Forearm Fasciotomy and Arterial Exploration: A Comprehensive Surgical Guide

Key Takeaway
Forearm fasciotomy is an emergent surgical intervention required to decompress elevated intracompartmental pressures and prevent irreversible ischemic necrosis, known as Volkmann contracture. This comprehensive guide details the volar, dorsal, and hand fasciotomy techniques, emphasizing precise anatomical approaches, arterial exploration protocols, and delayed wound closure strategies such as the vessel loop shoelace technique to optimize functional recovery in acute compartment syndrome.
INTRODUCTION TO FOREARM COMPARTMENT SYNDROME
Acute compartment syndrome (ACS) of the forearm is a devastating orthopedic emergency characterized by elevated intracompartmental pressure within a closed osteofascial space. This elevated pressure compromises local microvascular perfusion, initiating a catastrophic ischemic cascade that, if left untreated, culminates in irreversible myonecrosis and nerve death. The ultimate sequela of missed or inadequately treated forearm compartment syndrome is Volkmann ischemic contracture, a severely debilitating condition that permanently compromises upper extremity function.
Prompt recognition and emergent surgical decompression via forearm fasciotomy remain the absolute standard of care. This procedure must frequently be coupled with arterial exploration in cases of concomitant vascular injury, such as supracondylar humerus fractures or penetrating trauma, where arterial spasm, intimal tearing, or thrombosis may perpetuate distal ischemia even after fascial release.
This masterclass provides an exhaustive, step-by-step academic guide to the surgical management of forearm compartment syndrome, detailing the volar and dorsal approaches, hand fasciotomies, arterial exploration protocols, and advanced postoperative wound management techniques.
PATHOPHYSIOLOGY AND ESTABLISHED VOLKMANN CONTRACTURE
The Ischemic Cascade
Compartment syndrome develops when tissue pressure exceeds the venous capillary perfusion pressure (typically when the delta pressure—diastolic blood pressure minus intracompartmental pressure—falls below 30 mm Hg). This leads to venous hypertension, capillary collapse, and anoxic injury to the muscle and nerve tissues. Muscle tissue can survive approximately 4 hours of total ischemia before irreversible changes begin, with near-complete myonecrosis occurring by 8 hours.
Established Volkmann Contracture of the Forearm
If a compartment syndrome is untreated or inadequately treated, compartment pressures continue to increase until irreversible tissue ischemia occurs. Fibroblastic proliferation replaces necrotic muscle tissue, leading to dense scarring and contracture.
Volkmann ischemic contracture is the result of several different degrees of tissue injury; however, the earliest and most profound changes usually involve the deep flexor compartment, specifically the flexor digitorum profundus (FDP) and flexor pollicis longus (FPL) muscles in the middle third of the forearm.
Clinical Pearl: The Classic Volkmann Posture
The typical clinical picture of an established, severe Volkmann contracture is biomechanically predictable based on the involved musculature. It includes:
* Elbow flexion (due to flexor origin contracture)
* Forearm pronation (due to pronator teres and pronator quadratus fibrosis)
* Wrist flexion (due to primary wrist flexor contracture)
* Thumb adduction and flexion
* Metacarpophalangeal (MCP) joint extension (due to extrinsic extensor overtensioning and intrinsic paralysis)
* Interphalangeal (PIP and DIP) finger flexion (due to FDP and FDS contracture)
Degrees of Contracture
- Mild (Localized) Volkmann Contracture: Results from partial ischemia of the profundus mass. Flexion contractures usually involve only two or three fingers (most commonly the middle and ring fingers). Sensory changes are usually mild or absent. Intrinsic muscle contractures and joint contractures are absent. During the early stages of a mild contracture, dynamic splinting may be attempted, but surgical release is often eventually required.
- Moderate Contracture: Involves the classic posture described above, with involvement of the FDP, FDS, and FPL. Median and ulnar nerve sensory deficits are common due to direct ischemic neuropathy or secondary compression.
- Severe Contracture: Involves both the flexor and extensor compartments, presenting with a globally contracted, insensate, and non-functional hand.
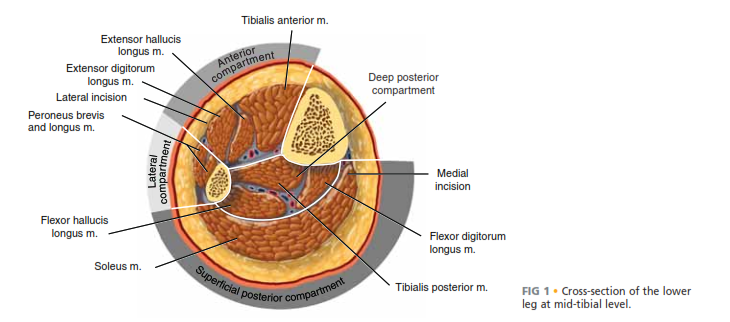
SURGICAL ANATOMY AND COMPARTMENTAL BIOMECHANICS
The forearm is anatomically divided into three primary compartments, each requiring specific attention during decompression:
- Volar (Flexor) Compartment: Divided into superficial and deep spaces. The deep space (containing the FDP, FPL, and pronator quadratus) is the most frequently and severely affected by ACS.
- Dorsal (Extensor) Compartment: Contains the extrinsic extensors of the wrist and digits.
- Mobile Wad of Henry: Contains the brachioradialis, extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB).
PREOPERATIVE PREPARATION
- Indications: Clinical diagnosis of ACS (pain out of proportion, pain with passive stretch, tense compartments) or a Delta Pressure < 30 mm Hg in an obtunded patient.
- Anesthesia: General anesthesia is preferred. Regional anesthesia is generally contraindicated preoperatively as it masks the cardinal symptom of breakthrough pain, but may be utilized post-decompression for pain control.
- Tourniquet: The use of a pneumatic tourniquet is controversial. If used to rapidly obtain initial hemostasis and anatomical orientation, it must be deflated immediately after the fascial incisions are made to assess muscle viability, reactive hyperemia, and the need for arterial exploration.
- Positioning: Supine with the affected upper extremity extended on a radiolucent hand table.
SURGICAL TECHNIQUE: VOLAR FOREARM FASCIOTOMY
The volar approach is the workhorse of forearm decompression. It must release both the superficial and deep flexor compartments, as well as the carpal tunnel.
Incision used for anterior forearm compartment syndromes in which skin and underlying fascia are released completely throughout.
Step-by-Step Volar Approach
- Incision Design: Begin the incision just proximal and medial to the medial epicondyle. Extend it distally and laterally across the antecubital fossa in a curvilinear fashion to avoid crossing the flexor crease at a right angle (which risks future flexion contracture).
- Forearm Extension: Continue the incision distally along the volar forearm, curving gently toward the ulnar border of the distal forearm.
- Wrist and Palm: As the incision approaches the wrist, curve it back radially to cross the wrist crease obliquely, extending into the palm along the thenar crease to facilitate a complete carpal tunnel release.
- Superficial Fascial Release: Incise the superficial fascia of the forearm completely from the elbow to the wrist. Identify and protect the medial antebrachial cutaneous nerve.
- Carpal Tunnel Release: Divide the transverse carpal ligament completely to decompress the median nerve.
- Deep Compartment Release: Retract the flexor carpi ulnaris (FCU) ulnarly and the flexor digitorum superficialis (FDS) radially. This exposes the deep fascial envelope overlying the FDP and FPL. Incise this deep epimysium longitudinally.
- Muscle Assessment: Inspect the muscle bellies for color, consistency, contractility, and capacity to bleed (the "4 Cs"). Necrotic muscle that is frankly mushy and non-contractile should be judiciously debrided, though marginal tissue should be left for re-evaluation at a second-look surgery 48 hours later.
SURGICAL TECHNIQUE: DORSAL FOREARM FASCIOTOMY
While the volar fasciotomy often decompresses the dorsal musculature sufficiently due to the interconnected nature of the fascial septa, the dorsal compartments must be clinically re-evaluated or have their pressures re-measured after volar release. If involvement of the dorsal compartments is still suspected, they must be released independently.

Extensive opening of fascia of dorsum of forearm in dorsal compartment syndromes.
Step-by-Step Dorsal Approach
- Incision Placement: Make a longitudinal straight incision starting distal to the lateral epicondyle, running between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis (ECRB).
- Extension: Extend the incision approximately 10 cm distally.
- Subcutaneous Dissection: Gently undermine the subcutaneous tissue radially and ulnarly to maximize fascial exposure while preserving the superficial radial nerve and posterior antebrachial cutaneous nerve.
- Fascial Release: Release the fascia overlying the mobile wad of Henry (brachioradialis, ECRL, ECRB).
- Extensor Retinaculum: Continue the fascial release distally to include the proximal border of the extensor retinaculum if distal dorsal swelling is severe.
SURGICAL TECHNIQUE 74-3: HAND AND DIGITAL FASCIOTOMY
In general, it is prudent to release all compartments, including the carpal tunnel, if any of the hand compartments are involved. Tensely swollen fingers with delayed capillary refill mandate immediate digital decompression.
Step-by-Step Hand Decompression
- Dorsal Hand Incisions: Make two dorsal parallel incisions through the skin overlying the second and fourth metacarpals. Begin at the level of the metacarpophalangeal (MCP) joints and extend just distal to the wrist.
- Interosseous Release: Make each incision down to the musculofascial area. Incise the fascia and release the compression of the distended dorsal and volar interosseous muscles, allowing them to extrude into the wound if necessary.
- Muscle Verification: Identify each muscle individually to ensure that a complete release is done. Passively flex the MCP joints and extend the proximal interphalangeal (PIP) joints to stretch the intrinsic muscles, ensuring that all are adequately released.
> 🚨 Surgical Warning: Do not attempt to débride the interosseous muscles at this point. Ischemic intrinsic muscles may appear marginal initially but can recover significantly once perfusion is restored. - Thenar and Hypothenar Release: Release the thenar and hypothenar compartments by making additional palmar radial and palmar ulnar incisions along the glabrous and nonglabrous interval to allow for their separate decompression.
- Digital Fasciotomies: If the fingers remain tensely swollen and capillary refill is delayed, continue with digital fasciotomies. Make midlateral incisions along the radial border of the ring and small fingers, and the ulnar border of the index and long fingers.
ARTERIAL EXPLORATION
In cases of severe trauma (e.g., supracondylar humerus fractures, crush injuries, or penetrating wounds), the absence of a distal pulse following fracture reduction and fascial decompression necessitates immediate arterial exploration.
- Exposure: The volar fasciotomy incision provides excellent extensile exposure to the brachial artery at the antecubital fossa, as well as its bifurcation into the radial and ulnar arteries.
- Vascular Assessment: Inspect the artery for contusion, intimal tearing, or thrombosis.
- Management of Spasm: If the artery is in severe spasm but structurally intact, bathe the vessel in warm saline or topical papaverine. Gently dilate the adventitia.
- Thrombectomy/Repair: If a thrombus is present, a transverse arteriotomy and Fogarty catheter thrombectomy may be required. If a segment of the artery is irreparably crushed or thrombosed, resection and reconstruction with a reversed saphenous vein graft is indicated. Orthopedic surgeons should have a low threshold to consult vascular surgery colleagues if complex reconstruction is required.
POSTOPERATIVE CARE AND WOUND MANAGEMENT
The management of the fasciotomy wound is as critical as the decompression itself. Under no circumstances should the wounds be closed primarily at the index operation.
Immediate Postoperative Protocol
- Dressing: Apply a sterile, non-adherent moist dressing. A vacuum-assisted wound closure (VAC) system is highly recommended to assist in wound management, manage exudate, and reduce interstitial edema.
- Splinting: Apply a bulky long-arm splint. The elbow should not be left flexed beyond 90 degrees to prevent vascular kinking. The wrist should be splinted in neutral to slight extension, with MCP joints in 70-90 degrees of flexion and IP joints fully extended (intrinsic-plus position).
- Elevation: The arm must be strictly elevated for 24 to 48 hours after surgery to facilitate venous and lymphatic drainage.
Delayed Wound Closure Strategies
Patients are typically returned to the operating room at 48 to 72 hours for a "second look" to reassess muscle viability, perform necessary debridement, and evaluate for closure.
- Split-Thickness Skin Grafting (STSG): If primary closure is not possible within 5 to 7 days due to persistent muscle edema, a split-thickness skin graft should be applied over the muscle bed.
- Vessel Loop Shoelace Technique: Alternatively, closure of fasciotomy wounds can be accomplished gradually with progressive tension using vessel loops.
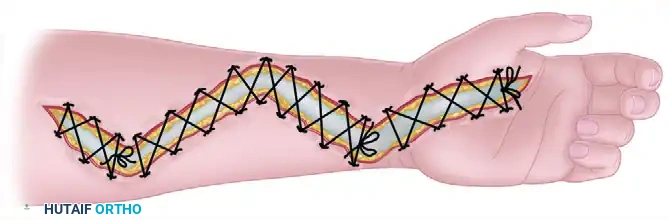
FIGURE 74-6 Vessel loop shoelace technique for fasciotomy closure.
Clinical Pearl: The Shoelace Technique
The vessel loop shoelace technique utilizes silastic vessel loops stapled to the dermal edges of the wound in a crisscross pattern. The loops are tightened progressively postoperatively during dressing changes (or subsequent trips to the OR). This provides continuous, dynamic dermatotraction, counteracting skin retraction. Wound closure by this method usually can be accomplished in 2 weeks, often negating the need for a skin graft and providing a superior cosmetic and functional result.
Rehabilitation
The splint is worn until sutures are removed or as determined by concomitant fracture care. Once the wounds are stabilized, aggressive occupational therapy is initiated, focusing on passive and active range of motion of the digits, wrist, and elbow to prevent tendon adhesions and joint contractures.
CONCLUSION
Forearm fasciotomy is a limb-saving procedure that demands a thorough understanding of upper extremity cross-sectional anatomy and the pathophysiology of compartment syndrome. By meticulously executing the volar and dorsal releases, aggressively decompressing the hand when indicated, and employing advanced delayed closure techniques like the vessel loop shoelace method, orthopedic surgeons can halt the ischemic cascade, prevent the devastating onset of Volkmann contracture, and maximize the patient's functional recovery.
You Might Also Like