND PREOPERATIVE COUNSELING
Surgical intervention is indicated only after a rigorous trial of conservative management has failed. Nonoperative modalities should include activity modification, nonsteroidal anti-inflammatory drugs (NSAIDs), heel lifts, open-backed footwear, physical therapy focusing on eccentric stretching, and occasionally, immobilization in a controlled ankle motion (CAM) boot. Corticosteroid injections within the retrocalcaneal bursa are highly controversial and generally discouraged due to the significant risk of iatrogenic Achilles tendon rupture.
When conservative measures fail, surgical resection of the Haglund prominence (calcaneal osteotomy or exostectomy) and debridement of the retrocalcaneal bursa and diseased Achilles tendon are indicated.
⚠️ Surgical Warning: Managing Patient Expectations
Preoperative counseling is arguably the most critical step in the management of Haglund deformity. Brunner et al. reported that 6 out of 36 patients (16.6%) who underwent calcaneal osteotomy were dissatisfied with their outcomes, primarily due to the unexpectedly prolonged recovery time.
Surgeons must explicitly warn patients—particularly young women seeking to return to wearing stylish or rigid-heeled shoes—that the recovery period is lengthy, typically ranging between 6 months and 2 years. Patients must be informed that it may take 3 to 6 months before they can comfortably wear standard footwear, and there is no absolute guarantee that they will ever be able to wear rigid, stylish shoes without some degree of discomfort.
SURGICAL ANATOMY AND BIOMECHANICS
Understanding the footprint of the Achilles tendon is paramount to successful surgical execution. The Achilles tendon inserts into the middle third of the posterior calcaneal tuberosity. The insertion is crescent-shaped, being wider distally and medially. The superior third of the posterior calcaneus is devoid of tendinous attachments; this bare area is covered by the retrocalcaneal bursa.
During a calcaneal osteotomy, the goal is to resect the superior bare area (the Haglund prominence) without compromising the structural integrity of the Achilles insertion. However, because the Achilles tendon has an extensive insertion extending into the posterior and plantar aspects of the tuberosity, adequate resection of the bone often necessitates elevating a 1- to 2-cm long portion of the tendon.
CALCANEAL OSTEOTOMY FOR HAGLUND DEFORMITY
The primary surgical objective is to decompress the retrocalcaneal space by excising the inflamed bursa, resecting the posterosuperior calcaneal prominence, and debriding any calcified or necrotic portions of the Achilles tendon.
Positioning and Anesthesia
- Anesthesia: The procedure is performed under general anesthesia or regional anesthesia (spinal or popliteal block).
- Positioning: Place the patient in the prone position. Ensure all bony prominences are well-padded.
- Tourniquet: Apply a well-padded pneumatic tourniquet to the proximal thigh to ensure a bloodless surgical field.
Surgical Approach
- Incision: Make a longitudinal lateral incision approximately 1 cm lateral to the lateral border of the Achilles tendon. The incision should extend distally from 3 to 4 cm proximal to the superior tuberosity of the calcaneus, down to 2 to 3 cm distal to the superior tuberosity.
- Superficial Dissection: Deepen the incision through the subcutaneous tissues. Take meticulous care to identify and protect the sural nerve, which crosses the lateral border of the Achilles tendon approximately 10 cm proximal to its insertion and courses distally along the lateral hindfoot.
- Tendon Exposure: Plantar flex the ankle joint to relieve tension on the Achilles tendon. By a combination of sharp and blunt dissection, identify the lateral border of the Achilles tendon and the retrocalcaneal space.
Resection of the Haglund Prominence
- Retraction: Place a right-angle retractor between the anterior aspect of the Achilles tendon and the posterior/superior borders of the calcaneal tuberosity. With the foot held in plantar flexion, this maneuver usually affords sufficient exposure to access the superior border of the calcaneal tuberosity.
- Tendon Elevation: While the goal is to leave the Achilles insertion undisturbed, the extensive footprint often dictates that raising a 1- to 2-cm long portion of the tendon from the posterior and plantar aspect of the tuberosity is necessary to achieve an adequate bony resection.
- Osteotomy: Remove the superior aspect of the tuberosity (the Haglund lesion) using a microsagittal saw or a sharp osteotome.
- Clinical Pearl: Placing several drill holes along the proposed osteotomy site from lateral to medial significantly facilitates this resection and prevents inadvertent propagation of the osteotomy into the posterior facet of the subtalar joint.
- The cut should be angled from posterosuperior to anteroinferior, effectively removing the entire prominence that impinges on the tendon during dorsiflexion.
- Tendon Debridement: Inspect the anterior aspect of the Achilles tendon. If an area of intratendinous ossification or severe tendinosis remains, split the Achilles tendon longitudinally in a coronal plane. Elevate the anterior third or half of the tendon distally to free up enough tissue to completely excise the calcified and necrotic tendon.
ADJUNCTIVE FLEXOR HALLUCIS LONGUS (FHL) TRANSFER
In cases of chronic, severe insertional or noninsertional Achilles tendinosis associated with Haglund deformity, extensive debridement may leave the Achilles tendon critically deficient. If more than 50% of the tendon insertion is resected, or if the tendon is severely degenerated, augmentation is required to prevent postoperative rupture and restore plantar flexion power.
The Flexor Hallucis Longus (FHL) tendon is the gold standard for Achilles augmentation. It is an in-phase synergist, possesses a strong axis of pull, and its low-lying, highly vascularized muscle belly provides excellent blood supply to the relatively avascular Achilles region, promoting healing.
FHL Transfer Technique
🔪 Surgical Technique: FHL Harvest and Transfer
Step 1: Exposure of the Defect
Following the resection of the Haglund prominence and aggressive debridement of the diseased Achilles tendon, assess the remaining defect. In chronic cases, a massive void is often present.
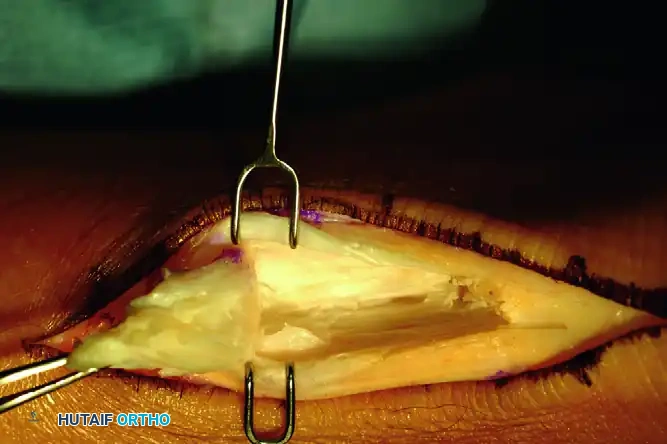
FIGURE A: Exposure of the involved portion of the tendon, demonstrating the extensive defect following debridement of chronic tendinosis.
Step 2: Identification and Harvest of the FHL
The FHL can be harvested through the same posterior incision. Deepen the dissection medially, anterior to the Achilles tendon and posterior to the deep posterior compartment fascia.
1. Identify the FHL muscle belly, which is the most posterior and lateral structure in the deep posterior compartment.
2. Trace the FHL tendon distally as it enters the fibro-osseous tunnel beneath the sustentaculum tali.
3. Harvest the tendon as distally as possible. While a double-incision technique (adding a medial midfoot incision) can yield a longer graft, a single posterior incision usually provides sufficient length to bridge the Achilles defect and anchor into the calcaneus.

FIGURE B: Harvest and mobilization of the flexor hallucis longus (FHL) tendon. Note the robust, low-lying muscle belly.
Step 3: Fixation and Muscle Belly Interposition
1. Drill a bone tunnel or use a biotenodesis screw system in the superior aspect of the calcaneus, just anterior to the remaining Achilles footprint.
2. Tension the FHL tendon into the calcaneal tunnel with the ankle held in 15 to 20 degrees of plantar flexion to match the resting tension of the Achilles.
3. Suture the robust FHL muscle belly directly into the Achilles tendon defect. This step is critical, as the vascular muscle belly provides a rich blood supply to the avascular zone of the Achilles, significantly enhancing biologic healing.

FIGURE C: The flexor hallucis longus muscle belly is meticulously sutured into the Achilles tendon defect, providing both biomechanical augmentation and vascular enhancement.
CLOSURE AND POSTOPERATIVE CARE
Wound Closure
Meticulous hemostasis is mandatory to prevent postoperative hematoma, which can compromise wound healing in this high-risk area.
1. Copiously lavage the wound with sterile saline to remove all bone debris from the osteotomy.
2. If the Achilles tendon was split or partially detached, repair it using heavy nonabsorbable sutures (e.g., #2 FiberWire) using a Krackow or similar locking stitch. Use suture anchors if reattachment to the calcaneus is required.
3. Close the paratenon (if viable), subcutaneous tissues, and skin in layered fashion. A closed-suction drain may be placed at the surgeon's discretion.
Postoperative Protocol
The postoperative rehabilitation protocol must balance the need for tissue healing with the prevention of debilitating stiffness.
Phase 1: Immobilization (Weeks 0–3)
* Immediately postoperatively, apply a well-padded, short-leg, non–weight-bearing (NWB) cast with the ankle immobilized in approximately 20 degrees of plantar flexion. This position minimizes tension on the Achilles repair and the FHL transfer.
* Strict elevation is required to manage edema and protect the posterior skin incision.
Phase 2: Transition and Early ROM (Weeks 3–6)
* At 3 weeks, the cast and skin sutures are removed. (Sutures may be removed earlier if clinically indicated, but the NWB cast must remain in place for the full 3 weeks).
* Transition the patient to a removable controlled ankle motion (CAM) weight-bearing cast boot, fitted with heel wedges to maintain slight plantar flexion.
* Initiate active plantar flexion and gentle active dorsiflexion exercises to neutral. Passive dorsiflexion stretching is strictly prohibited at this stage to protect the tendon insertion.
* Weight-bearing is gradually progressed in the boot as tolerated.
Phase 3: Strengthening and Normalization (Weeks 6–12)
* Gradually remove the heel wedges from the CAM boot over a period of 2 to 3 weeks to slowly stretch the Achilles complex.
* Transition to regular footwear with a slight heel lift.
* Begin formal physical therapy focusing on isometric strengthening, progressing to concentric, and eventually eccentric loading of the gastroc-soleus complex.
Phase 4: Return to Activity (Months 3–6+)
* Proprioceptive training and sport-specific activities are introduced.
* As emphasized during preoperative counseling, patients must be reminded that complete resolution of swelling and the ability to wear rigid or stylish shoes comfortably may take up to 6 months, and maximal medical improvement may not be reached until 1 to 2 years postoperatively.
COMPLICATIONS AND PITFALLS
- Wound Dehiscence and Infection: The posterior heel has tenuous vascularity. Excessive retraction, overly tight skin closure, or early mobilization can lead to skin necrosis and deep infection. Meticulous soft tissue handling is non-negotiable.
- Inadequate Bone Resection: Failure to remove enough of the posterosuperior prominence will result in persistent impingement and recurrent symptoms. Pre-drilling the osteotomy helps ensure an aggressive, yet safe, resection angle.
- Achilles Tendon Avulsion/Rupture: Over-resection of the calcaneus that violates the Achilles footprint, or failure to augment a severely degenerated tendon (>50% debrided), can lead to catastrophic postoperative rupture. Always have a low threshold to perform an FHL transfer if the tendon integrity is questionable.
- Sural Nerve Injury: Iatrogenic injury to the sural nerve during the lateral approach results in painful neuromas and lateral foot numbness. Careful blunt dissection in the subcutaneous tissues is required.
You Might Also Like

