Comprehensive Introduction and Patho-Epidemiology
The precise evaluation and surgical management of peripheral nerve injuries in the upper extremity represent some of the most formidable challenges in orthopedic and reconstructive microsurgery. These injuries, ranging from simple compression neuropathies to devastating avulsions and transections, require a profound understanding of neuroanatomy, muscle biomechanics, and anomalous innervation patterns. Foundational texts, notably the seminal works of MacKinnon and Dellon, emphasize that accurate clinical diagnosis dictates both the timing and the nature of surgical intervention. A meticulous physical examination must isolate individual muscle functions, eliminating the confounding effects of synergistic muscles and trick movements, to establish an accurate baseline for both intervention and prognostication.
Epidemiologically, upper extremity peripheral nerve injuries predominantly affect young, active demographics, frequently resulting from high-energy motor vehicle collisions, industrial accidents, penetrating trauma, and iatrogenic causes. The incidence of peripheral nerve injury is estimated to occur in 2% to 3% of all major trauma patients, with the radial, ulnar, and median nerves being the most frequently compromised. The socioeconomic burden is immense, given the prolonged recovery periods, the necessity for specialized rehabilitation, and the potential for permanent functional impairment and chronic neuropathic pain. The pathophysiology of these injuries is governed by the principles of Wallerian degeneration, a highly orchestrated cellular process wherein the distal axonal segment and its myelin sheath disintegrate following transection or severe crush.
At the cellular level, within hours of a neurotmesis injury, the proximal axonal stump undergoes retrograde degeneration to the next node of Ranvier, while the neuronal cell body undergoes chromatolysis, shifting its metabolic machinery from neurotransmission to structural protein synthesis. Concurrently, in the distal stump, Schwann cells proliferate and align within the basal lamina tubes to form the bands of Büngner, creating a biological conduit essential for guiding regenerating axons. Macrophages infiltrate the site to clear myelin debris, a critical step since myelin-associated glycoproteins strongly inhibit axonal sprouting. Successful regeneration depends entirely on the ability of the proximal axonal sprouts—advancing at a theoretical maximum rate of 1 mm per day—to cross the zone of injury and enter these distal endoneurial tubes before target motor endplates undergo irreversible fibrosis and atrophy, a process typically culminating between 12 and 18 months post-injury.
Understanding the classification of nerve injuries is paramount for clinical decision-making. The Seddon classification divides injuries into neurapraxia (focal conduction block with intact axonal continuity), axonotmesis (axonal disruption with intact supportive connective tissue frameworks), and neurotmesis (complete anatomical transection). Sunderland further expanded this into a five-degree system, detailing the progressive involvement of the endoneurium, perineurium, and epineurium. These classifications are not merely academic; they directly dictate the necessity for surgical exploration. While neurapraxic and lower-grade axonotmetic injuries typically recover spontaneously with conservative management, higher-grade Sunderland injuries and complete neurotmesis mandate meticulous microsurgical reconstruction to restore functional continuity and mitigate the devastating sequelae of permanent denervation.
Detailed Surgical Anatomy and Biomechanics
The microanatomy of a peripheral nerve is a complex, hierarchical arrangement of neural and connective tissues designed to facilitate rapid signal conduction while withstanding significant biomechanical stress. The individual axon is surrounded by the endoneurium, a delicate matrix that maintains the optimal microenvironment for the axon and its investing Schwann cells. Bundles of axons are grouped into fascicles, which are encased by the perineurium. The perineurium is a robust, metabolically active layer that provides the primary tensile strength of the nerve and maintains the blood-nerve barrier. Fascicles are subsequently bound together by the internal epineurium, and the entire nerve trunk is ensheathed by the external epineurium, which provides a gliding surface against surrounding fascial planes. The topographic arrangement of fascicles within the nerve trunk is highly dynamic; fascicles frequently branch and anastomose as they travel distally, transitioning from a polyfascicular, intermingled arrangement proximally to a more segregated, target-specific grouping distally.
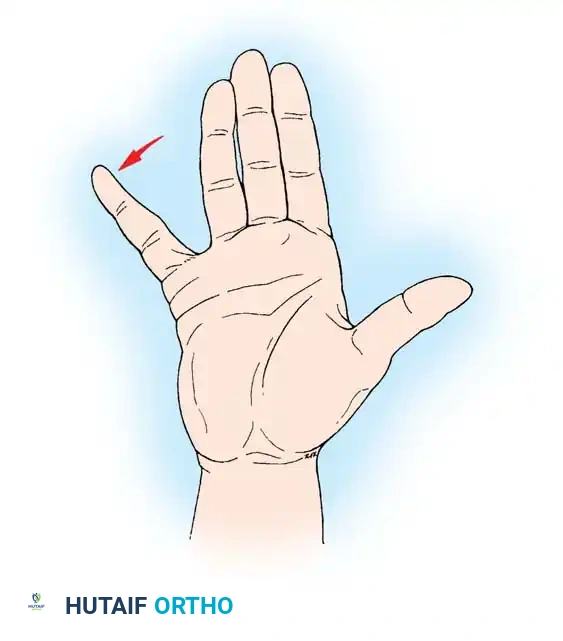
The median nerve serves as the primary motor nerve for the flexor compartment of the forearm and the precision pinch mechanics of the hand. Proximally, it innervates the pronator teres, flexor carpi radialis (FCR), palmaris longus, and flexor digitorum sublimis (FDS). The anterior interosseous nerve (AIN) branch, a critical motor sub-component, supplies the index and middle flexor digitorum profundus (FDP), the flexor pollicis longus (FPL), and the pronator quadratus. In the hand, the median nerve innervates the critical intrinsic muscles responsible for opposition: the lumbricals to the index and long fingers, the opponens pollicis, the abductor pollicis brevis (APB), and the superficial head of the flexor pollicis brevis (FPB). The single most reliable median nerve–mediated motor function to evaluate is the apposition of the tip of the thumb to the pulp of the ring or little finger. Visual inspection alone is insufficient; the examiner must simultaneously palpate the active contraction of the APB muscle belly to ensure the motion is not a "trick movement" generated by the adductor pollicis (ulnar nerve) or the FPL (AIN).
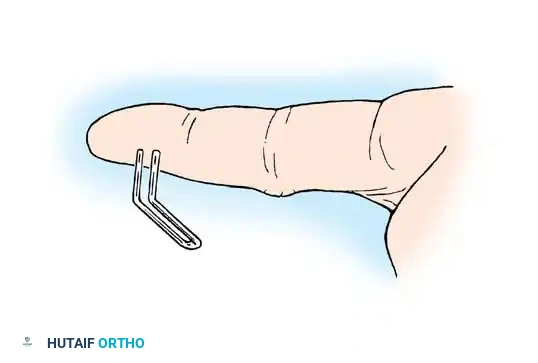
The ulnar nerve governs the intrinsic power and synchronized digital motion of the hand. Proximally, it innervates the flexor carpi ulnaris (FCU) and the ulnar half of the FDP. Distally, it supplies the deep head of the FPB, the adductor pollicis, the hypothenar group (abductor digiti minimi, flexor digiti minimi, opponens digiti minimi), all interosseous muscles, and the ulnar two lumbricals. Evaluation requires careful isolation of the intrinsic muscles from the extrinsic long flexors and extensors. The standard test involves active abduction of the middle finger (Egawa's sign) with the palm resting flat to neutralize extrinsic forces. Thumb adduction is evaluated using Froment’s Sign; if the adductor pollicis is paralyzed, the patient hyperflexes the thumb IP joint (recruiting the FPL) to hold a piece of paper. Abductor digiti minimi (ADM) function is isolated by resisting little finger abduction while palpating the muscle belly.
The radial nerve provides the essential stable platform required for effective grip strength by controlling extension of the elbow, wrist, and digits. Proximally, it innervates the triceps, brachioradialis, supinator, and anconeus. Distally, it supplies the extensor carpi radialis longus (ECRL) and brevis (ECRB), extensor carpi ulnaris (ECU), extensor digitorum communis (EDC), extensor indicis proprius (EIP), extensor digiti minimi (EDM), abductor pollicis longus (APL), extensor pollicis longus (EPL), and extensor pollicis brevis (EPB). A critical pitfall in examination is confusing MCP extension (strictly radial nerve via EDC) with PIP/DIP extension (intrinsic muscles via lateral bands, innervated by median and ulnar nerves). Furthermore, surgeons must maintain a high index of suspicion for anomalous innervation patterns, such as the Martin-Gruber anastomosis (median to ulnar crossover in the forearm, up to 15% prevalence) and the Riche-Cannieu anastomosis (ulnar to median connection in the palm), which can drastically confound clinical localization.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical exploration and reconstruction of upper extremity peripheral nerve injuries is dictated by the mechanism of injury, the temporal relationship to the trauma, and the specific anatomical level of the lesion. In cases of sharp, penetrating trauma (e.g., knife wounds, glass lacerations) where a corresponding motor or sensory deficit is immediately apparent, the diagnosis of neurotmesis is presumed. These scenarios mandate early surgical exploration and primary repair, ideally within 72 hours of the injury. Early intervention in sharp transections allows for direct end-to-end epineurial repair before the nerve ends undergo significant retraction and before the surrounding tissues become indurated and scarred, which would necessitate the use of nerve grafts later.
Conversely, closed injuries resulting from high-energy traction, crush mechanisms, or blunt trauma present a more complex diagnostic dilemma. These lesions frequently represent a continuum of neurapraxia and axonotmesis, which have the potential for spontaneous recovery. The standard of care dictates a period of expectant management and serial clinical examinations for approximately 3 months. If, at the 12-week mark, clinical evaluation and electromyographic (EMG) evidence demonstrate an absolute absence of nascent motor unit action potentials (MUAPs) or signs of advancing Tinel's sign, surgical exploration is indicated. Iatrogenic injuries represent a unique subset; if a nerve deficit is noted immediately following an orthopedic procedure where the nerve was at risk but not directly visualized (e.g., radial nerve palsy after humeral shaft plating), immediate exploration is generally warranted to rule out entrapment, transection, or hardware impingement.
Contraindications to peripheral nerve surgery are generally relative but must be carefully weighed against the potential benefits. Severe, untidy wounds with massive soft tissue avulsion and gross contamination preclude immediate primary repair; in such instances, the nerve ends should be tagged for delayed reconstruction once the soft tissue envelope is stabilized. Systemic medical instability or life-threatening polytrauma naturally takes precedence over peripheral nerve reconstruction. Furthermore, delayed presentations beyond 18 to 24 months post-injury represent a significant biological contraindication to traditional nerve repair or grafting for motor recovery. At this late stage, the target motor endplates have undergone irreversible fibrosis, and the muscles have suffered severe fatty infiltration and atrophy. In these chronic scenarios, the surgical strategy must shift from nerve reconstruction to salvage procedures, such as regional tendon transfers or free functioning muscle transfers.
| Parameter | Indications for Surgical Intervention | Contraindications / Relative Contraindications |
|---|---|---|
| Mechanism | Sharp lacerations with immediate distal deficits; iatrogenic injuries with known intraoperative nerve risk. | Massive crush injuries with extensive soft tissue loss (requires delayed repair). |
| Timing | Acute (<72 hours) for sharp cuts; 3 months for closed traction/crush injuries showing no EMG recovery. | Late presentation (>18-24 months) for motor repair due to irreversible motor endplate fibrosis. |
| Clinical Signs | Advancing Tinel's sign halts; persistent dense anesthesia; complete flaccid paralysis without spontaneous recovery. | Documented clinical or EMG evidence of progressive reinnervation (continue observation). |
| Patient Factors | Motivated patient capable of adhering to strict, prolonged postoperative rehabilitation protocols. | Medically unstable polytrauma; severe non-compliance; active deep infection at the surgical site. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful peripheral nerve reconstruction. The process begins with a meticulous clinical evaluation that documents the precise extent of motor and sensory deficits. Motor function is graded using the Medical Research Council (MRC) scale from M0 (no contraction) to M5 (normal power). Sensibility testing must be rigorous, utilizing static and moving two-point discrimination tests to evaluate slowly adapting (Merkel cells) and quickly adapting (Meissner corpuscles) mechanoreceptors, respectively. Autonomic evaluation is equally critical; complete nerve transection results in an immediate loss of sympathetic tone, leading to anhidrosis. In the acute setting, the denervated skin will feel smooth and lack normal tactile friction. Formal testing can be documented using the Ninhydrin test or the O'Riain wrinkle test, where denervated skin fails to wrinkle when submerged in warm water.
Electrodiagnostic studies, comprising Electromyography (EMG) and Nerve Conduction Studies (NCS), are indispensable adjuncts in the pre-operative workup, particularly for closed injuries. However, timing is critical; Wallerian degeneration must progress sufficiently before EMG changes become apparent. Fibrillation potentials and positive sharp waves, indicative of muscle denervation, typically do not appear until 3 to 4 weeks post-injury. NCS can help localize the lesion by demonstrating conduction block or severe amplitude attenuation across the zone of injury. Advanced imaging modalities are increasingly utilized in pre-operative templating. High-resolution ultrasound (HRUS) provides real-time, dynamic assessment of nerve continuity, neuroma formation, and anatomical variants. Magnetic Resonance Neurography (MRN) offers exquisite soft-tissue contrast, allowing for the visualization of nerve fascicular architecture, surrounding scar tissue, and denervation edema within target muscles.
Patient positioning and operating room setup must be meticulously orchestrated to facilitate unhindered access and optimal microsurgical conditions. The patient is typically positioned supine with the affected extremity extended on a radiolucent hand table. The use of a pneumatic tourniquet is absolute critical for providing the bloodless field required for microsurgery. Following extremity exsanguination with an Esmarch bandage, the tourniquet is inflated to 250 mmHg (or approximately 100 mmHg above the patient's systolic blood pressure). Tourniquet time must be strictly monitored and generally should not exceed 120 minutes without a reperfusion interval, to prevent ischemic damage to the already compromised neural and muscular tissues. The operating microscope must be positioned and balanced prior to the incision, ensuring that both the primary surgeon and the assistant have comfortable, ergonomic access to the surgical field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to peripheral nerve injuries demands extensile exposures that allow for the identification of normal anatomy both proximal and distal to the zone of injury. Incisions must be carefully planned to avoid crossing flexion creases at right angles. In the digits, palm, and volar wrist, Brunner zig-zag incisions or lazy-S incisions are mandatory to prevent the development of postoperative flexion contractures. Dissection always proceeds from known, healthy tissue toward the scarred, injured zone. The nerve is identified in virgin tissue planes and mobilized with vessel loops. Meticulous hemostasis is maintained using bipolar electrocautery to avoid thermal injury to the nerve. Once the injured segment is isolated, external neurolysis is performed to free the nerve from surrounding scar tissue, allowing for an accurate assessment of the lesion's continuity and tension.
If a complete transection (neurotmesis) is identified, the preparation of the nerve ends is the most critical step in the repair process. The injured nerve stumps must be serially resected back to healthy, viable tissue. Using a fresh surgical blade or specialized nerve scissors, the surgeon sections the nerve until healthy, bleeding fascicles are visualized. A classic hallmark of adequate resection is the "pouting" fascicle sign, where the endoneurial contents bulge slightly beyond the cut edge of the epineurium, indicating that the restrictive scar tissue has been bypassed. The primary axiom of nerve surgery is that repairs must be completely tension-free. Tension across a neurorrhaphy site compromises intraneural microvascular perfusion, leading to ischemia, increased scar proliferation, and ultimately, failure of axonal regeneration. If the nerve ends cannot be approximated without tension, even after extensive mobilization and joint positioning, a nerve graft or conduit must be utilized.
For primary end-to-end repairs, the epineurial technique is the gold standard. Under the high magnification of an operating microscope, the superficial epineurial vascular markings are aligned to prevent rotational malalignment of the fascicular topography. The epineurium is approximated using 8-0 or 9-0 non-absorbable monofilament sutures (e.g., Nylon). The first two sutures are placed 180 degrees apart to act as traction and alignment sutures, followed by the placement of intervening sutures just tight enough to coapt the fascicles without buckling. If a gap exists, autologous nerve grafting remains the gold standard. The reversed sural nerve is the most frequently utilized donor, providing up to 40 cm of expendable graft material. The graft is reversed to prevent regenerating axons from escaping through side branches. In modern practice, distal nerve transfers (e.g., transferring the expendable AIN branch of the pronator quadratus to the deep motor branch of the ulnar nerve) are increasingly utilized to bypass long regeneration distances and restore critical intrinsic function more rapidly.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical technique, peripheral nerve reconstruction is fraught with potential complications, primarily due to the complex biological constraints of axonal regeneration. The most frequent and frustrating complication is the failure of adequate motor or sensory recovery, which can occur in up to 30-40% of proximal nerve injuries. This failure is often multifactorial, resulting from extensive zones of injury, prolonged denervation times leading to motor endplate atrophy, or intraneural scarring at the coaptation site. Another significant complication is the formation of a symptomatic neuroma, which occurs when regenerating axons escape the repair site or fail to find distal endoneurial tubes, forming a disorganized, painful mass of nerve tissue and scar. Neuromas can cause debilitating neuropathic pain and severe hypersensitivity, drastically reducing the patient's quality of life.
Complex Regional Pain Syndrome (CRPS) is a devastating complication characterized by severe, disproportionate pain, autonomic dysfunction, trophic changes, and joint stiffness. Its incidence following peripheral nerve injury varies but is a constant threat that requires aggressive, multidisciplinary management, including sympathetic blocks, gabapentinoids, and intensive desensitization therapy. Joint contractures frequently develop as a secondary complication of prolonged immobilization or muscle imbalance resulting from the denervation. For example, in high ulnar nerve injuries, the loss of intrinsic muscle function leads to the classic ulnar claw hand deformity, where the extrinsic extensors hyperextend the MCP joints and the extrinsic flexors hyperflex the IP joints. Prevention through dynamic splinting and aggressive hand therapy is far superior to surgical release.
When nerve reconstruction fails or presents too late for primary repair, salvage management relies heavily on regional tendon transfers to restore functional biomechanics. Tendon transfers involve detaching a functioning, expendable muscle-tendon unit and re-routing it to substitute for a paralyzed muscle. For irreversible radial nerve palsy, a classic transfer utilizes the Pronator Teres (PT) to the ECRB for wrist extension, the Flexor Carpi Radialis (FCR) to the EDC for finger extension, and the Palmaris Longus (PL) to the EPL for thumb extension. For median nerve palsy with loss of opposition, an opponensplasty (e.g., transferring the EIP or FDS of the ring finger to the APB) is employed. For ulnar claw hands, procedures such as the Zancolli lasso or FDS transfers are utilized to prevent MCP hyperextension and restore synchronized digital flexion.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Failure of Regeneration | 20% - 40% (higher in proximal lesions) | Motor endplate atrophy, prolonged denervation (>18 mos), excessive tension at repair. | Tendon transfers, free functioning muscle transfers, arthrodesis. |
| Symptomatic Neuroma | 5% - 10% | Extrafascicular axonal escape, inadequate resection of scarred nerve ends. | Excision and burying in muscle/bone, Targeted Muscle Reinnervation (TMR), capping. |
| CRPS (Type II) | 2% - 5% | Abnormal sympathetic-somatic coupling, severe crush, delayed mobilization. | Multidisciplinary pain management, sympathetic blocks, aggressive hand therapy. |
| Joint Contractures | 15% - 25% | Muscle imbalance (e.g., intrinsic minus hand), prolonged static immobilization. | Dynamic splinting, intensive physical therapy, surgical capsulotomy/release. |
Phased Post-Operative Rehabilitation Protocols
The surgical repair of a peripheral nerve is only the beginning of a prolonged, arduous journey toward functional recovery. Post-operative rehabilitation is absolutely critical and must be carefully phased to protect the fragile microsurgical repair while preventing secondary complications such as joint stiffness and tendon adhesions. In 1984, the Clinical Assessment Committee of the American Society for Surgery of the Hand (ASSH) recommended standardized areas of importance in evaluating progress: sensibility testing, motor testing, subjective evaluation, and sudomotor function. The rehabilitation protocol is generally divided into three distinct phases, tailored to the specific nerve injured and the tension of the repair.
Phase I (0-3 Weeks): Protection and Immobilization. Immediately following surgery, the primary goal is to protect the neurorrhaphy site from any tension that could cause dehiscence or ischemia. The extremity is immobilized in a custom thermoplastic orthosis. For volar repairs (median and ulnar nerves), the wrist and digits are typically placed in slight flexion to minimize tension. For dorsal repairs (radial nerve), slight extension is utilized. During this phase, strict elevation and edema control are paramount. While the affected joints are immobilized, active range of motion of all uninvolved adjacent joints (shoulder, elbow, or unaffected digits) is aggressively encouraged to maintain overall limb function and prevent proximal stiffness.
Phase II (3-6 Weeks): Protected Range of Motion. As the epineurial healing progresses and tensile strength increases, the orthosis is systematically adjusted to allow for protected, guided active range of motion. The goal is to initiate nerve and tendon gliding to prevent dense adhesions to the surrounding soft tissue bed, without placing undue stress on the regenerating axons. For a median nerve repair at the wrist, the splint may be adjusted weekly to gradually bring the wrist from a flexed position to neutral. Passive stretching is strictly contraindicated during this phase. Therapists begin gentle scar massage and desensitization techniques once the surgical incisions are fully healed to mitigate hypersensitivity.
Phase III (6+ Weeks): Strengthening and Cortical Remapping. Once the repair site is deemed biomechanically stable, progressive strengthening exercises are initiated. However, the most critical component of Phase III is sensory re-education. Following nerve injury and repair, the regenerating axons rarely return to their exact original sensory receptors, leading to disorganized afferent signals reaching the somatosensory cortex. Sensory re-education utilizes brain plasticity to help the cerebral cortex remap and interpret these altered signals. Patients undergo structured exercises using various textures, shapes, and temperatures, initially with visual feedback and then without, to retrain the brain's spatial recognition and tactile gnosis. Motor relearning programs are similarly employed to overcome trick movements and integrate the newly reinnervated muscles into synchronized, functional use patterns.
Summary of Landmark Literature and Clinical Guidelines
The evolution of peripheral nerve surgery is deeply rooted in landmark anatomical studies and pivotal clinical trials that have shaped modern guidelines. The foundational classifications by Seddon (1943) and Sunderland (1951) remain the bedrock of nerve injury prognostication and surgical decision-making. Their meticulous descriptions of the microarchitectural damage sustained during different injury mechanisms provided the rationale for when to observe and when to operate. The surgical principles of tension-free repair, meticulous fascicular alignment, and the critical biological limits of nerve grafting were heavily championed by Millesi in the 1970s, whose work on interfascicular nerve grafting revolutionized the management of large nerve defects.
Further advancements in the clinical evaluation of nerve recovery were codified by the American Society for Surgery of the Hand (ASSH) Clinical Assessment Committee in 1984. Their guidelines established the standardized use of static and moving two-point discrimination (popularized by Dellon and Weber) as the most reliable metrics for sensibility evaluation. Dellon's work specifically highlighted that moving two-point discrimination (evaluating quickly adapting Meissner corpuscles) is typically the first sensory modality to return following a nerve repair, serving as an early clinical indicator of successful regeneration. MacKinnon's extensive contributions to both the basic science of nerve regeneration and the clinical application of nerve transfers have fundamentally shifted the paradigm of severe nerve injury management.
In the modern era, clinical guidelines increasingly emphasize the utility of distal nerve transfers over lengthy traditional nerve grafts, particularly for proximal injuries where the time required for axonal regeneration would exceed the biological viability of the target motor endplates. Landmark papers, such as Oberlin's description of transferring ulnar nerve fascicles to the musculocutaneous nerve for biceps reinnervation, have paved the way for similar intra-hand transfers (e.g., AIN to deep ulnar motor branch). Current consensus guidelines advocate for a multidisciplinary approach, combining early, precise microsurgical intervention with advanced, neuroplasticity-focused rehabilitation protocols, to maximize functional outcomes in these devastating injuries.
