First Metatarsophalangeal (MTP) Joint Arthrodesis: A Masterclass in Hallux Rigidus Reconstruction

Key Takeaway
Join us in the OR for a detailed masterclass on First Metatarsophalangeal Joint Arthrodesis. We'll navigate the intricate anatomy, meticulous surgical steps, and critical decision-making required for successful fusion in severe hallux rigidus. From precise patient positioning and joint preparation with power reamers to definitive fixation and complication management, this guide provides an exhaustive, surgeon's-eye view of the entire procedure.
Comprehensive Introduction and Patho-Epidemiology
The Evolution of Hallux Rigidus
First metatarsophalangeal (MTP) joint arthrodesis remains the undisputed gold standard for the surgical management of end-stage hallux rigidus, severe hallux valgus, and various inflammatory arthritides affecting the first ray. Hallux rigidus, a term first coined by Cotterill in 1887, describes a progressive, debilitating condition characterized by profound restriction of sagittal plane motion at the first MTP joint, predominantly affecting dorsiflexion. Over the past century, our understanding of this pathology has evolved from a simple mechanical impingement model to a complex interplay of biomechanical, traumatic, and genetic factors. The procedure of arthrodesis itself has undergone significant refinement, transitioning from crude non-fixated resections to highly precise, biomechanically optimized constructs utilizing advanced osteosynthesis principles.
The natural history of hallux rigidus is one of relentless progression. Initially, patients experience episodic synovitis and capsular distension, often misdiagnosed as acute sprains or gout. As the articular cartilage undergoes fibrillation and progressive delamination, the joint attempts to stabilize itself through the formation of robust periarticular osteophytes. These osteophytes, particularly prominent on the dorsal and dorsolateral aspects of the metatarsal head, act as mechanical blocks to dorsiflexion, creating the hallmark "rigidus" clinical picture. The loss of the windlass mechanism profoundly alters forefoot kinematics, leading to compensatory transfer metatarsalgia and altered gait mechanics.
Epidemiologically, hallux rigidus is the most common osteoarthritic condition of the foot, affecting approximately 1 in 40 adults over the age of 50. It exhibits a bimodal age distribution, with a younger cohort often presenting secondary to acute trauma or osteochondritis dissecans, and an older cohort presenting with insidious, idiopathic degenerative joint disease. Female patients are disproportionately affected, and bilateral involvement is observed in nearly 80% of idiopathic cases, strongly suggesting an underlying genetic predisposition or inherent anatomical variant that predisposes the joint to premature mechanical failure.
For the orthopedic surgeon, mastering the first MTP arthrodesis is paramount. While joint-sparing procedures such as cheilectomy or interpositional arthroplasty have their indications in earlier stages of the disease, arthrodesis provides definitive, predictable, and durable relief for advanced arthrosis. It restores the weight-bearing capacity of the first ray, realigns severe deformities, and eliminates the pain generator entirely, allowing patients to return to high levels of function and activity with remarkable reliability.
Pathogenesis and Etiological Factors
The exact etiology of idiopathic hallux rigidus remains a subject of ongoing academic debate, though it is widely accepted to be multifactorial. A primary driver is often repetitive microtrauma or a discrete macro-traumatic event, such as a severe hyperextension injury (turf toe) or an intra-articular fracture. These events precipitate an inflammatory cascade within the joint space, leading to the upregulation of matrix metalloproteinases and subsequent degradation of the chondral extracellular matrix. The initial chondral injury, often located on the dorsal aspect of the metatarsal head, progresses to full-thickness cartilage loss and subchondral bone exposure.
Anatomical predispositions play a critical role in the pathogenesis. A flattened or chevron-shaped first metatarsal head is frequently implicated, as it inherently restricts the rolling and gliding motion necessary for normal MTP joint kinematics. Furthermore, an excessively long first metatarsal (index plus) can increase the reactive ground reaction forces transmitted across the joint during the terminal stance phase of gait, accelerating chondral wear. Metatarsus primus elevatus, long debated as either a primary cause or a secondary consequence, is now generally considered by most authorities to be an acquired deformity resulting from the loss of normal plantarflexion power and the dorsal impingement created by osteophytosis.
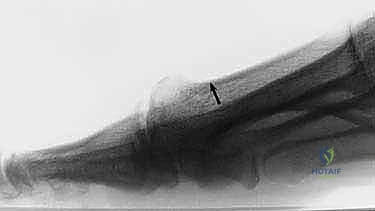
As the degenerative process advances, the joint exhibits characteristic radiographic and gross anatomical changes. Proliferative bone formation occurs at the margins of the articular cartilage, producing massive dorsal osteophytes that resemble "dripping candle wax." These exostoses not only impinge on the proximal phalanx during attempted dorsiflexion but also cause direct pressure symptoms against overlying footwear, leading to adventitial bursitis and severe cutaneous pain. The joint capsule becomes fibrotic and contracted, further tethering the joint and obliterating any remaining physiological motion.
At the cellular level, the subchondral bone undergoes significant remodeling. Sclerosis, cyst formation, and microfractures become evident as the protective cushioning of the cartilage is lost. The sesamoid complex, integral to the function of the flexor hallucis brevis, may also become involved in the arthritic process, leading to severe plantar pain. Understanding this comprehensive pathological cascade is essential for the surgeon, as it dictates the necessity for meticulous joint preparation and complete eradication of the diseased articular surfaces during arthrodesis.
Clinical Presentation and Natural History
Patients presenting with hallux rigidus typically report a long-standing history of deep, aching pain localized to the first MTP joint, exacerbated by weight-bearing activities and the toe-off phase of gait. Early in the disease process, the pain is often insidious and intermittent, correlating with periods of increased activity or the use of flexible, thin-soled footwear that demands greater MTP dorsiflexion. As the condition progresses, the pain becomes constant, and patients may report a grinding or catching sensation within the joint.
A hallmark of the clinical presentation is the presence of a palpable, and often visible, dorsal eminence resulting from the underlying osteophytosis. This prominence is frequently associated with overlying erythema and hyperkeratosis due to chronic shoe wear friction. To mitigate the pain associated with dorsiflexion, patients subconsciously adopt compensatory gait patterns. They often walk with an apropulsive gait, avoiding terminal stance, or they may supinate the foot to offload the medial column, transferring weight to the lateral border of the foot. This compensatory mechanism frequently leads to secondary pathologies, including lateral column overload, transfer metatarsalgia, and exacerbation of pre-existing lesser toe deformities.
Physical examination reveals a profound restriction in active and passive dorsiflexion of the first MTP joint. In advanced cases, plantarflexion is also severely limited. Pain is reliably elicited at the extremes of motion, particularly when the joint is forcibly dorsiflexed, causing impingement of the dorsal osteophytes. The "grind test," performed by applying axial compression with circumduction of the proximal phalanx, typically elicits severe pain and palpable crepitus, confirming the presence of advanced intra-articular arthrosis.
The natural history of untreated hallux rigidus is progressive functional decline. While the rate of progression varies significantly among individuals, the ultimate endpoint is near-complete bony ankylosis of the joint. Although spontaneous autofusion can theoretically eliminate pain by obliterating motion, it rarely occurs in a functionally optimal position. Patients are left with a painful, malaligned, and stiff joint that severely limits their ability to ambulate efficiently or wear standard footwear, underscoring the critical need for surgical intervention when conservative measures fail.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Configuration
The first MTP joint is a complex diarthrodial joint formed by the articulation between the convex head of the first metatarsal and the shallow, concave elliptical base of the proximal phalanx. The metatarsal head is unique in its geometry; it is not a perfect sphere but rather possesses a larger radius of curvature dorsally than plantarly. This cam-like configuration is crucial for normal kinematics, allowing the proximal phalanx to glide dorsally and proximally during toe-off. The articular cartilage covering the metatarsal head extends further plantarly to accommodate the articulation with the sesamoid bones.
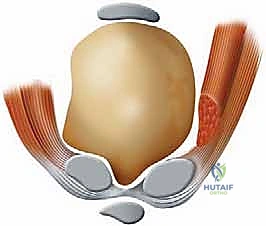
The plantar aspect of the first metatarsal head features two distinct longitudinal grooves separated by a central bony ridge, the crista. These grooves serve as the articulation sites for the medial (tibial) and lateral (fibular) sesamoids. The sesamoids are embedded within the tendinous slips of the flexor hallucis brevis (FHB) and are connected to each other by the strong intersesamoidal ligament. This sesamoid complex functions as a dynamic pulley system, increasing the mechanical advantage of the intrinsic flexor musculature and protecting the underlying flexor hallucis longus (FHL) tendon as it traverses the joint.
The base of the proximal phalanx provides a relatively small articular surface compared to the expansive metatarsal head. This inherent bony mismatch dictates that the stability of the first MTP joint is heavily reliant on its robust capsuloligamentous and musculotendinous envelope. During the surgical preparation for arthrodesis, the surgeon must meticulously decorticate these complex geometries. The dense subchondral bone plate, particularly on the metatarsal head, must be adequately penetrated or completely resected to expose the underlying cancellous bone, which is essential for achieving a robust biological fusion.
Understanding the osteology is also critical for hardware placement. The first metatarsal shaft is composed of dense cortical bone, providing excellent purchase for screws, while the head and the base of the proximal phalanx are predominantly cancellous. Consequently, fixation constructs must be designed to maximize thread purchase in these varying bone densities, often utilizing lag screws to generate interfragmentary compression across the prepared cancellous surfaces.
Musculotendinous and Capsuloligamentous Stabilizers
The dynamic stability of the first MTP joint is governed by a complex array of extrinsic and intrinsic tendons. Dorsally, the extensor hallucis longus (EHL) tendon is the primary extensor, crossing the joint centrally and inserting onto the base of the distal phalanx. It is stabilized by the extensor hood mechanism, which receives contributions from the extensor hallucis brevis (EHB) tendon laterally. The EHL is a critical landmark during the dorsal surgical approach; the incision is typically placed just medial to the EHL to avoid the neurovascular bundle while providing excellent exposure to the joint.
Plantarly, the flexor hallucis longus (FHL) runs through a fibro-osseous tunnel beneath the intersesamoidal ligament, acting as a powerful plantarflexor of the interphalangeal and MTP joints. The intrinsic muscles—the abductor hallucis medially and the adductor hallucis laterally—insert onto the medial and lateral sesamoids and the base of the proximal phalanx. These muscles provide crucial transverse plane stability. In cases of severe hallux valgus requiring arthrodesis, the adductor hallucis may be contracted, necessitating release to achieve proper axial alignment prior to fixation.
The static stabilizers of the joint are equally complex. The joint capsule is relatively thin dorsally but thickens significantly on the plantar aspect to form the plantar plate. The plantar plate is a dense, fibrocartilaginous structure that firmly attaches to the base of the proximal phalanx distally and loosely to the metatarsal neck proximally. It incorporates the sesamoids and provides critical resistance against excessive hyperextension. The collateral ligaments, consisting of the proper collateral and accessory collateral (suspensory) ligaments, originate from the medial and lateral epicondyles of the metatarsal head and insert onto the proximal phalanx and plantar plate, respectively.
During an MTP arthrodesis, a thorough capsular release is mandatory to mobilize the joint and permit accurate realignment. The collateral ligaments are typically excised, and the dorsal capsule is resected along with the impinging osteophytes. However, the surgeon must exercise extreme caution to preserve the integrity of the plantar plate and the FHL tendon, as inadvertent injury to these structures can lead to postoperative morbidity, including flexor weakness and destabilization of the interphalangeal joint.
Neurovascular Topography and Surgical Danger Zones
Meticulous attention to the neurovascular anatomy is paramount when performing a first MTP arthrodesis, as iatrogenic nerve injury is a leading cause of postoperative dissatisfaction. The primary sensory supply to the dorsal aspect of the hallux is derived from the medial dorsal cutaneous nerve (MDCN), a terminal branch of the superficial fibular nerve. The MDCN typically courses obliquely across the extensor tendons, providing branches to the medial aspect of the hallux. Its location is highly variable, making it highly susceptible to injury during the initial skin incision and superficial dissection.
The deep fibular nerve provides the dorsal digital nerve to the first web space, supplying sensation to the lateral aspect of the hallux and the medial aspect of the second toe. This nerve courses lateral to the EHL tendon and the dorsalis pedis artery. While less commonly injured during a standard medial-to-EHL approach, aggressive lateral retraction or errant hardware placement can compromise this structure. Injury to either the MDCN or the deep fibular nerve branches can result in a painful neuroma, complex regional pain syndrome (CRPS), or persistent numbness, significantly detracting from an otherwise successful arthrodesis.
The vascular supply to the first MTP joint is robust, derived primarily from the first dorsal metatarsal artery (a branch of the dorsalis pedis) and the first plantar metatarsal artery. These vessels form an intricate anastomotic ring around the metatarsal head and neck. While devascularization of the metatarsal head leading to avascular necrosis is a recognized complication of distal metatarsal osteotomies (e.g., Chevron procedures), it is exceedingly rare in the context of arthrodesis, provided that the soft tissue stripping is judicious and limited to the articular margins.
The plantar nerves and vessels, derived from the medial plantar nerve and artery, course deep to the abductor hallucis and are generally protected from direct injury during a dorsal approach. However, overzealous plantar dissection, aggressive use of Hohmann retractors, or plunging with a drill bit or saw blade can inadvertently damage these critical plantar structures. The surgeon must always maintain a clear awareness of the depth of the joint and protect the plantar soft tissues during preparation of the articular surfaces.
Biomechanics of the First Ray
The first ray, comprising the first metatarsal and the medial cuneiform, is the primary load-bearing structure of the forefoot during the terminal stance and pre-swing phases of gait. Normal biomechanics rely heavily on the integrity of the first MTP joint and the function of the "windlass mechanism," famously described by Hicks. As the heel lifts and the hallux dorsiflexes, the plantar fascia, which inserts into the base of the proximal phalanx via the plantar plate, is tensioned. This tension effectively shortens the distance between the calcaneus and the metatarsal heads, elevating the medial longitudinal arch and locking the midtarsal joints, thereby creating a rigid lever for propulsion.
In hallux rigidus, the loss of dorsiflexion obliterates the windlass mechanism. The forefoot cannot transition into a rigid lever, resulting in inefficient propulsion and increased stress on the lesser metatarsals. When performing an arthrodesis, the goal is to surgically recreate a stable, propulsive lever arm. The position of fusion is the single most critical factor in achieving a successful biomechanical outcome. The joint must be fused in slight dorsiflexion (typically 15 to 20 degrees relative to the first metatarsal axis) to allow the foot to roll forward smoothly over the hallux during toe-off.
If the joint is fused in excessive plantarflexion, the patient will experience painful impingement at the tip of the toe, excessive pressure on the interphalangeal joint leading to secondary arthritis, and vaulting during gait. Conversely, excessive dorsiflexion results in the hallux failing to purchase the ground, leading to transfer metatarsalgia beneath the lesser metatarsal heads and a significant loss of push-off power. The transverse and frontal plane alignments are equally important; the hallux should be positioned in 10 to 15 degrees of valgus to match the contour of the lesser toes and in neutral rotation to ensure the toenail faces directly upward.
The arthrodesis construct itself must be biomechanically robust enough to withstand the immense bending moments applied to the first ray during gait. The first MTP joint experiences forces exceeding 100% of body weight during normal walking, and significantly higher forces during running or jumping. Modern fixation techniques, utilizing a combination of interfragmentary compression (via a lag screw) and a dorsal neutralization or locking plate, provide superior biomechanical stability compared to historical methods such as isolated K-wires or intramedullary devices, minimizing micromotion and optimizing the environment for primary bone healing.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a first MTP joint arthrodesis must be carefully individualized, taking into account the patient's age, activity level, symptom severity, and specific anatomical deformities. The classic indication is end-stage hallux rigidus (Coughlin and Shurnas Grade 3 or 4), characterized by near-complete loss of articular cartilage, massive osteophytosis, and profound restriction of motion with associated debilitating pain. In these advanced stages, joint-sparing procedures like cheilectomy are highly likely to fail, making arthrodesis the most reliable and definitive treatment option.
Arthrodesis is also the procedure of choice for severe, complex, or recurrent hallux valgus deformities. When the intermetatarsal angle is excessively large, or when the MTP joint is highly unstable or arthritic, an isolated osteotomy may be insufficient to maintain correction. Fusing the MTP joint provides a powerful lever to realign the entire first ray, effectively reducing the intermetatarsal angle without the need for a proximal metatarsal osteotomy. This is particularly relevant in older patients with poor bone quality, where complex osteotomies carry a higher risk of nonunion or hardware failure.
Inflammatory arthropathies, most notably rheumatoid arthritis, frequently devastate the first MTP joint, leading to severe subluxation, dislocation, and erosive cartilage destruction. In this patient population, arthrodesis is universally accepted as the gold standard. It not only eliminates the painful, unstable joint but also provides a stable medial buttress, which is essential when performing concurrent lesser MTP joint resectional arthroplasties (the classic Hoffman procedure) for severe forefoot deformities.
Furthermore, arthrodesis serves as a highly effective salvage procedure for failed previous forefoot surgeries. This includes failed silastic or metallic joint replacements, failed Keller excisional arthroplasties that have resulted in a floppy, non-purchasing toe or transfer metatarsalgia, and failed bunionectomies with resultant avascular necrosis of the metatarsal head or severe iatrogenic hallux varus. In these complex revision scenarios, structural bone grafting (autograft or allograft) may be required to restore the length of the first ray and optimize the biomechanics of the foot.
Absolute and Relative Contraindications
While highly successful, first MTP arthrodesis is not without its limitations, and careful consideration of contraindications is essential to avoid catastrophic failures. Absolute contraindications are relatively few but critical. Active infection, whether systemic or localized to the foot, absolutely precludes any elective arthrodesis procedure. The presence of a compromised soft tissue envelope, such as active ulceration or severe peripheral vascular disease with inadequate perfusion (e.g., Ankle-Brachial Index < 0.5 or non-palpable pulses with poor Doppler signals), is also an absolute contraindication, as the risk of wound dehiscence, deep infection, and subsequent amputation is unacceptably high.
Relative contraindications require nuanced clinical judgment. Severe, symptomatic degenerative joint disease of the interphalangeal (IP) joint of the hallux is a significant concern. Because the MTP arthrodesis transfers increased biomechanical stress to the adjacent IP joint, pre-existing IP arthritis can become rapidly and severely symptomatic postoperatively. In such cases, if MTP arthrodesis is unavoidable, the patient must be extensively counseled regarding the potential need for a subsequent IP joint fusion.
Neuromuscular disorders characterized by severe spasticity or uncontrolled involuntary movements present a major challenge. The constant, unpredictable forces exerted across the fusion site significantly increase the risk of hardware failure and nonunion. Similarly, profound patient non-compliance, whether due to cognitive impairment, psychiatric illness, or substance abuse, represents a relative contraindication, as adherence to strict postoperative weight-bearing restrictions is critical for successful osteointegration.
Severe osteopenia or osteoporosis is a relative contraindication that demands careful surgical planning. While arthrodesis can still be performed, the surgeon must anticipate poor screw purchase and consider utilizing advanced fixation techniques, such as locking plates, longer screws that engage the diaphyseal cortical bone, or the augmentation of screw tracts with bone cement. Finally, young, highly active patients or elite athletes with early-stage hallux rigidus (Grade 1 or 2) should generally be managed with joint-sparing procedures, as the permanent loss of MTP motion associated with arthrodesis may be incompatible with the specific demands of their sport or profession.
Table: Indications and Contraindications Summary
| Category | Specific Conditions | Rationale / Considerations |
|---|---|---|
| Primary Indications | End-stage Hallux Rigidus (Grade 3/4) | Definitive elimination of painful arthritic articulation. |
| Severe/Recurrent Hallux Valgus | Provides powerful correction and stabilization of the first ray. | |
| Inflammatory Arthropathy (e.g., RA) | Addresses erosive destruction and provides a medial buttress. | |
| Failed Previous Surgery (Implants, Keller) | Restores stability and length (often requires bone grafting). | |
| Iatrogenic Hallux Varus | Corrects deformity and stabilizes the incompetent joint. | |
| Absolute Contraindications | Active Local or Systemic Infection | High risk of hardware seeding and catastrophic failure. |
| Severe Peripheral Vascular Disease | Inadequate perfusion for wound healing and bone fusion. | |
| Inadequate Soft Tissue Envelope | Risk of wound breakdown over prominent hardware. | |
| Relative Contraindications | Symptomatic IP Joint Arthritis | Arthrodesis increases stress on the IP joint, exacerbating pain. |
| Severe Neuromuscular Spasticity | Excessive forces predispose to nonunion and hardware failure. | |
| Profound Osteoporosis | Compromised fixation strength; requires specialized implants. | |
| Early-Stage Disease in Young Athletes | Loss of motion may be functionally unacceptable; consider cheilectomy. |
Alternative Surgical Considerations
When evaluating a patient for first MTP pathology, the surgeon must always weigh the benefits of arthrodesis against alternative surgical options. For patients with early to moderate hallux rigidus (Coughlin and Shurnas Grades 1 and 2), where the primary pathology is dorsal impingement and the central articular cartilage remains largely intact, a cheilectomy is the procedure of choice. This involves the resection of the dorsal 25% to 30% of the metatarsal head along with the impinging osteophytes, effectively decompressing the joint and restoring dorsiflexion while preserving the native articulation.
In highly selected, older, sedentary patients with severe hallux rigidus who cannot tolerate the prolonged recovery or non-weight-bearing period associated with arthrodesis, a Keller excisional arthroplasty may be considered. This procedure involves the resection of the base of the proximal phalanx, decompressing the joint via shortening. However, the Keller procedure is fraught with complications, including a "cock-up" deformity, loss of hallux purchase, and significant transfer metatarsalgia due to the complete loss of the windlass mechanism. It is rarely utilized in modern orthopedic practice outside of specific, low-demand scenarios.
Interpositional arthroplasty, utilizing autologous tissue (e.g., joint capsule or Achilles tendon allograft) to resurface the resected joint surfaces, is another alternative. While it preserves some motion, the results are often unpredictable, and patients frequently experience progressive joint space narrowing, recurrent pain, and eventual failure requiring conversion to arthrodesis. Synthetic joint replacements (silicone or metallic hemiarthroplasties/total joints) have historically yielded poor long-term results, plagued by high rates of osteolysis, implant subsidence, and mechanical failure.
Ultimately, while alternatives exist, first MTP arthrodesis remains the most reliable, durable, and predictable operation for end-stage forefoot pathology. It boasts a patient satisfaction rate consistently exceeding 90% in the literature. The surgeon's primary responsibility is to ensure accurate patient selection, meticulously execute the surgical technique to optimize alignment and fixation, and manage patient expectations regarding the permanent loss of MTP motion in exchange for a pain-free, stable, and functional foot.
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Diagnostic Modalities
The foundation of a successful first MTP arthrodesis is laid during
Clinical & Radiographic Imaging Archive