Comprehensive Introduction and Patho-Epidemiology
The reconstruction of complex soft tissue defects remains a foundational pillar of operative orthopaedics, serving as the critical interface between skeletal stability and functional limb restoration. Whether managing high-energy acute trauma, executing post-oncologic resections, or salvaging chronic wounds complicated by osteomyelitis, the orthopaedic surgeon must possess a masterful, nuanced understanding of soft tissue management. The traditional paradigm of the "reconstructive ladder"—progressing linearly from secondary intention and primary closure to the sophisticated application of free skin grafts, local flaps, and distant pedicled or free tissue transfers—has evolved. Contemporary orthopaedic microsurgery now advocates for the "reconstructive elevator," wherein the optimal reconstructive modality is selected immediately based on the specific anatomical and biomechanical requirements of the defect, bypassing intermediate, potentially morbid steps.
The fundamental axiom of skin grafting dictates a critical biological and biomechanical trade-off: “The thinner the graft, the better the take; however, the thicker the graft, the better the function.” A thick graft, incorporating a substantial portion of the reticular dermis, is biomechanically superior. It withstands shear friction, accommodates constant functional use, and contracts only about 10% during the maturation phase. Conversely, a thin graft, while possessing a higher metabolic tolerance during the initial ischemic phase and thus a higher probability of initial survival, may undergo profound secondary contraction of 50% to 75%, potentially leading to severe joint contractures if applied across flexor creases.
For any free graft to survive, it must rapidly reestablish its nutritional supply before full-thickness cellular death ensues. This intricate physiological process occurs in three distinct, overlapping phases. The first phase, Plasmatic Imbibition (Days 1-2), is characterized by the graft absorbing wound exudate; the graft swells and survives purely via passive diffusion of nutrients and oxygen from the recipient bed. The second phase, Inosculation (Days 3-4), involves the precise alignment and connection of the graft's severed capillary network with the proliferating vessels of the recipient bed. The final phase, Neovascularization (Days 5 and beyond), is defined by the active ingrowth of new blood vessels into the graft dermis, establishing a definitive blood supply.
A graft cannot survive if a hematoma, seroma, or sheer force physically separates it from the underlying vascular bed, as this disrupts the fragile process of inosculation. Furthermore, grafts will categorically fail if applied to avascular beds; they will generally not survive on bare cortical bone devoid of periosteum, bare tendon devoid of paratenon, or bare cartilage devoid of perichondrium. In these scenarios, the orthopaedic surgeon must pivot to the utilization of vascularized tissue transfers, such as local or free flaps, to import a robust, independent blood supply to the compromised recipient site.
Detailed Surgical Anatomy and Biomechanics
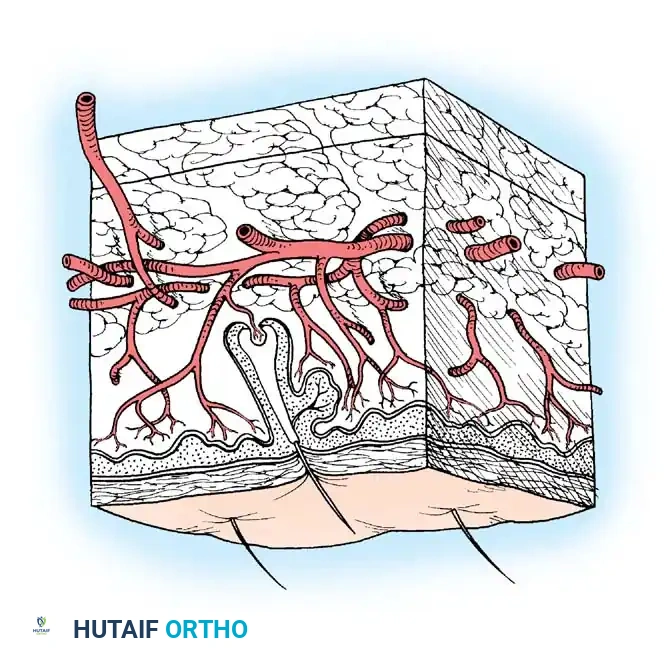
A profound comprehension of cutaneous anatomy and its inherent biomechanical properties is non-negotiable for the reconstructive orthopaedic surgeon. The skin is a complex, bilaminar organ consisting of the superficial epidermis and the deeper dermis, supported by the underlying subcutaneous adipose tissue. The epidermis is an avascular, stratified squamous epithelium comprising five distinct layers (stratum corneum, lucidum, granulosum, spinosum, and basale), relying entirely on diffusion from the underlying dermal capillary beds. The dermis, which provides the structural integrity and elasticity of the skin, is divided into the superficial papillary dermis (rich in capillary loops and nerve endings) and the deeper reticular dermis (composed of dense, interlacing collagen and elastin fibers).
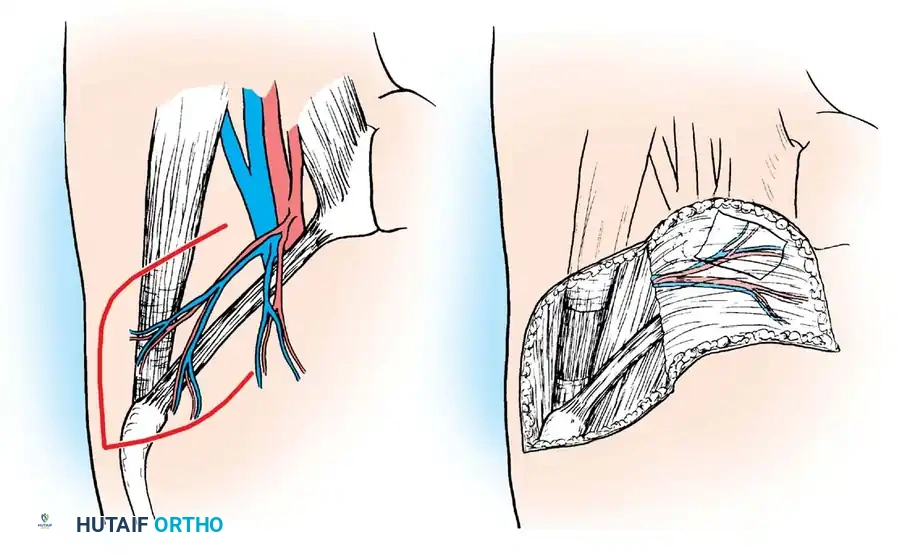
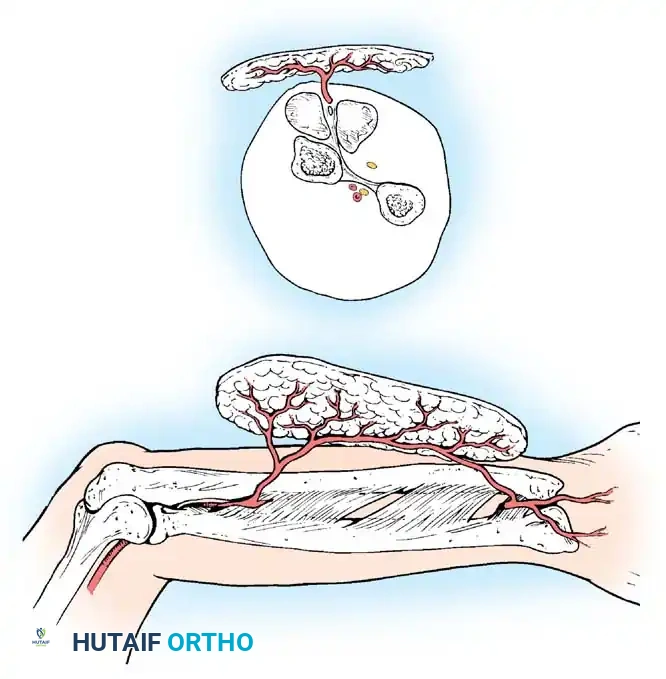
The vascular supply to the skin is orchestrated through a sophisticated, tiered network of plexuses. Perforating vessels derived from underlying source arteries traverse the muscle and fascia (musculocutaneous perforators) or travel within the intermuscular septa (septocutaneous perforators). These vessels feed the deep subdermal plexus, which in turn supplies the dermal plexus and ultimately the superficial subpapillary plexus. When harvesting a full-thickness skin graft (FTSG), the subdermal plexus is severed, necessitating complete defatting to allow the dermal plexus to directly interface with the recipient bed. In contrast, skin flaps are harvested with their subdermal plexus intact, maintaining intrinsic vascularity either through a random pattern (relying on the diffuse subdermal network) or an axial pattern (incorporating a named, anatomically consistent blood vessel).
Biomechanically, skin exhibits profound viscoelastic properties, primarily characterized by creep and stress relaxation. Creep refers to the progressive extension of skin over time when subjected to a constant load, a principle heavily utilized in tissue expansion and serial tensioning devices. Stress relaxation occurs when skin is stretched to a given length and held; the force required to maintain that stretch decreases over time as the collagen fibers realign and interstitial fluid is displaced. These properties are critical when planning local flaps, as they allow the surgeon to mobilize adjacent tissue under controlled tension without precipitating ischemic necrosis at the flap margins.
Furthermore, the orientation of collagen fibers dictates the skin's lines of maximal tension, known as Langer's lines. Surgical incisions and flap designs should ideally parallel these lines to minimize tension on the closure, thereby optimizing wound healing and mitigating hypertrophic scar formation. When planning local transposition or rotation flaps, the orthopaedic surgeon must meticulously calculate the pivot point and the arc of rotation, ensuring that the vascular pedicle is not subjected to excessive torsion or tension, which would catastrophically compromise the microcirculation and lead to flap failure.
Exhaustive Indications and Contraindications
The decision matrix for selecting the appropriate soft tissue coverage modality requires a comprehensive evaluation of the defect's size, depth, location, and the physiological status of the recipient bed. Split-thickness skin grafts (STSGs) are the workhorse for broad, shallow defects exhibiting robust granulation tissue or healthy, vascularized muscle/fascia. They are particularly indicated in massive trauma, extensive burns, and large fasciotomy wound closures where primary approximation is impossible. Because they require less revascularization energy, STSGs are preferred in beds with marginal vascularity, though they are contraindicated over bare bone, tendon, or hardware.
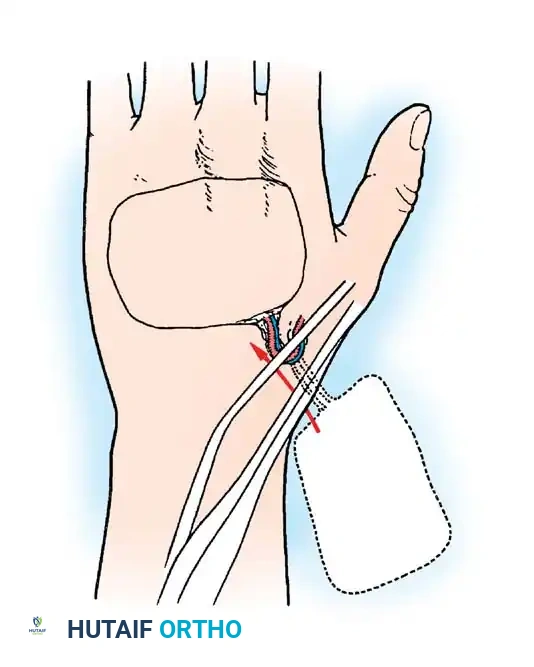
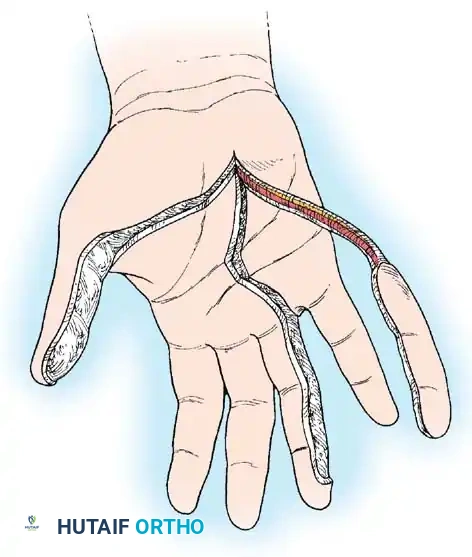
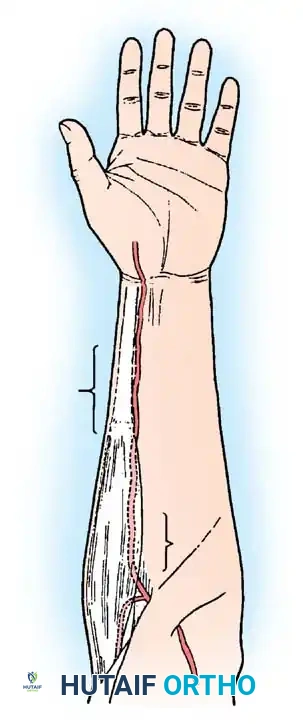
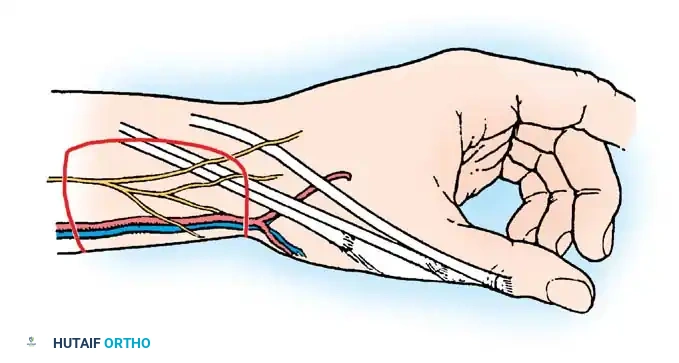
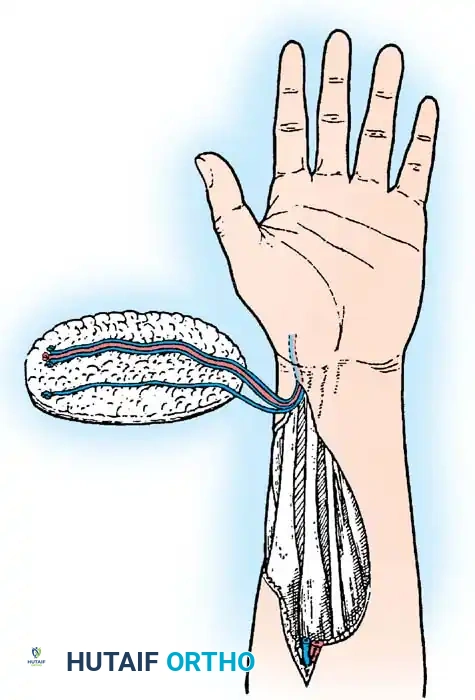
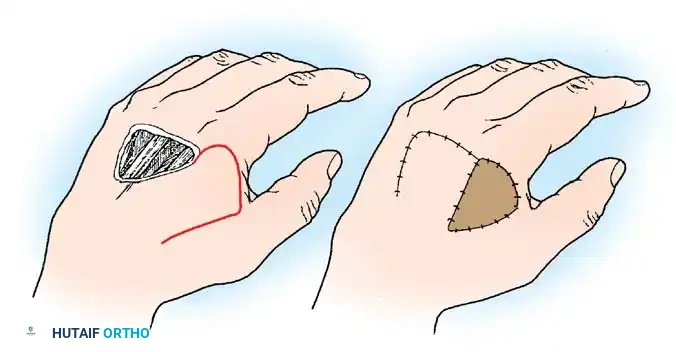
Full-thickness skin grafts (FTSGs) are indicated for smaller, highly visible, or functionally demanding areas where secondary contraction must be minimized and durability maximized. In orthopaedic surgery, FTSGs are predominantly utilized in the hand and digits, particularly for palmar defects, syndactyly releases, and fingertip amputations where a sensate, durable, and pliable surface is paramount. However, FTSGs demand a pristine, highly vascularized recipient bed; thus, they are relatively contraindicated in acute, contaminated trauma or over irradiated tissue where the microcirculation is inherently compromised.
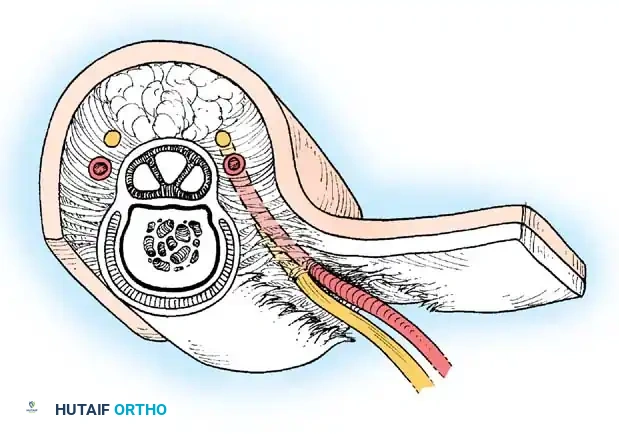
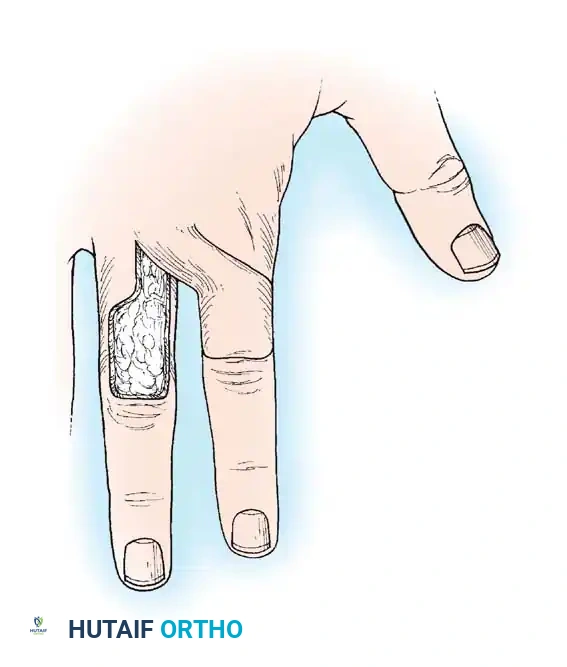
Local skin flaps are unequivocally indicated when the defect exposes structures that cannot support a free graft—namely, bare cortical bone, joints, nerves, tendons without paratenon, and orthopaedic implants. Flaps provide a robust layer of subcutaneous tissue, restoring contour, providing a durable gliding surface, and importing an independent blood supply. This is crucial for managing osteomyelitis or facilitating the healing of underlying fractures. Contraindications to local flaps include extensive zone of injury (where the adjacent tissue is traumatized and its vascularity unreliable), severe peripheral vascular disease, and active, uncontrolled infection at the operative site.
| Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| STSG | Large surface area defects, fasciotomy closures, burns, highly exuding wounds (meshed). | Bare bone, bare tendon, bare cartilage, exposed hardware, >10^5 CFU/g bacterial load. | Joint creases (due to contracture risk), highly irradiated tissue, severe malnutrition. |
| FTSG | Palmar hand defects, fingertip amputations, syndactyly release, facial reconstruction. | Contaminated acute wounds, avascular recipient beds, large defects (>5-7 cm). | Smokers (high risk of failure), areas requiring high shear resistance immediately. |
| Local Flap | Exposed bone/tendon/hardware, small to medium defects, need for gliding surface. | Traumatized adjacent tissue (zone of injury), inadequate local vascularity. | Patient non-compliance with immobilization, severe systemic comorbidities. |
| Free Flap | Massive defects, composite tissue loss (bone/skin), distal third tibia/foot defects. | Lack of recipient vessels, severe cardiopulmonary instability. | Advanced age (case-by-case), hypercoagulable states, profound peripheral arterial disease. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful soft tissue reconstruction. The orthopaedic surgeon must first aggressively optimize the patient's systemic physiology, correcting malnutrition (albumin > 3.0 g/dL), optimizing glycemic control (HbA1c < 7.0%), and mandating smoking cessation, as nicotine acts as a potent vasoconstrictor and significantly impairs microcirculatory flow, drastically increasing the risk of graft or flap necrosis. The recipient site must be critically evaluated; sepsis must be rigorously excluded. A quantitative wound biopsy yielding greater than $10^5$ colony-forming units (CFU) per gram of tissue, or the presence of any beta-hemolytic Streptococcus, is an absolute contraindication to grafting and necessitates further surgical debridement and targeted antimicrobial therapy.
Templating the defect is a critical step, particularly for FTSGs and local flaps. The surgeon should utilize sterile foil, a specialized surgical marker, or a piece of moistened Esmarch bandage to create an exact replica of the defect. For FTSGs, this template is transferred to the donor site, and the planned excision is marked slightly larger (approximately 10-15%) to accommodate for the primary, immediate elastic recoil of the harvested skin. For local flaps, the template is used to reverse-plan the flap's movement, ensuring that the arc of rotation or advancement distance is sufficient to achieve tension-free closure without compromising the pedicle. Handheld Doppler ultrasound is frequently employed to map out local perforating vessels, ensuring the flap design captures a reliable axial blood supply.
Patient positioning in the operating room must facilitate simultaneous, unhindered access to both the recipient defect and the chosen donor site. For extensive lower extremity trauma requiring large STSG coverage, the patient is typically positioned supine, allowing access to the anterior and lateral thighs. The donor site must be shaved, prepped, and draped widely. The use of a pneumatic tourniquet is highly recommended during the recipient bed preparation to ensure meticulous hemostasis and precise identification of viable tissue. However, the tourniquet must be deflated, and absolute hemostasis achieved via bipolar electrocautery or topical hemostatic agents prior to graft application, as an underlying hematoma is the most common cause of graft failure.
Equipment preparation is equally vital. The surgeon must verify the availability and functionality of dermatomes (e.g., Zimmer, Padgett, or Weck blades), ensuring the blades are newly opened and flawlessly sharp. Mineral oil or specialized skin lubricants must be available to facilitate smooth passage of the dermatome. If meshing is planned, the skin mesher must be pre-set to the desired expansion ratio (typically 1.5:1 for standard coverage, or up to 3:1 for massive burns), and the appropriate sterile carriers must be on the surgical field.
Step-by-Step Surgical Approach and Fixation Technique
Recipient Bed Preparation
The absolute prerequisite for successful grafting is a meticulously prepared, highly vascularized recipient bed. The sooner a graft can be applied to a clean bed, the better the functional outcome. It is a common misconception that one must wait for exuberant, "beefy red" granulation tissue to form; in fact, early coverage of healthy muscle or fascia yields superior results. If the bed is contaminated or contains necrotic debris, the surgeon must perform radical surgical excision, utilizing scalpel, curette, or hydrosurgery systems (e.g., Versajet) until punctate bleeding is observed from all surfaces. Negative pressure wound therapy (NPWT) is an invaluable adjunct in the interim, promoting angiogenesis, reducing tissue edema, and decreasing the bacterial bioburden prior to definitive coverage.
Split-Thickness Skin Graft Harvest and Application
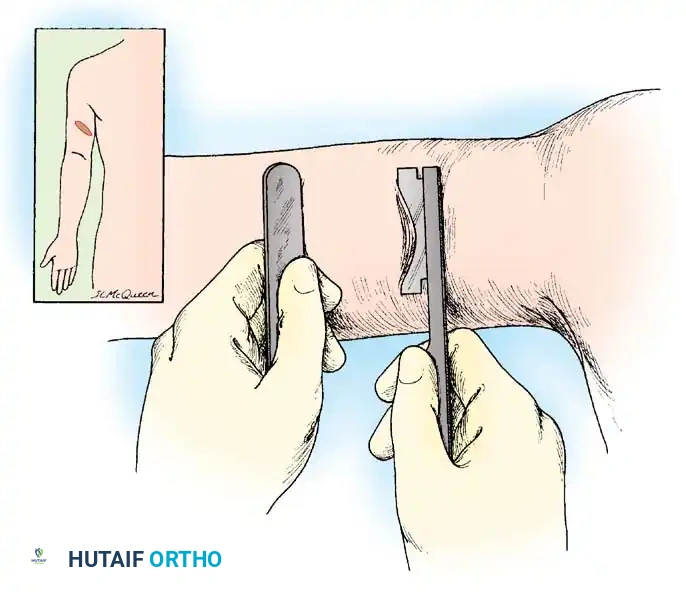
For standard STSGs, electrically or pneumatically powered dermatomes are the gold standard. The donor site (typically the anterolateral thigh) is lubricated with mineral oil. The surgeon applies firm, counter-traction using a sterile tongue depressor or board just ahead of the advancing dermatome. The dermatome is engaged, placed flat against the skin at a 45-degree angle, and advanced with steady, continuous downward and forward pressure. The thickness is typically set between 0.010 and 0.015 inches. Once the desired length is achieved, the dermatome is angled upward to sever the graft.
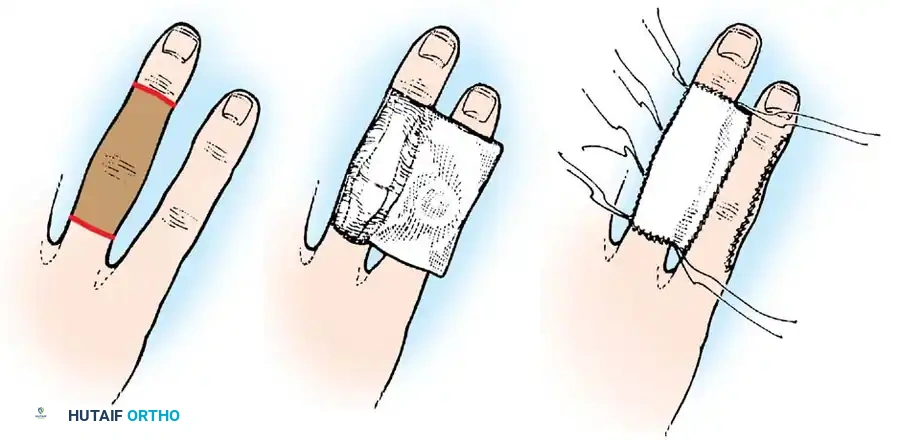
The harvested graft is immediately transferred to a saline-moistened sponge. Meshing the graft (1.5:1) is strongly advocated; it not only expands the surface area but critically creates fenestrations that allow for the egress of serum and blood, thereby preventing the catastrophic formation of a subgraft hematoma. The graft is then transferred to the recipient bed and carefully unrolled, ensuring the dermal (matte, pale) side is down and the epidermal (glossy) side is up. Fixation is achieved using surgical staples or fine non-absorbable sutures (e.g., 4-0 or 5-0 nylon) placed circumferentially. A tie-over stent dressing, utilizing a non-adherent contact layer (e.g., Xeroform) topped with fluffed gauze and secured by tying the peripheral sutures over the bolus, provides essential uniform compression and prevents devastating shear forces.
Full-Thickness Skin Graft Harvest and Application
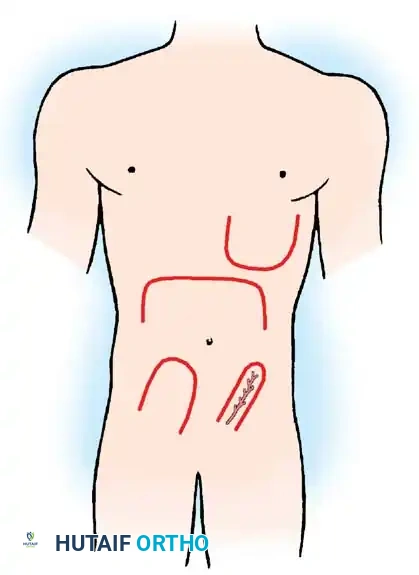
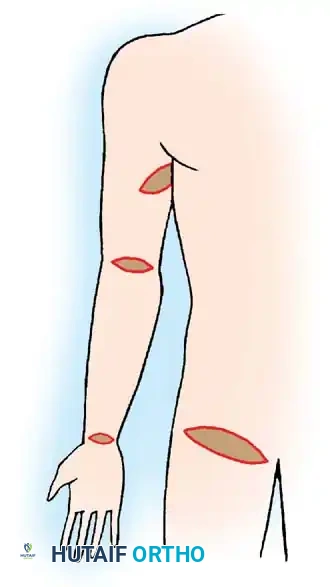
FTSG harvest requires an entirely different surgical technique. Following precise templating, the donor site (e.g., groin crease, hypothenar eminence) is infiltrated with local anesthetic containing epinephrine to facilitate hemostasis and hydrodissection. The marked ellipse is incised down to the subcutaneous fat using a #15 scalpel. The graft is elevated using fine skin hooks, and sharp dissection is utilized to separate the dermis from the underlying adipose tissue. The donor site is then widely undermined and closed primarily in layers.
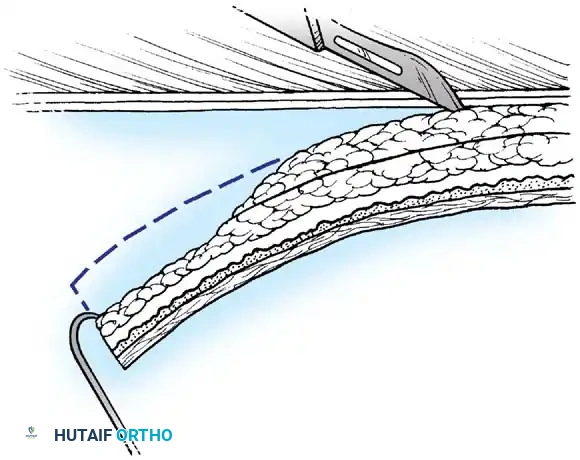
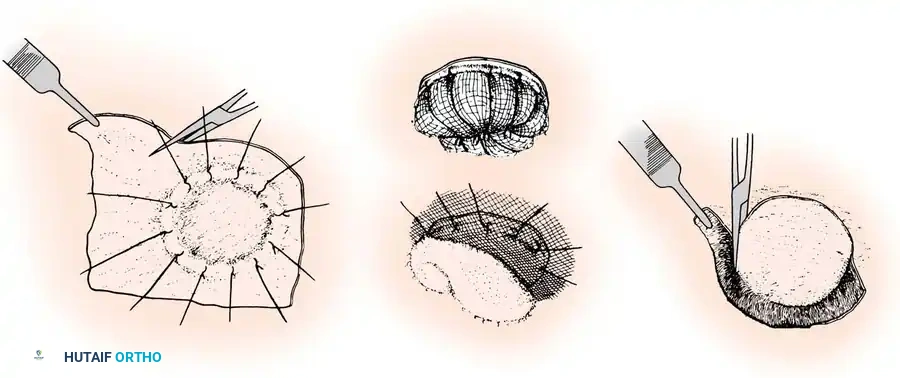
The most critical step in FTSG preparation is aggressive defatting. The surgeon drapes the graft, epidermal side down, over a sterile finger or a firm board. Using curved tenotomy or Iris scissors, every macroscopic lobule of yellow subcutaneous fat is painstakingly excised until the pure white, glistening undersurface of the reticular dermis is exposed. Failure to adequately defat the graft will result in a physical barrier to inosculation and guaranteed graft necrosis. The FTSG is then sutured into the recipient defect with exact edge-to-edge apposition, and a tie-over bolster dressing is universally applied to maintain intimate contact with the bed.
Local Flap Mobilization Techniques
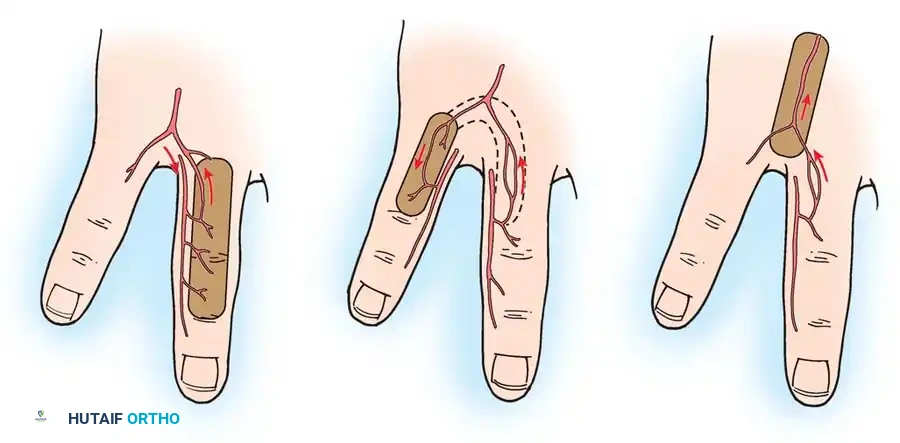
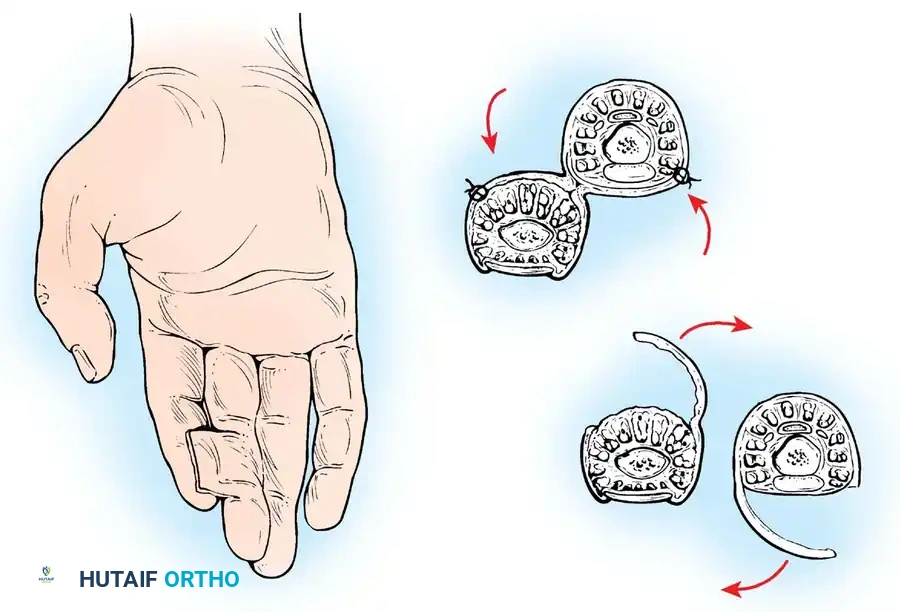
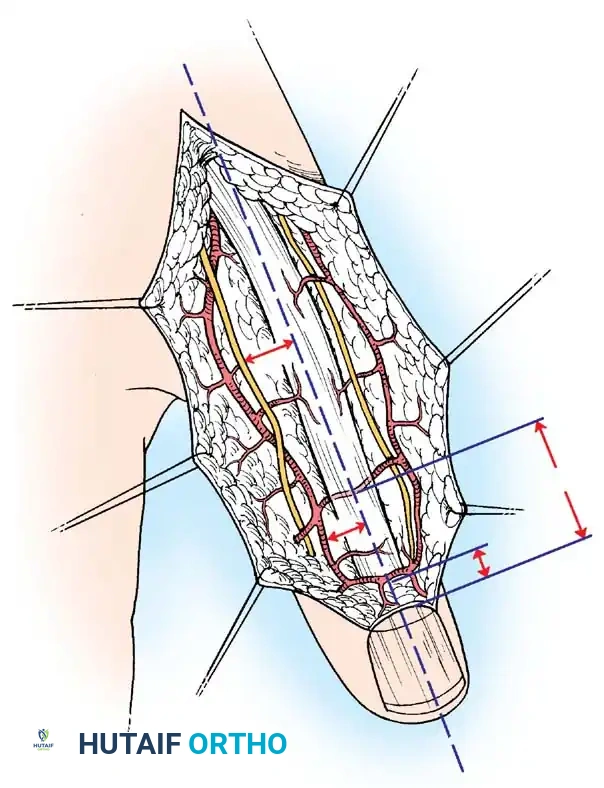
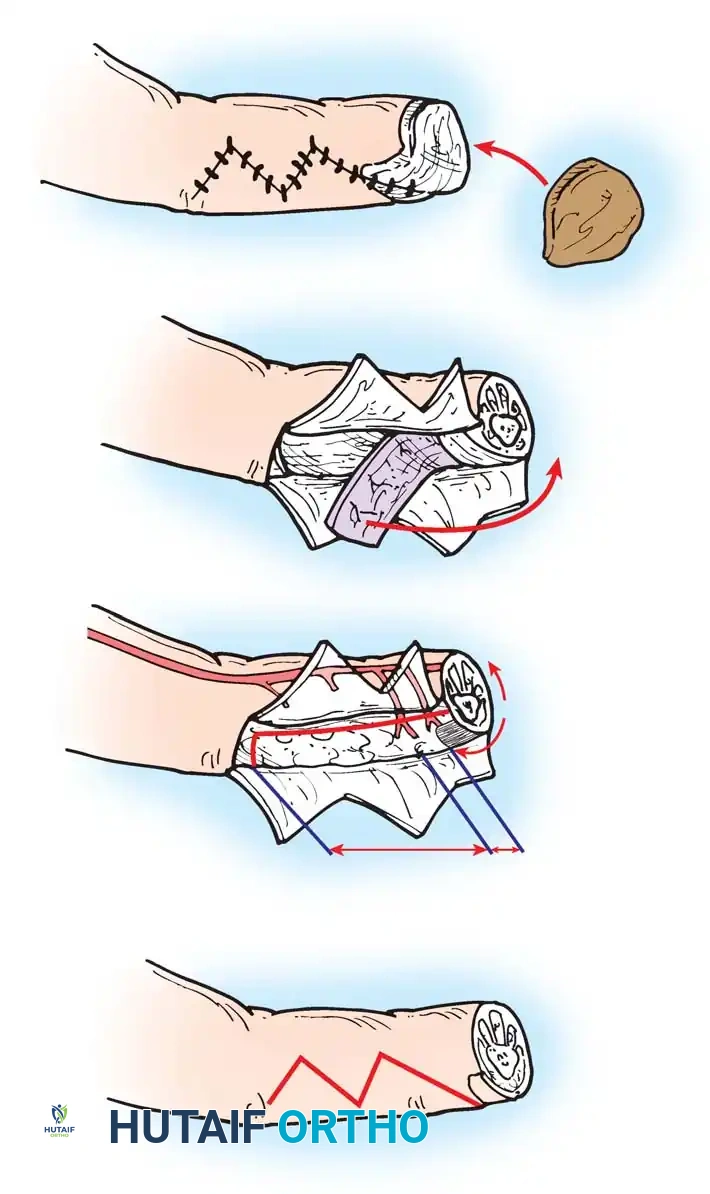
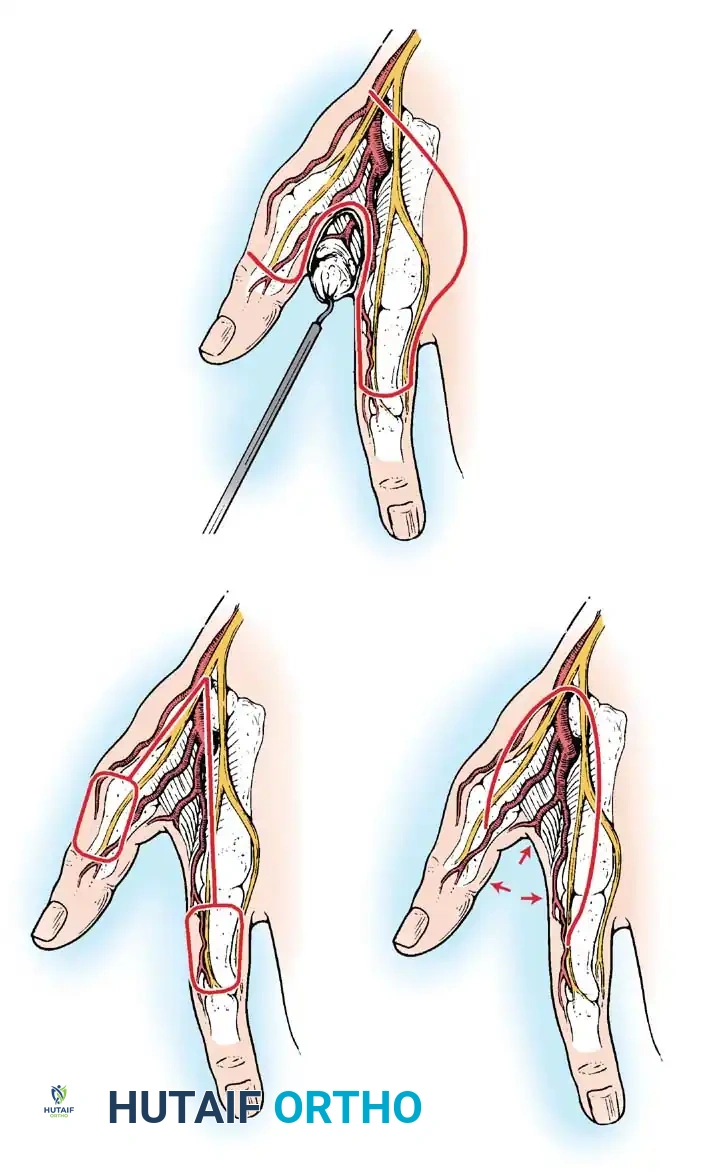
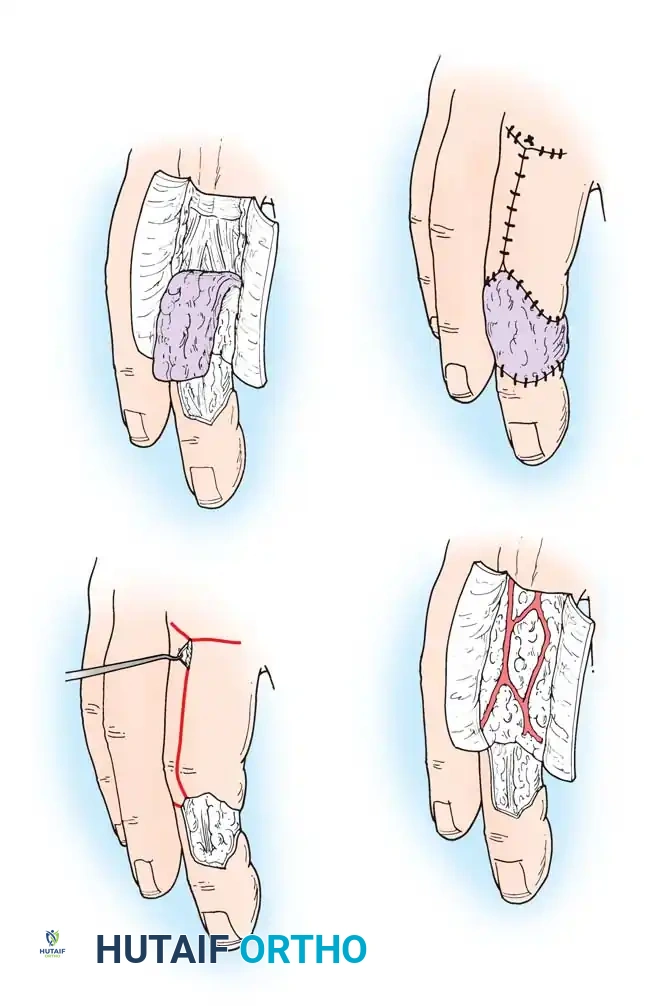
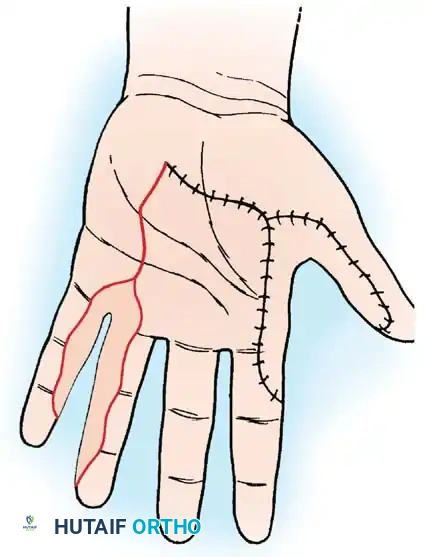
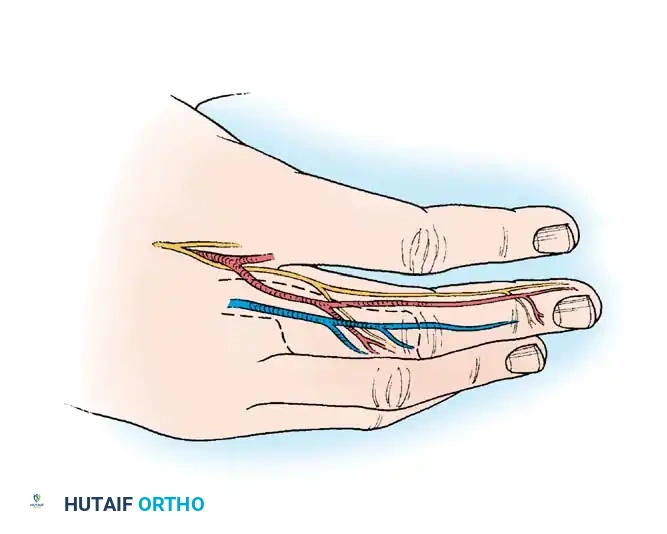
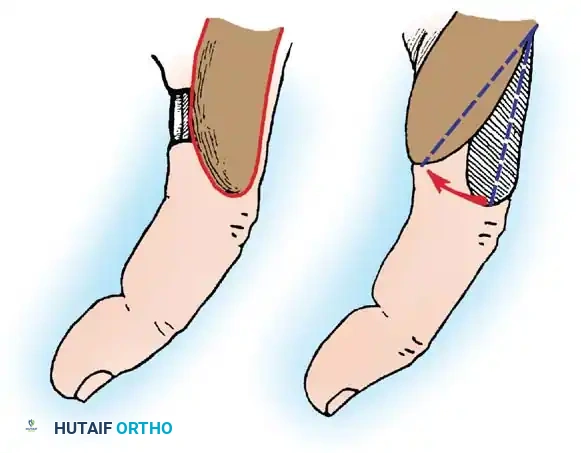
When a local flap is indicated, the surgeon must choose the appropriate geometry to mobilize tissue without compromising its vascularity. Advancement flaps (e.g., V-Y or rectangular advancement) are incised and stretched directly forward over the defect. The V-Y advancement flap is particularly useful for fingertip amputations; a V-shaped incision is made with the apex pointing proximally, the subcutaneous tissue is aggressively mobilized while preserving the neurovascular bundles, and the skin is advanced distally, with the secondary defect closed in a Y-configuration.
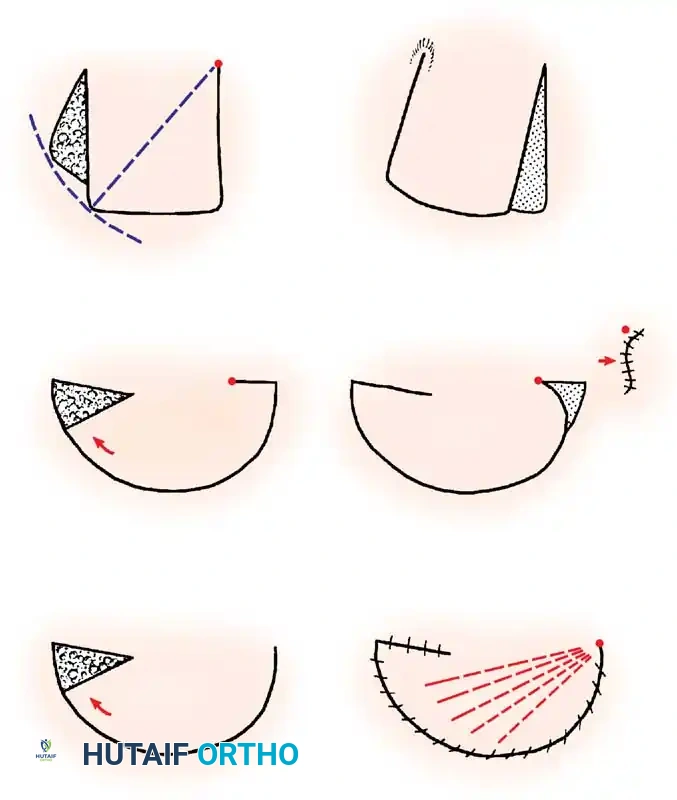
Rotation flaps are semicircular flaps rotated about a pivot point into the defect. The radius of the flap must be significantly larger than the defect to minimize tension. A back-cut or a Burow's triangle excision at the base may be required to facilitate rotation and eliminate dog-ears, though the surgeon must be acutely aware that a back-cut narrows the pedicle and reduces the blood supply.
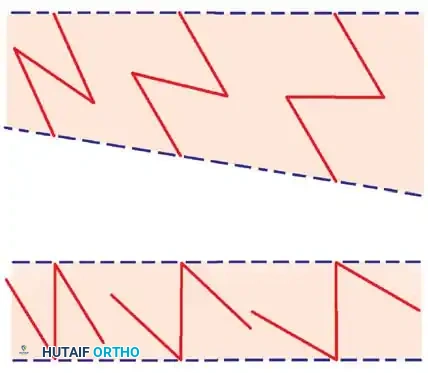
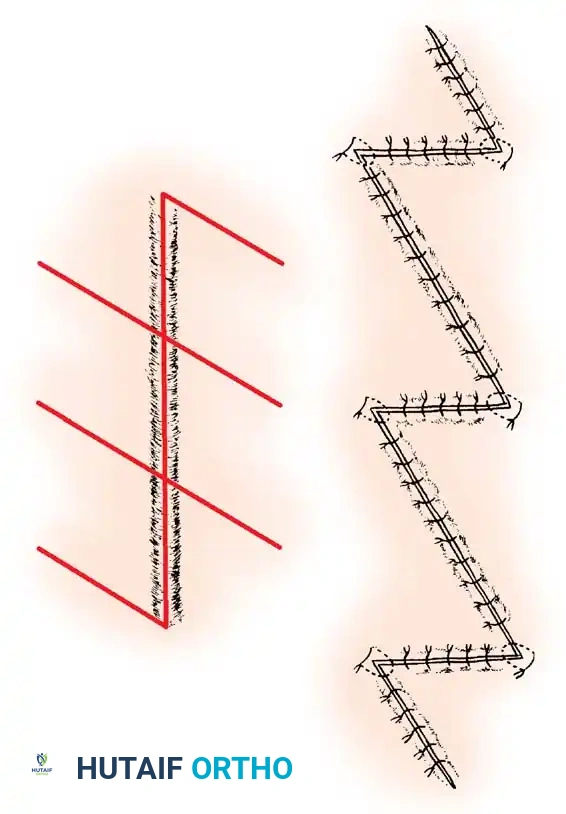
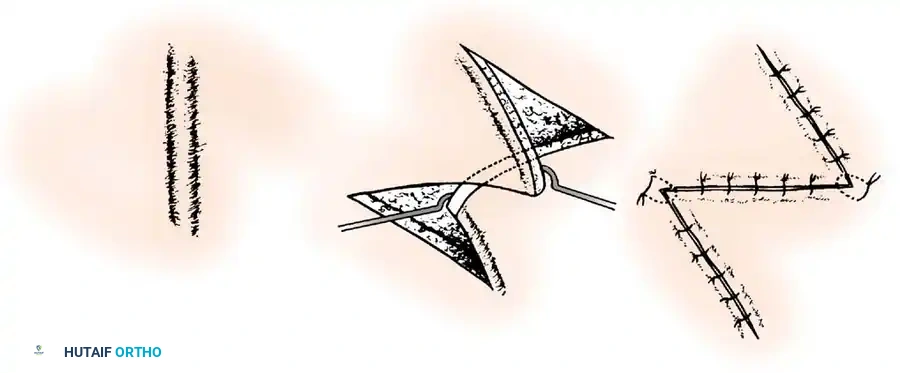
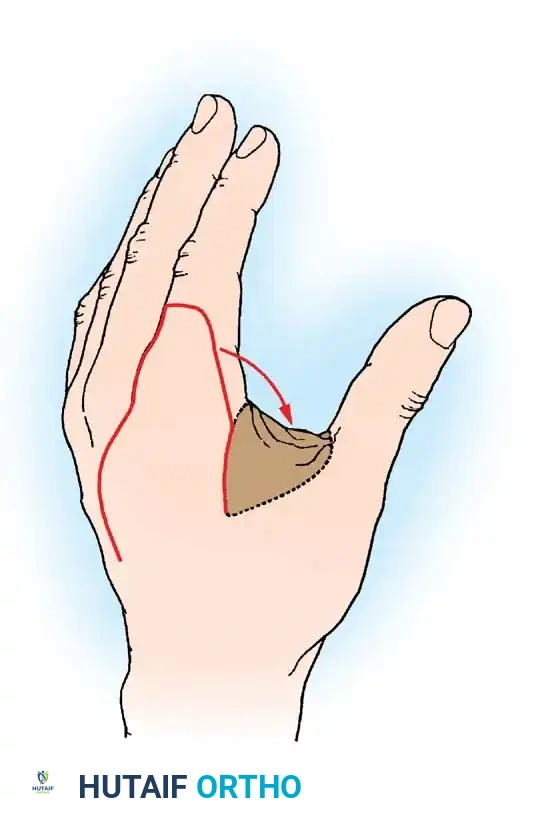
Transposition flaps, such as the Z-plasty or rhomboid (Limberg) flap, involve moving a paddle of tissue laterally across an intervening bridge of intact skin. The Z-plasty is a masterful orthopaedic technique used to lengthen a contracted scar or redirect tension lines. By creating two triangular flaps with equal limb lengths and specific angles (a 60-degree angle provides a theoretical 73% increase in length), the flaps are transposed, fundamentally altering the biomechanical vectors of the skin. The secondary defect created by larger transposition flaps inevitably requires coverage with an STSG.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, soft tissue reconstruction is fraught with potential complications that the orthopaedic surgeon must be prepared to rapidly diagnose and manage. The most frequent cause of graft failure is the accumulation of a hematoma or seroma beneath the graft, which physically prevents plasmatic imbibition and inosculation. The incidence of hematoma-induced failure ranges from 5% to 15%, heavily dependent on the adequacy of recipient bed hemostasis and the use of meshing. Shear forces are the second most common cause of failure, disrupting the fragile capillary connections during the critical days 3-5 post-op.

Flap complications are primarily vascular in nature. Venous congestion is far more common than arterial insufficiency and presents as a swollen, purplish-blue flap with brisk (less than 1 second) capillary refill and the bleeding of dark, deoxygenated blood upon pinprick. Arterial insufficiency, conversely, presents as a pale, cool flap with absent capillary refill. The incidence of partial or complete flap necrosis in local random pattern flaps can approach 10-20% if the length-to-width ratio exceeds 2:1 in the lower extremity. Infection remains a catastrophic complication for both grafts and flaps, rapidly destroying the microvascular network through thrombosis and enzymatic degradation.
Salvage management requires decisive action. If a subgraft hematoma is identified within the first 48 hours, it must be immediately evacuated by rolling a sterile swab over the graft or making a small incision to express the clot. If a flap exhibits severe venous congestion, immediate removal of tight sutures, application of medicinal leeches (Hirudo medicinalis), or systemic administration of rheologic agents (e.g., dextran, heparin) may salvage the tissue. If frank necrosis occurs, the dead tissue must be aggressively debrided once demarcated. The surgeon must then reassess the reconstructive ladder; a failed graft may require upgrading to a local flap, while a failed local flap may necessitate a free tissue transfer or application of NPWT to stimulate a new granulating bed.
| Complication | Estimated Incidence | Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Hematoma / Seroma | 5% - 15% | Fluctuant, dark mass under graft; loss of graft adherence. | Immediate evacuation (rolling or incision); re-apply compressive bolster. |
| Shear Disruption | 2% - 10% | Graft displacement, tearing, failure to vascularize by Day 5. | Strict immobilization; potentially requires re-grafting if full-thickness loss. |
| Venous Congestion (Flap) | 10% - 20% | Blue/purple discoloration, rapid cap refill, dark bleeding. | Suture removal, medicinal leeches, elevation, avoid compressive dressings. |
| Arterial Ischemia (Flap) | 1% - 5% | Pale, cool, empty capillary bed, no bleeding on pinprick. | Release tension, check pedicle geometry (kinking), surgical exploration. |
| Infection (Graft/Flap) | 2% - 8% | Erythema, purulent exudate, foul odor, graft lysis. | Rapid debridement, quantitative cultures, targeted IV antibiotics, NPWT. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following soft tissue reconstruction is as critical as the surgical execution itself. The protocol is rigidly phased to respect the biological timeline of graft take and flap revascularization. The Immobilization Phase (Days 0-7) is paramount. The reconstructed extremity must be strictly immobilized using rigid plaster or fiberglass splints to eliminate all shear forces across the recipient site. For upper extremity reconstructions, the hand is typically splinted in the intrinsic-plus (safe) position to prevent collateral ligament contracture. Elevation above the level of the heart is mandatory to minimize interstitial edema, which can compress the fragile microcirculation and precipitate venous congestion.