Introduction to Arthroscopic Surgery
During the past three decades, arthroscopy has dramatically changed the orthopaedic surgeon’s approach to the diagnosis and treatment of a variety of joint ailments. A high degree of clinical accuracy, combined with low morbidity, has encouraged the widespread use of arthroscopy to assist in diagnosis, determine prognosis, and provide definitive therapeutic intervention.
Clinical Pearl: Arthroscopic procedures must serve as adjuncts to—and not replacements for—thorough clinical evaluation. Arthroscopy is never a substitute for foundational clinical skills, rigorous history taking, and comprehensive physical examination.
Progressive improvements in the lens systems of arthroscopes, fiberoptic illumination, miniaturization of digital cameras, and the refinement of accessory operative instruments have made advanced operative arthroscopic techniques possible for virtually every joint in the body. This includes the knee, shoulder, hip, ankle, elbow, wrist, hand, and foot. Endoscopic techniques have even become standard in many spinal procedures. Although many arthroscopic procedures have proven superior to traditional open techniques, surgical outcomes should never be sacrificed merely to expand the indications for arthroscopic intervention.
Optical Systems and the Arthroscope
An arthroscope is fundamentally a highly specialized optical instrument. Three basic optical systems have historically been utilized in rigid arthroscopes:
1. The classic thin-lens system.
2. The rod-lens system (designed by Professor Harold Hopkins).
3. The graded index (GRIN) lens system.
Modern fiberoptic technology, the integration of magnifying lenses, and high-definition digital monitors have driven rapid advancements in arthroscope design. Contemporary arthroscopes offer an increased field of view with smaller outer diameters, superior depth of field, and optimized fluid flow through the surrounding sheath.
Optical Characteristics
Certain geometric and physical features determine the optical characteristics of an arthroscope. The most critical parameters are the diameter, angle of inclination, and field of view.
Angle of Inclination: This is the angle between the longitudinal axis of the arthroscope and a line perpendicular to the surface of the objective lens. It varies from 0 to 120 degrees. The 25- and 30-degree arthroscopes are the most commonly utilized in routine orthopaedic practice.
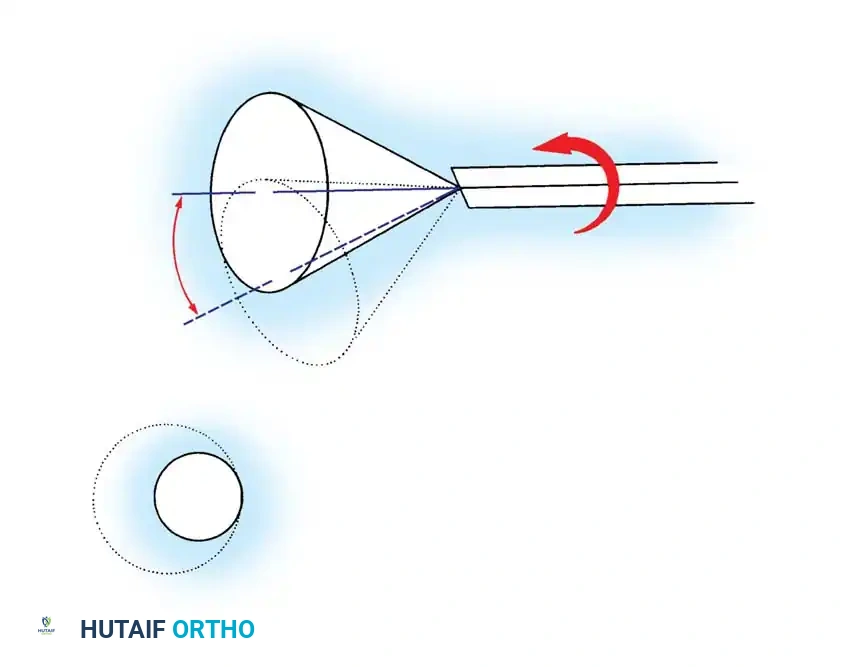
Rotation of the forward-oblique viewing (25- and 30-degree) arthroscopes allows a significantly larger area of the joint to be observed through a sweeping, scanning effect. The 70- and 90-degree arthroscopes are invaluable for visualizing "around corners," such as inspecting the posterior compartments of the knee through the intercondylar notch. However, these steeper angles have the distinct disadvantage of making spatial orientation significantly more difficult for the observer, often creating a central blind spot directly in front of the scope.
Field of View: This refers to the viewing angle encompassed by the lens. It varies according to the specific design and diameter of the arthroscope.
* A 1.9-mm scope typically provides a 65-degree field of view.
* A 2.7-mm scope provides a 90-degree field of view.
* A standard 4.0-mm scope provides a 115-degree field of view.
Wider viewing angles facilitate much easier anatomical orientation. Arthroscopes vary in diameter from 1.7 to 7 mm, with the 4.0-mm scope being the universal standard for large joints like the knee and shoulder. The smaller 1.9- and 2.7-mm scopes are reserved for tighter, smaller joints such as the wrist and ankle.
Illumination and Imaging Systems
Fiberoptic Light Sources
Initial light sources relied on 150-watt incandescent bulbs, which were adequate for direct visual observation but entirely insufficient for the demands of modern television and digital recording systems. To meet the high-intensity light requirements of video arthroscopy, tungsten, halogen, and xenon arc light sources producing 300 to 350 watts were developed.
The fiberoptic cable consists of a bundle of specially prepared glass fibers encased in a protective, flexible sheath. One end connects to the remote light source, while the other attaches to the arthroscope.
Surgical Warning: Glass fibers are highly fragile. Bending cables acutely, coiling them tightly, or placing heavy instruments on them will fracture the fibers, drastically reducing light transmission. Remember the rule of optical physics: approximately 8% of transmitted light is lost for every foot of cable length.
Modern systems increasingly utilize liquid (glycerin) light guides or advanced LED technology, which eliminate the problem of fiber breakage and provide a cooler, more consistent color temperature.
Television Cameras and Digital Imaging
The introduction of the television camera to the arthroscopy system revolutionized the field. It provided a more ergonomic operating position for the surgeon, prevented contamination of the sterile field by the surgeon’s face, and allowed the entire surgical team to participate in the procedure.
Modern solid-state cameras are compact, lightweight, and can be sterilized via gas, chemical soaking (e.g., Cidex), or autoclaving. Video-dedicated systems eliminate the traditional eyepiece, connecting the camera directly to the arthroscopic lens system. This direct connection mitigates the common issue of fogging—caused by moisture collecting between the arthroscope and the camera at the C-mount adapter. Three-chip camera technology and 4K digital signal processing now provide unprecedented color resolution, depth perception, and high-fidelity imaging.
Accessory Instruments
The basic arthroscopic instrument kit must be robust, versatile, and meticulously maintained. It typically includes 30-degree and 70-degree arthroscopes, probes, scissors, basket forceps, grasping forceps, arthroscopic knives, motorized shavers, and electrosurgical/radiofrequency devices.
The Probe
The probe is arguably the most critical diagnostic instrument after the arthroscope itself. It is universally recognized as "the extension of the arthroscopist’s finger."

The probe is essential for palpating intraarticular structures and planning the surgical approach. A refined tactile sensation allows the surgeon to differentiate normal from pathologic tissue. It is always better to "see and feel" rather than to "see" alone.
Indications for Probing:
* Assessing the consistency of articular cartilage (e.g., detecting early chondromalacia).
* Identifying and palpating occult meniscal tears.
* Maneuvering loose bodies into accessible grasping positions.
* Testing the tension of the anterior cruciate ligament (ACL).
* Retracting synovial tissue for enhanced exposure.
Most probes feature a right-angled tip measuring 3 to 4 mm in length. This known dimension serves as an intraoperative ruler to measure the size of osteochondral defects or meniscal tears.
Scissors and Basket Forceps
Arthroscopic scissors (3 to 4 mm in diameter) are available in straight, hooked, and curved configurations. Hooked scissors are generally preferred because their jaw geometry actively pulls tissue into the cutting edge, whereas straight scissors tend to push tissue away.
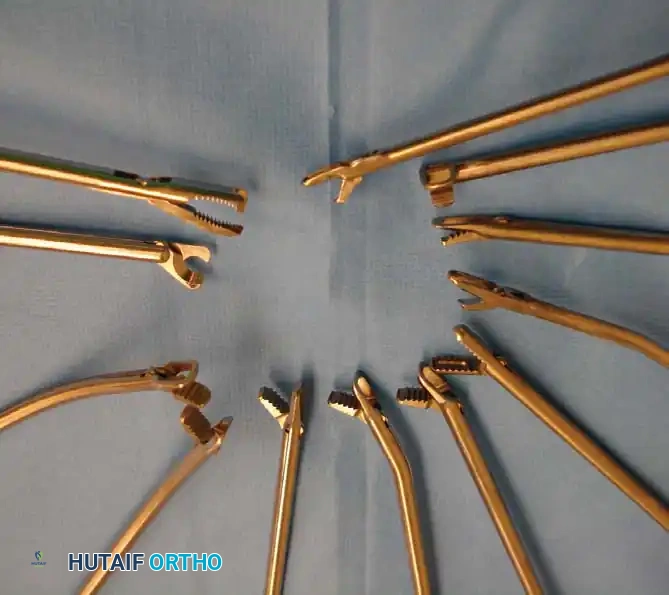
The basket forceps (punch biopsy forceps) is a workhorse in operative arthroscopy. The standard basket forceps features an open base, allowing each excised tissue fragment to drop free into the joint, where it is subsequently evacuated by fluid irrigation or suction. This eliminates the need to repeatedly remove the instrument from the joint for cleaning.
Baskets are available in an assortment of angles, including 30, 45, and 90 degrees, which are specifically designed to access difficult anatomical recesses, such as the anterior and posterior horns of the menisci. Wide, low-profile baskets are particularly excellent for precise meniscal contouring.
Motorized Shaving Systems
Motorized instrumentation is indispensable for efficient tissue resection, synovial debridement, and bony preparation.

These systems consist of a motorized handpiece connected to a central console that controls speed and direction (forward, reverse, and oscillate). The cutting attachments include various blades and burrs.

- Shaver Blades: Used primarily for soft tissue resection (synovectomy, meniscectomy, chondroplasty). They feature an outer stationary window and an inner rotating hollow blade connected to wall suction, which draws tissue into the window for precise amputation.
- Burrs: Used for aggressive bone resection, such as subacromial decompression, notchplasty in ACL reconstruction, or osteophyte removal.
Electrosurgical and Radiofrequency (RF) Instruments
Electrocautery and RF ablation devices are critical for achieving intraoperative hemostasis and performing controlled soft-tissue ablation. Bipolar RF wands operate by creating a localized plasma field that dissolves tissue at relatively low temperatures, minimizing collateral thermal necrosis to adjacent healthy cartilage.
Fluid Management and Irrigation Systems
Continuous irrigation is mandatory during arthroscopy to distend the joint cavity, maintain a clear visual field, and flush out blood and surgical debris.
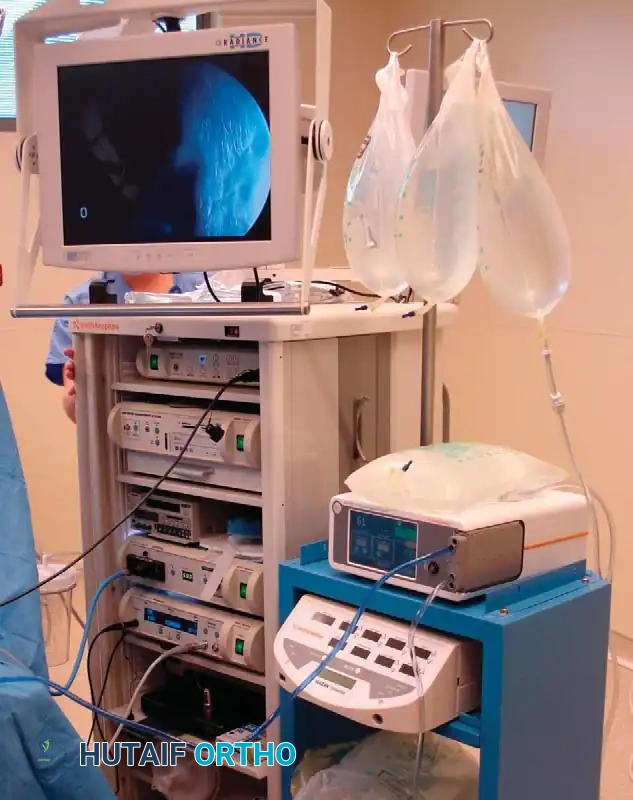
Historically, gravity-fed systems were utilized, requiring fluid bags to be elevated high above the patient. Today, automated mechanical fluid pumps are the standard of care. These sophisticated towers monitor and maintain constant intraarticular pressure and flow rates.
Surgical Warning: Intraarticular pressure must be carefully monitored. Excessive pressure can lead to severe fluid extravasation into surrounding soft tissues, potentially causing compartment syndrome, particularly in the calf or thigh during prolonged knee arthroscopy.
Normal saline or Lactated Ringer's solution are the most common irrigation fluids. Epinephrine (typically 1 mg per 3-liter bag) is frequently added to induce local vasoconstriction and improve visualization by minimizing synovial bleeding.
Patient Positioning and Preparation
Tourniquet and Leg Holders
Proper patient positioning and the use of specialized stabilization devices are critical for successful arthroscopy, particularly in the knee.

A pneumatic tourniquet is routinely placed on the proximal thigh. While many surgeons perform arthroscopy without inflating the tourniquet to minimize postoperative pain and ischemic complications, it remains in place as a fail-safe should uncontrollable bleeding obscure the visual field.
Leg holders or lateral posts are utilized to secure the thigh, allowing the surgeon to apply controlled varus or valgus stress. This stress opens the medial or lateral compartments, providing the necessary space to maneuver instruments without causing iatrogenic scuffing of the articular cartilage.
Basic Arthroscopic Techniques: Triangulation
The fundamental psychomotor skill required for operative arthroscopy is triangulation.
Triangulation is the technique of bringing the arthroscope (the "eye") and the operative instrument (the "hand") together at a specific target within the joint. Because the surgeon is viewing a two-dimensional monitor while operating in a three-dimensional space, spatial proprioception must be meticulously developed.
Steps for Successful Triangulation:
1. Establish the Viewing Portal: Insert the arthroscope and center the target lesion in the middle of the visual field.
2. Localize the Instrument Portal: Use a spinal needle under direct intraarticular visualization to determine the optimal trajectory and entry point for the working instrument.
3. Introduce the Instrument: Advance the instrument blindly through the capsule until it enters the fluid-filled joint space.
4. Converge: Keep the arthroscope completely still. Slowly advance the instrument until its tip enters the field of view.
The skin portal acts as a fulcrum; moving the handle of the instrument externally in one direction causes the intraarticular tip to move in the opposite direction. Mastery of this fulcrum effect is the hallmark of an expert arthroscopist.
Complications in Arthroscopy
While arthroscopy is generally considered minimally invasive and safe, complications can and do occur. A thorough understanding of regional anatomy and strict adherence to surgical principles are required to minimize morbidity.
Iatrogenic Damage to Intraarticular Structures
The most common complication is iatrogenic scuffing or gouging of the articular cartilage. This usually occurs during blind insertion of the trocar or when forcing instruments into tight compartments without adequate joint distraction. Damage to the menisci, fat pad, or native cruciate ligaments can also occur if motorized shavers are used recklessly without keeping the blade window in direct view.
Extraarticular and Neurovascular Injury
- Blood Vessels: The popliteal artery is at extreme risk during posterior compartment work in the knee. Penetration of the posterior capsule must be strictly avoided.
- Nerves: The saphenous nerve (specifically its infrapatellar branch) is vulnerable during medial portal placement. The common peroneal nerve is at risk during lateral meniscal repairs or posterolateral portal establishment.
Fluid Extravasation and Compartment Syndrome
Capsular rents or prolonged high-pressure pump usage can force irrigation fluid into the fascial compartments of the leg or thigh. If the calf becomes tense and non-compressible, the procedure must be aborted, and compartment pressures measured immediately.
Infection and Thrombophlebitis
Septic arthritis following arthroscopy is rare (incidence < 0.5%) but devastating. Strict aseptic technique and proper instrument sterilization are non-negotiable. Deep vein thrombosis (DVT) can occur, particularly in patients with pre-existing risk factors or those subjected to prolonged tourniquet times.
Instrument Breakage
The harsh mechanical environment of the joint can lead to the breakage of delicate instruments, particularly the tips of probes or basket forceps. If an instrument breaks, the surgeon must immediately stop fluid flow (to prevent the fragment from migrating), keep the arthroscope focused on the broken piece, and introduce a magnetic grasper or hemostat through a secondary portal to retrieve it.
Conclusion
Arthroscopy represents a pinnacle of modern orthopaedic surgery, blending complex optical physics with refined surgical anatomy. Mastery of the general principles—ranging from the nuances of fiberoptic illumination and fluid dynamics to the precise psychomotor execution of triangulation—is essential for any orthopaedic surgeon. By respecting the indications, understanding the instrumentation, and anticipating potential complications, the surgeon can leverage arthroscopy to deliver superior, minimally invasive care with excellent clinical outcomes.
