Comprehensive Introduction and Patho-Epidemiology
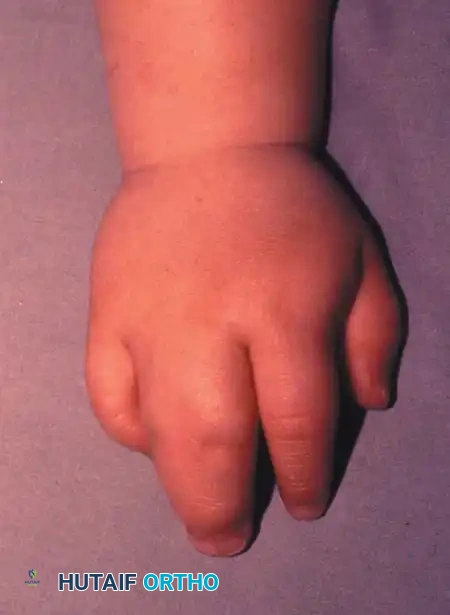
Syndactyly, fundamentally defined as the failure of adjacent digits to separate during embryological development, stands as the most frequently encountered congenital anomaly of the upper extremity. Presenting with an incidence of approximately one in 2,000 to 2,500 live births, this condition demands a profound understanding of embryology, genetics, and complex spatial biomechanics to achieve successful surgical reconstruction. The embryological insult occurs during the critical window of the seventh and eighth weeks of gestation, specifically between days 41 and 46. During normal morphogenesis, the apical ectodermal ridge (AER) and the zone of polarizing activity (ZPA) orchestrate a precise sequence of cellular events, culminating in the activation of apoptotic pathways within the interdigital mesenchymal necrotic zones. A disruption in this programmed cell death—often mediated by alterations in Sonic Hedgehog (SHH), Fibroblast Growth Factor (FGF), and Bone Morphogenetic Protein (BMP) signaling cascades—results in the persistence of the interdigital webbing.
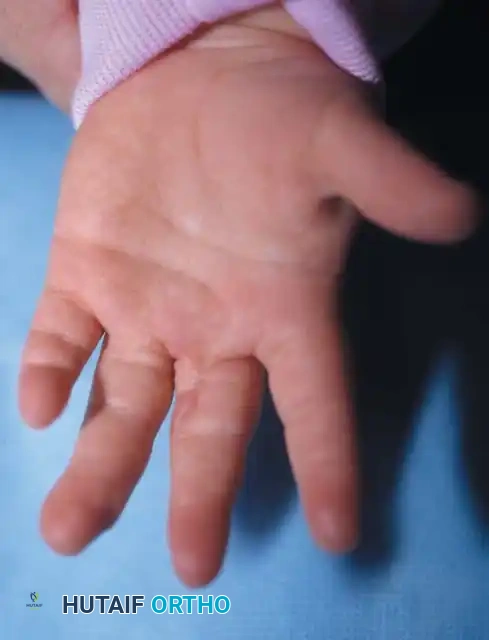
While the majority of syndactyly presentations are sporadic and isolated, the genetic underpinnings of familial cases are well-established and highly complex. Flatt’s seminal epidemiological investigations demonstrated that up to 40% of patients possess a positive family history, pointing toward a strong hereditary component. Familial syndactyly typically follows an autosomal dominant pattern of inheritance with variable phenotypic expression and incomplete penetrance. Genetic mapping has frequently implicated mutations in the HOXD13 gene on chromosome 2q31, particularly in cases of syndactyly type II (synpolydactyly). The clinical presentation is highly variable, ranging from minor cutaneous webbing bridging the proximal phalanges to devastating, multi-digit complex synostoses involving shared osseous, cartilaginous, and neurovascular elements.


A rigorous clinical evaluation of the neonate presenting with syndactyly is paramount, as this anomaly frequently serves as a harbinger for broader systemic syndromes. The surgeon must conduct a meticulous total-body examination to rule out associated congenital anomalies. Syndactyly is a hallmark feature in over 28 recognized syndromic conditions. Poland Syndrome, for instance, is characterized by unilateral brachysyndactyly combined with the ipsilateral aplasia or hypoplasia of the sternocostal head of the pectoralis major muscle. In contrast, Apert Syndrome (Acrocephalosyndactyly Type I), driven by mutations in the FGFR2 gene, presents with devastating, complex multi-digit fusions—often resulting in a "rosebud" or "spoon" hand deformity—concomitant with craniosynostosis and severe midface hypoplasia. Furthermore, the presence of acrosyndactyly (distal fusion with proximal epithelialized fenestrations) is virtually pathognomonic for amniotic constriction band sequence, an entirely distinct pathoetiological entity caused by in utero mechanical entrapment rather than a failure of primary differentiation.



Detailed Surgical Anatomy and Biomechanics
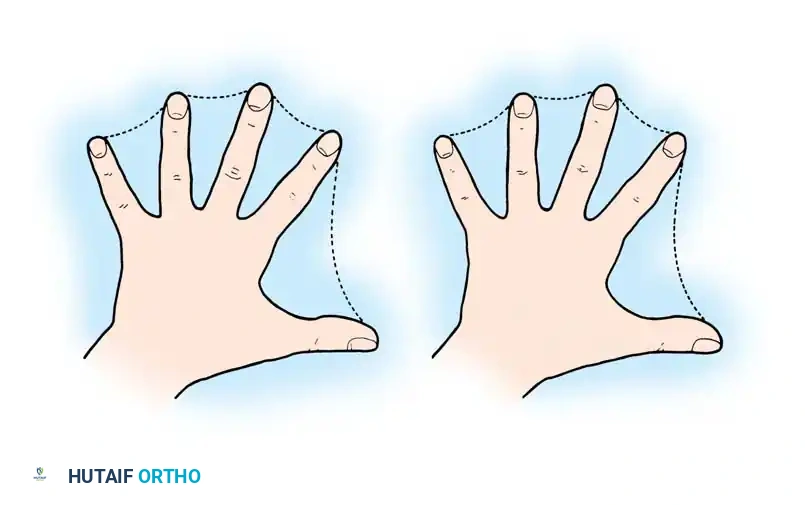
The foundational challenge of syndactyly reconstruction lies not merely in the separation of the conjoined digits, but in the mathematical reality of the geometric skin deficit. Biomechanically and geometrically, the circumference of two conjoined cylindrical digits is inherently less than the sum of the circumferences of two independent, separated digits. When the digits are surgically divided, the existing skin envelope is grossly insufficient to resurface the newly created medial and lateral borders. Attempts at primary closure under tension inevitably lead to catastrophic ischemic necrosis, severe hypertrophic scarring, and aggressive longitudinal contractures. Consequently, the surgical strategy must inherently rely on the importation of new tissue, either through full-thickness skin grafting or sophisticated local flap designs, to accommodate this immutable geometric deficit.
Beyond the cutaneous deficiency, the internal fascial, neurovascular, and musculotendinous anatomy within the syndactylized web space is frequently anomalous and treacherous. While the intervening skin may appear texturally normal, the underlying fascial structures—specifically Cleland’s and Grayson’s ligaments, as well as the natatory ligaments—are typically thickened, contracted, and abnormally oriented. These aberrant fascial bands act as unyielding tethers, restricting independent digital motion and exacerbating angular deformities during rapid phases of pediatric growth. Meticulous excision of these fascial constraints during separation is a mandatory step to restore normal digital kinematics and prevent recurrent contractures.

The neurovascular anatomy in syndactyly demands the highest degree of surgical vigilance. The common digital nerve frequently exhibits a delayed bifurcation, splitting far distal to the normal commissure, sometimes extending to the level of the distal interphalangeal joint. During separation, the surgeon must perform a meticulous, intra-neural longitudinal micro-dissection to split the common nerve into its proper digital components, preserving sensation to both adjacent borders. Arterial anomalies are equally perilous. The proper digital arteries may be entirely absent, hypoplastic, or arise from a distally bifurcating common digital artery. In instances where a distal arterial bifurcation prevents adequate separation, the surgeon must carefully evaluate the vascular dominance of each digit. Ligation of an anomalous redundant branch may be necessary to achieve separation, but this must only be performed after confirming robust collateral perfusion via the contralateral digital artery, typically utilizing intraoperative microvascular clamps and tourniquet deflation.
The osseous anatomy in complex syndactyly introduces an additional layer of profound biomechanical complexity. Shared cartilaginous or bony elements, ranging from subtle distal phalangeal tuft synostoses to massive, branching interosseous fusions, dictate the necessity and trajectory of intraoperative osteotomies. Furthermore, the presence of associated osseous anomalies, such as a delta phalanx (longitudinally bracketed epiphysis), will drive progressive, multi-planar angular deformities. Even in simple syndactyly, tethering digits of unequal lengths (e.g., the ring and small fingers) forces the longer digit to conform to the growth trajectory of the shorter digit, resulting in severe flexion contractures, rotational malalignment, and lateral deviation. This differential growth tethering is the primary biomechanical driver dictating the urgency of surgical intervention in border digit syndactylies.
Exhaustive Indications and Contraindications
The decision-making matrix for syndactyly reconstruction is governed by the specific digits involved, the complexity of the fusion, and the patient's age. Surgical intervention is inherently elective in the sense that it is a reconstructive procedure, yet it is highly time-sensitive. The overarching goal is to achieve functional independence of the digits while preventing irreversible secondary osseous and joint deformities. The timing of the release is the most critical strategic decision the orthopedic surgeon must make, balancing the risks of early surgery (anesthesia risks, smaller anatomical structures, higher rates of web creep) against the risks of delayed surgery (permanent angular deformities, joint contractures).
For central digits (the second and third web spaces, involving the index-long and long-ring fingers), the digits are of relatively equal length. Consequently, the differential growth tethering effect is minimal. In these cases, the definitive recommendation is to delay surgical release until the child is between 18 and 24 months of age. Kettlekamp and Flatt, alongside numerous subsequent longitudinal studies, have conclusively demonstrated that delaying surgery until this age significantly improves the final aesthetic and functional appearance of the reconstructed commissure. The anatomical structures are larger, making precise flap elevation and neurovascular dissection safer, and the incidence of post-operative "web creep" (the distal migration of the commissure due to differential growth between the scar tissue and the surrounding normal tissue) is drastically reduced.
Conversely, syndactyly involving the border digits (the first web space between the thumb and index finger, and the fourth web space between the ring and small fingers) constitutes a surgical urgency. Because these adjacent digits possess vastly different intrinsic lengths and growth rates, the shorter digit acts as an unyielding tether. If left unreleased, the longer digit will rapidly develop severe, irreversible flexion, rotational, and lateral deviation deformities. Therefore, complete syndactylies of the border digits must be released early, typically between 6 and 12 months of age. The imperative to prevent permanent joint and osseous deformity completely supersedes the increased risk of web creep associated with early intervention.
| Clinical Scenario | Indication / Contraindication | Rationale / Biomechanical Consequence |
|---|---|---|
| Border Digit Syndactyly (Thumb-Index, Ring-Small) | Absolute Indication for Early Release (6-12 months) | Prevents severe angular, rotational, and flexion deformities caused by the differential longitudinal growth rates of unequal digits. |
| Central Digit Syndactyly (Index-Long, Long-Ring) | Indication for Delayed Release (18-24 months) | Digits are of equal length, minimizing tethering risk. Delaying surgery reduces the incidence of web creep and allows for technically safer dissection of larger structures. |
| Simultaneous Bilateral Release of a Single Digit | ABSOLUTE CONTRAINDICATION | Operating on both the radial and ulnar sides of a single digit simultaneously jeopardizes the bilateral digital arterial supply, risking catastrophic ischemic necrosis and auto-amputation of the finger. |
| Complex Synostosis with Non-Functional Ray | Relative Contraindication for Separation | If separation will result in a flail, insensate, or mechanically useless digit, amputation or ray resection may be functionally superior to a complex, multi-staged separation attempt. |
| Mild Incomplete Simple Syndactyly | Relative Indication / Elective | If the webbing does not cross the PIP joint and causes no functional impairment, surgery is primarily cosmetic and may be deferred or avoided based on shared decision-making. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful syndactyly reconstruction. The clinical evaluation must precisely document the extent of the webbing, the presence of active and passive range of motion in all involved joints, and the apparent length and alignment of the digits. High-quality, multi-planar plain radiographs of the hand are mandatory to delineate the osseous anatomy, identify synostoses, detect delta phalanges, and evaluate the presence of supernumerary digits (synpolydactyly). In complex syndromic cases, such as Apert syndrome, advanced imaging modalities like MRI or high-resolution ultrasound may be deployed to map aberrant musculotendinous insertions and complex neurovascular arborizations prior to the initial incision.
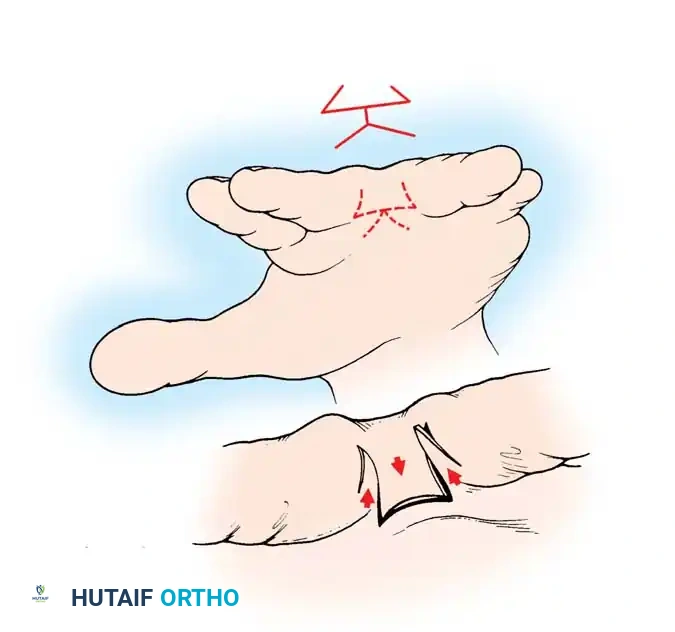
The selection of the surgical technique and the precise design of the local flaps must be templated pre-operatively. The surgeon must choose between various commissuroplasty designs, such as the classic dorsal "pantaloon" flap (Bauer, Tondra, and Trusler), proximally based V-flaps (Cronin and Skoog), or the butterfly flap (Shaw, Woolf, and Broadbent). The dorsal rectangular flap remains the workhorse for recreating the normal dorsal-to-palmar slope of the web space. The surgeon must also plan the donor site for the anticipated full-thickness skin grafts (FTSG). The groin (specifically the lower abdominal crease) is the most common donor site, providing ample, pliable skin that can be closed primarily with minimal cosmetic morbidity. Alternative sites include the hypothenar eminence (for ideal color match in small defects), the medial plantar instep, or the antecubital fossa. Split-thickness skin grafts (STSG) are generally avoided due to their high propensity for secondary contracture, which severely compromises the reconstructed web space.
Patient positioning and intraoperative setup are critical for executing these precise microvascular techniques. The pediatric patient is positioned supine with the operative extremity extended on a radiolucent hand table. General anesthesia is mandatory. A well-padded pediatric pneumatic tourniquet is applied to the upper arm. Exsanguination is achieved via elevation or a sterile Esmarch bandage, and the tourniquet is inflated to appropriate pediatric pressures (typically 50-75 mmHg above systolic blood pressure, not exceeding 200 mmHg). The use of high-powered loupe magnification (minimum 3.5x to 4.5x) or an operating microscope is absolute necessity for the safe identification and micro-dissection of the digital nerves and arteries. The surgeon must also ensure that all necessary micro-instruments, including fine tenotomy scissors, micro-forceps, and vessel loops, are readily available on the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
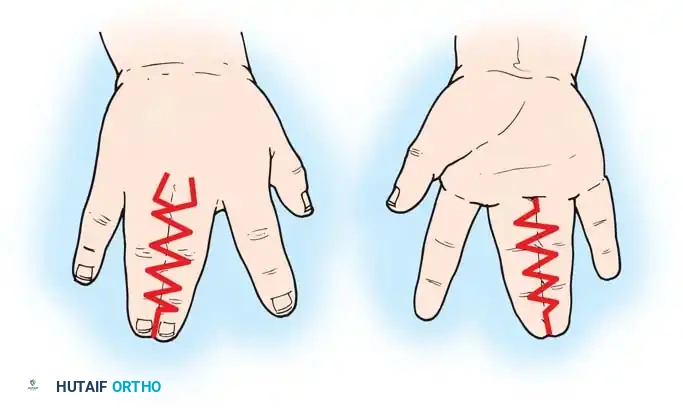
The surgical execution of syndactyly release demands uncompromising precision. The fundamental objectives are the safe separation of the digits, the anatomical reconstruction of the commissure, and the tension-free resurfacing of the resultant skin defects. The classic approach utilizing a dorsal rectangular flap combined with interdigitating zigzag incisions (Technique of Bauer et al.) remains the gold standard for most presentations.
1. Incision Design and Marking:
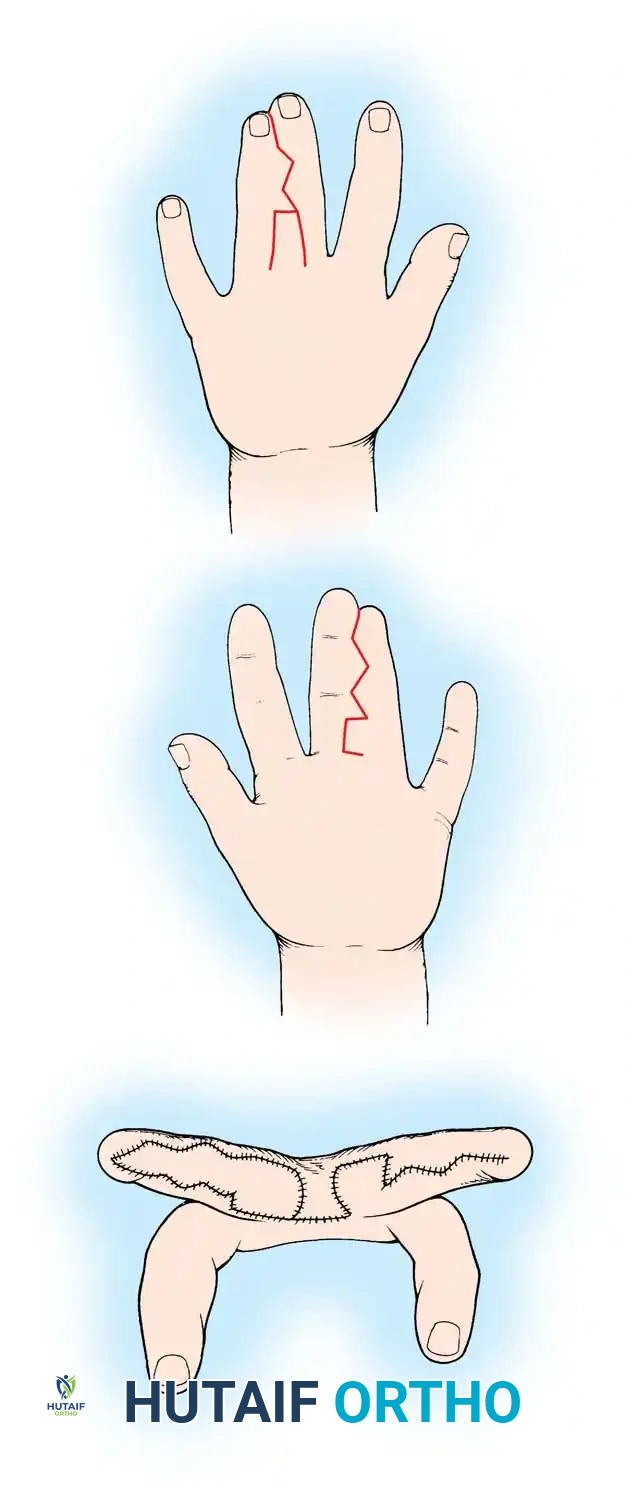
Prior to exsanguination, all incisions are meticulously drawn using a fine sterile skin marker. A dorsal rectangular flap is designed with its base at the level of the metacarpal heads, extending distally to approximately two-thirds the length of the proximal phalanx. This flap will be transposed volarly to recreate the sloping floor of the new web space. On the volar aspect, a corresponding proximal V-shaped or rectangular flap is designed, terminating just proximal to the adjacent normal commissures. Along the longitudinal axes of the conjoined digits, a series of interdigitating triangular flaps (zigzag incisions) are marked. These apices must be carefully aligned so that the flap from one digit will interdigitate with the defect on the adjacent digit, effectively breaking up the linear scar and preventing longitudinal contracture.

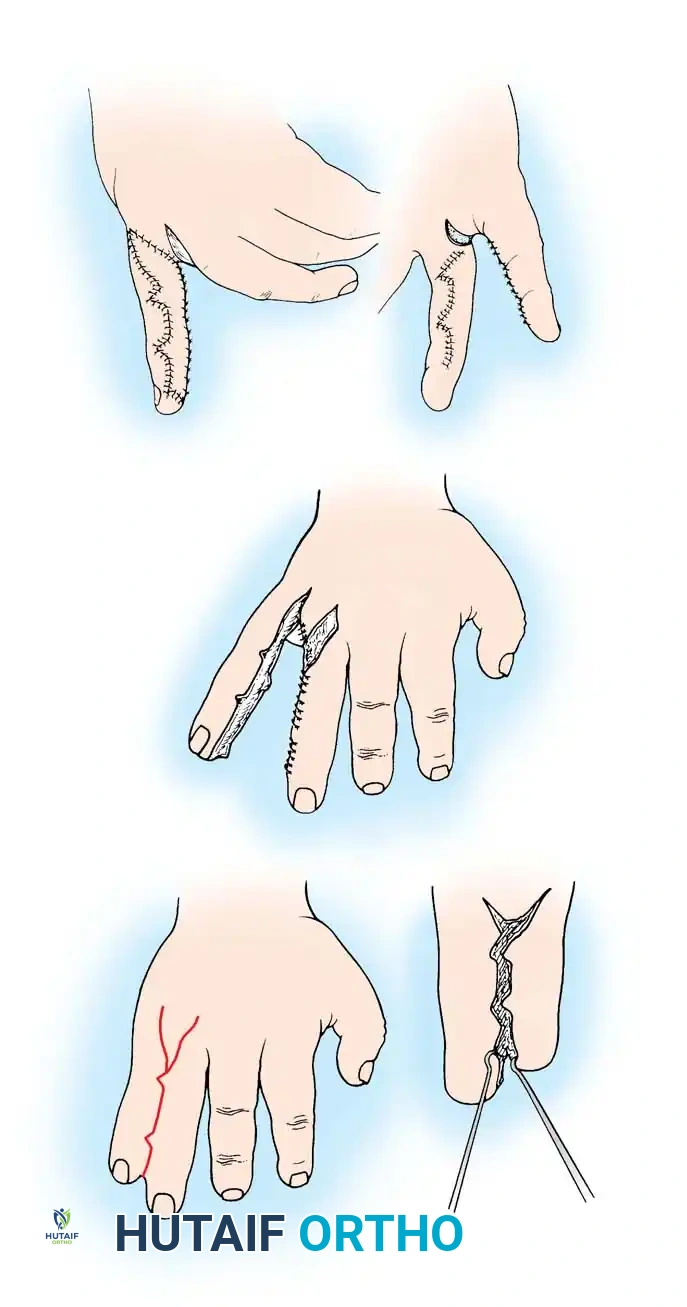
2. Flap Elevation and Neurovascular Dissection:
Under tourniquet control and loupe magnification, the incisions are made through the dermis. The dorsal rectangular flap is elevated in a plane just superficial to the extensor paratenon. The proximal portion of this flap is carefully defatted to ensure it can fold smoothly into the web space without excessive bulk. The volar and zigzag flaps are similarly elevated, preserving as much subcutaneous fat as possible within the flaps to maintain their delicate microvascular perfusion. As the dissection proceeds proximally into the web space, the neurovascular bundles are identified. The common digital nerve is isolated and traced distally. If it bifurcates distal to the planned commissure, it is meticulously split longitudinally along its internal fascicular planes using micro-scissors, ensuring that each digit retains its proper digital nerve branch. The arterial anatomy is then assessed. If a common digital artery bifurcates distally and tethers the separation, the surgeon must confirm the presence of adequate collateral flow to both digits before selectively ligating the redundant or anomalous branch.
3. Digital Separation and Osseous Management:
The digits are separated completely from distal to proximal. Any thickened, abnormal fascial bands (Cleland's and Grayson's ligaments) are sharply excised to release tethering. In cases of complex syndactyly, shared osseous elements are addressed at this stage. Distal tuft synostoses are sharply divided with a micro-osteotome or heavy scalpel. If significant collateral ligament instability is created during the osteotomy, temporary stabilization with a fine smooth Kirschner wire (0.028 or 0.035 inch) may be required, though this is rare in simple syndactylies.
4. Commissure Reconstruction and Flap Inset:
The dorsal rectangular flap is transposed through the newly created web space and sutured to the apex of the volar defect using fine absorbable sutures (e.g., 5-0 or 6-0 chromic gut or Vicryl Rapide). This critical step establishes the normal dorsal-to-palmar slope and width of the commissure. The interdigitating zigzag flaps along the medial and lateral borders of the digits are then loosely tacked into position. It is imperative that these flaps are inset with absolute zero tension.
5. Skin Grafting vs. Open Technique:
Because of the geometric skin deficit, substantial raw areas will remain along the digital borders. In the classic technique, these defects are meticulously templated. Full-thickness skin grafts are harvested from the pre-planned donor site (e.g., groin), completely defatted to the level of the white dermis, and sutured into the defects. The grafts must be precisely tailored; redundant graft tissue will wrinkle and fail, while undersized grafts will cause tension and contracture.
Alternatively, the Open Finger Syndactyly Release (Technique of Withey et al.) avoids skin grafting entirely. In this innovative approach, numerous narrow, interdigitating flaps are designed and elevated without defatting. After digital separation and commissure reconstruction, the flaps are tacked at their apices, and the intervening raw areas are intentionally left open to heal by secondary intention. Extensive comparative studies have demonstrated that this open technique yields superior scar quality, eliminates donor site morbidity, and significantly reduces the incidence of late web contracture compared to traditional closed grafting techniques.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, syndactyly reconstruction carries a significant complication profile, primarily driven by the biological behavior of pediatric scar tissue and the inherent vascular fragility of the reconstructed digits. The most common and frustrating complication is "web creep," defined as the distal migration of the reconstructed commissure. This occurs due to a combination of longitudinal scar contracture and the differential growth rate between the grafted/scarred tissue and the adjacent normal digital skeletal growth. Web creep effectively recreates a partial syndactyly, often necessitating secondary revision surgeries (Z-plasties or additional flap reconstructions) as the child approaches skeletal maturity.
Vascular complications, while less frequent, are devastating. Ischemic necrosis of a digit can occur due to overzealous arterial ligation, excessive tension on the skin flaps, or the catastrophic error of performing simultaneous bilateral releases on a single digit. If intraoperative ischemia is noted upon tourniquet deflation, all sutures must be immediately removed, and the digit allowed to perfuse. If perfusion does not return, topical vasodilators (e.g., papaverine) and warm saline should be applied. In cases of irreversible thrombosis, microvascular vein grafting may be attempted, but salvage rates in infants are exceedingly low.
Graft failure is another significant complication, typically resulting from inadequate defatting of the FTSG, hematoma formation beneath the graft, or shear forces due to inadequate post-operative immobilization. Partial graft loss can often be managed conservatively with non-adherent dressings, allowing the area to heal by secondary intention. However, complete graft loss usually leads to severe hypertrophic scarring and aggressive flexion contractures, requiring delayed excision and re-grafting once the scar has matured.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Web Creep (Distal Migration) | 10% - 30% | Scar contracture, differential skeletal growth, use of STSG instead of FTSG, early age at surgery (<18 months). | Prevent with FTSG and robust dorsal flaps. Salvage with secondary Z-plasty or specialized local advancement flaps (e.g., V-Y advancement) near skeletal maturity. |
| Graft Failure / Necrosis | 5% - 10% | Inadequate graft defatting, hematoma, shear forces, infection. | Prevent with meticulous hemostasis and rigid long-arm casting. Salvage partial loss with secondary intention healing; complete loss requires delayed re-grafting. |
| Digital Ischemia / Loss | < 1% | Simultaneous bilateral release, aggressive arterial ligation, excessive flap tension. | NEVER perform simultaneous bilateral release. Intraoperative salvage: release all sutures, apply warm saline/papaverine. Late salvage: amputation. |
| Hypertrophic Scarring / Contracture | 5% - 15% | Linear incisions crossing joints, genetic predisposition, graft failure. | Prevent with precise zigzag incisions (Pieri principle). Manage with prolonged silicone sheeting, massage, and serial splinting. Surgical release for severe functional deficits. |
| Nail Deformity | Variable | Damage to the germinal matrix during separation of complex distal synostoses. | Prevent with meticulous micro-dissection of the paronychial folds. Salvage is difficult; may require composite grafting or nail bed reconstruction. |
Phased Post-Operative Rehabilitation Protocols
The immediate post-operative management is as critical to the success of the reconstruction as the surgical execution itself. The primary objective in the initial phase is the absolute immobilization of the hand to prevent shear forces across the newly inset flaps and skin grafts. At the conclusion of the procedure, a meticulous, bulky, non-adherent compressive dressing is applied. Layers of sterile Xeroform or Adaptic are placed directly over the grafts and incisions, followed by fluffed sterile gauze carefully packed into the newly created web spaces to maintain abduction and prevent maceration.
In the pediatric population, standard short-arm splints are notoriously ineffective, as infants and toddlers will quickly pull them off, destroying the delicate grafts. Therefore, the dressing must be incorporated into a rigid, long-arm cast extending from the proximal palmar crease to the proximal third of the humerus, with the elbow flexed at 90 degrees. This "anti-removal" cast ensures absolute immobilization of the hand and prevents the child from using the contralateral hand to dismantle the dressings.
The initial cast and dressings are typically left undisturbed for 2 to 3 weeks. The first dressing change is a critical event and, in young or uncooperative children, should be performed under conscious sedation or light general anesthesia in the operating room or a controlled clinic environment. This prevents sudden movements that could avulse newly adherent grafts. Once the cast is removed, the viability of the flaps and grafts is assessed. If healing is progressing appropriately, the child is transitioned to a removable thermoplastic splint, maintaining the digits in abduction and extension, to be worn primarily at night.
The secondary phase of rehabilitation focuses on scar management and the restoration of full active and passive range of motion. Parents are instructed to perform gentle, daily scar massage using emollient creams once the incisions are fully epithelialized. The use of custom-molded silicone gel sheeting or elastomer inserts within the web space is highly recommended to flatten hypertrophic scars and mitigate the early forces of web creep. Occupational therapy plays a vital role in guiding play-based activities that encourage independent digital movement and fine motor skill development. Long-term clinical and radiographic follow-up is mandatory, typically on an annual basis, to monitor for the late development of angular deformities or clinically significant web creep until the child reaches complete skeletal maturity.
Summary of Landmark Literature and Clinical Guidelines
The evolution of syndactyly reconstruction is deeply rooted in several landmark epidemiological and surgical studies that continue to dictate modern clinical guidelines.
Flatt (1977): In his foundational epidemiological work, Adrian Flatt established the baseline incidence and genetic patterns of congenital hand anomalies. His documentation of a 40% familial inheritance rate in syndactyly, alongside the detailed mapping of web space frequency (long-ring > index-long > thumb-index), remains the definitive demographic reference in pediatric hand surgery.
Kettlekamp and Flatt (1961): This critical study evaluated the timing of syndactyly release and its correlation with post-operative web creep. They conclusively demonstrated that delaying the release of central digits (where length discrepancies are minimal) until 18 to 24 months of age significantly reduced the incidence of scar contracture and distal web migration, establishing the modern clinical guideline for surgical timing.
Pieri (1949): Pieri revolutionized the surgical approach by introducing the concept of interdigitating zigzag incisions. Prior to his work, straight longitudinal incisions were standard, leading to disastrous, unyielding flexion contractures. The "Pieri principle" of breaking up linear scars remains an absolute, non-negotiable standard in all modern syndactyly releases.
Bauer, Tondra, and Trusler (1956): These authors described the classic dorsal rectangular "pantaloon" flap for commissure reconstruction. Their biomechanical insight that the normal web space requires a robust, non-grafted dorsal-to-palmar slope fundamentally changed flap design and remains the most widely utilized technique globally.
Withey et al. (2001): Challenging the dogma of mandatory skin grafting, Withey and colleagues published their long-term outcomes utilizing the "open
