Syndactyly: Principles of Surgical Reconstruction and Management
Key Takeaway
Syndactyly is the most common congenital hand anomaly, resulting from a failure of digital differentiation during the seventh and eighth weeks of gestation. Successful management requires meticulous surgical planning, precise flap design, and appropriate timing to prevent angular deformities and web creep. This guide details the pathoanatomy, classification, and step-by-step surgical techniques—including dorsal flap commissuroplasty and open release methods—to achieve optimal functional and aesthetic outcomes in pediatric patients.
Introduction to Failure of Differentiation: Syndactyly
Syndactyly, colloquially referred to as “webbed fingers,” represents a failure of the digits to separate during embryological development. Recognized as the most common congenital anomaly of the upper extremity, it occurs with an incidence of approximately one per 2,000 live births. The precise etiology remains multifactorial; however, it is fundamentally driven by an abnormal cessation or slowing of apoptosis (programmed cell death) within the interdigital necrotic zones of the finger buds during the seventh and eighth weeks of gestation.
While the majority of syndactyly cases present as sporadic, isolated occurrences, genetic predispositions are well-documented. Flatt’s seminal epidemiological studies revealed a family history of syndactyly in 40% of his patient cohort, strongly implicating heredity as a primary factor. Several pedigrees demonstrate an autosomal dominant inheritance pattern, particularly for syndactyly involving the long and ring fingers, though phenotypic penetrance is frequently incomplete.
Clinical Pearl: When evaluating a neonate with syndactyly, a comprehensive physical examination is mandatory. Anomalies frequently associated with syndactyly include webbing of the toes, polydactyly, amniotic constriction band syndrome, brachydactyly, cleft feet, hemangiomas, muscular aplasia, spinal deformities, pectus excavatum (funnel chest), and congenital cardiac defects.
Pathoanatomy and Classification
Syndactyly is classified based on the extent of the webbing (complete vs. incomplete) and the anatomical structures involved (simple vs. complex).
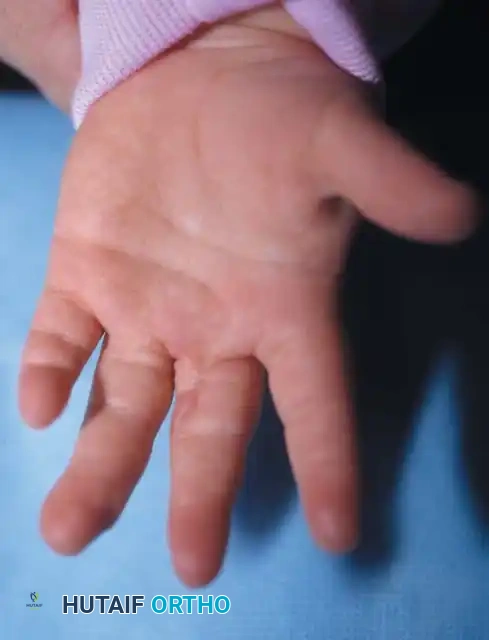
- Complete Syndactyly: The digits are joined seamlessly from the interdigital web space to the distal fingertips.
- Incomplete Syndactyly: The digits are joined from the web space to a variable point proximal to the fingertips.
- Simple Syndactyly: The bridging tissue between the digits consists exclusively of skin and soft tissue fascial bands. The phalanges remain distinct and separate.
- Complex Syndactyly: The involved digits share common osseous or cartilaginous elements. This can range from minor distal phalangeal fusions to intricate, branching interosseous synostoses.


Fig. 76-33 Simple syndactyly. Fingers are bridged only by skin and other soft tissues. A, Palmar view. B, Dorsal view. C, Radiograph. Note the angular deformity of the ring finger.

Fig. 76-34 Complex syndactyly. Common bony elements are shared by the involved fingers, necessitating precise osteotomies during separation.
Specialized Terminology
- Acrosyndactyly: Refers to the lateral fusion of adjacent digits exclusively at their distal ends, often leaving proximal fenestrations (epithelialized sinuses) between the joined digits. This is a hallmark of amniotic constriction band syndrome.
- Brachysyndactyly: Denotes an associated longitudinal shortening of the syndactylized digits.
Associated Syndromic Presentations
Syndactyly is a defining feature in several complex congenital syndromes:
- Poland Syndrome: Characterized by the unilateral absence or hypoplasia of the sternocostal head of the pectoralis major muscle. The ipsilateral hand deformity typically includes unilateral shortening of the index, long, and ring fingers; multiple simple incomplete syndactylies; and overall global hypoplasia of the hand.
- Apert Syndrome (Acrocephalosyndactyly Type I): Characteristically presents with complex, multiple syndactylies of the hands and feet (often termed a "rosebud" or "mitten" hand), alongside craniosynostosis and midface hypoplasia.



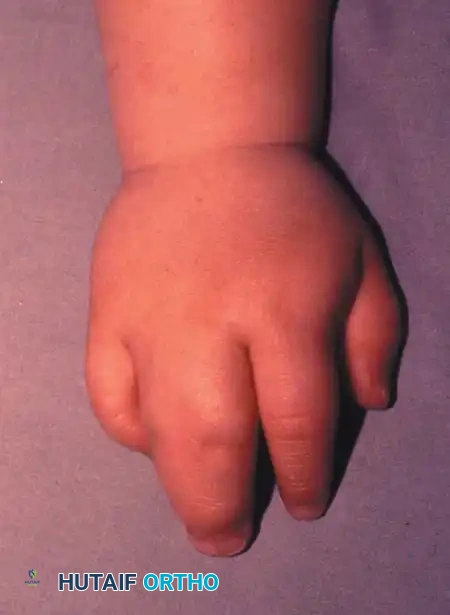
Fig. 76-35 Poland syndrome in an 18-month-old child. A and B, Brachysyndactyly. C, Hypoplasia of the pectoralis major muscle.
Epidemiology and Biomechanical Considerations
Syndactyly most frequently occurs between the long and ring fingers, accounting for more than 50% of all cases. The fourth web (ring-small), second web (index-long), and first web (thumb-index) are affected in diminishing frequencies. The anomaly is bilateral in approximately 50% of patients, with a higher prevalence in males than females.
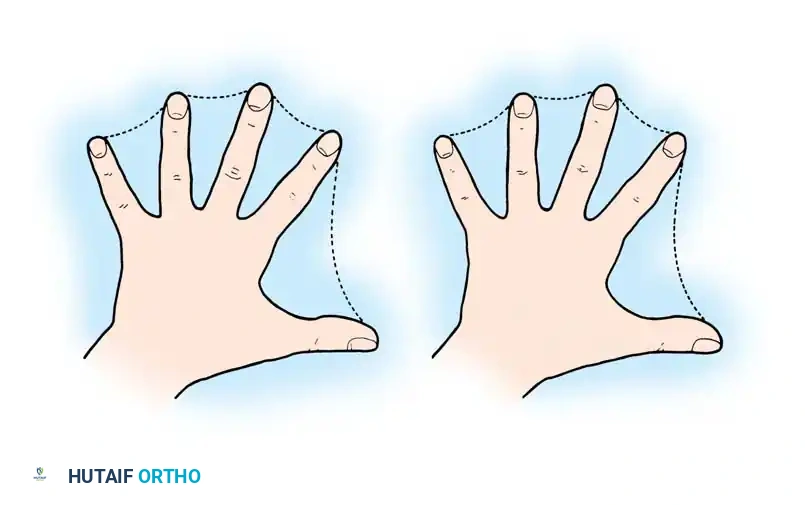
Fig. 76-36 Site of syndactyly. A, Percentage incidence when only true syndactyly of simple or complex type is considered. B, Total count incidence in which associated conditions are included.
The Geometric Skin Deficit
A critical biomechanical principle in syndactyly reconstruction is the inherent deficiency of skin surface area. The circumference of two conjoined digits is mathematically less than the sum of the circumferences of two separate, independent digits. Consequently, primary closure of both digits after separation is geometrically impossible without inducing severe tension and subsequent ischemia. This necessitates the use of skin grafts or specialized open-healing techniques.
Neurovascular and Musculotendinous Anomalies
The intervening skin is typically normal in texture, but abnormally tight fascial bands (Cleland's and Grayson's ligaments) are usually present within the web, restricting independent lateral movement. Frequently, there is anomalous arborization of the neurovascular bundles. The common digital nerve often bifurcates far distally, requiring meticulous longitudinal intra-neural splitting to preserve sensation to both digits. Similarly, common digital arteries may extend distally into the web; ligation of redundant branches must be performed with extreme caution to avoid devascularizing the digit.
Development of Angular Deformities
At birth, angular deformities are rare unless a delta phalanx is present. However, if a syndactyly tethers digits of unequal lengths (e.g., the ring and little fingers, or the index finger and thumb), the differential longitudinal growth rates will force the longer digit to develop a gradual flexion contracture, lateral deviation, and rotational deformity. This tethering effect typically manifests within the first year of life and dictates surgical timing.
Principles of Surgical Management
Surgical intervention for syndactyly is elective but highly time-sensitive based on the specific digits involved.
Timing of Surgery
- Standard Release (Long-Ring or Index-Long): If the syndactyly involves digits of relatively equal length (second or third web spaces) without complex bony fusions, surgery should be delayed until the child is at least 18 months old. Kettlekamp and Flatt demonstrated that delaying surgery until this age significantly improves the final appearance of the commissure and reduces the incidence of "web creep" (distal migration of the web space) and scar contracture.
- Early Release (Border Digits): When digits of significantly different lengths are completely involved (e.g., thumb-index or ring-small), early separation between 6 and 12 months of age is mandatory. Preventing irreversible angular, rotational, and flexion deformities takes absolute precedence over the risk of web creep.
🚨 SURGICAL WARNING: Simultaneous releases of the radial and ulnar sides of a single digit are strictly contraindicated. Operating on both sides simultaneously compromises the bilateral digital arterial supply, risking catastrophic circulatory insufficiency and ischemic necrosis of the finger. In multiple syndactylies, border digits are released first, followed by a mandatory 6-month waiting period before releasing the contralateral side of the shared digit.
Core Technical Objectives
Successful syndactyly reconstruction relies on three non-negotiable technical steps:
1. Separation of the digits: Utilizing zigzag incisions to prevent linear scar contracture.
2. Commissure reconstruction: Recreating the normal dorsal-to-palmar slope of the web space.
3. Resurfacing of the intervening borders: Utilizing full-thickness skin grafts or specialized flap designs to cover the geometric skin deficit.
Surgical Flap Design and Commissuroplasty
Early historical attempts at separation using straight linear incisions or ligatures resulted in disastrous longitudinal scar contractures. In 1949, Pieri revolutionized the approach by advocating for zigzag incisions, a principle universally applied today.
Special attention must be given to the commissure. A normal web space is not a simple V-shape; it has a sloping configuration from proximal-dorsal to distal-palmar. The distal web span must be wider than the proximal span to allow unhindered abduction around the metacarpophalangeal joint axis.
To recreate this complex geometry, local flaps are vastly superior to skin grafts, as flaps resist contracture. Commonly utilized flaps include:
* Dorsal "Pantaloon" Flap: Described by Bauer, Tondra, and Trusler.
* Proximally Based V-Flaps: Popularized by Cronin and Skoog.
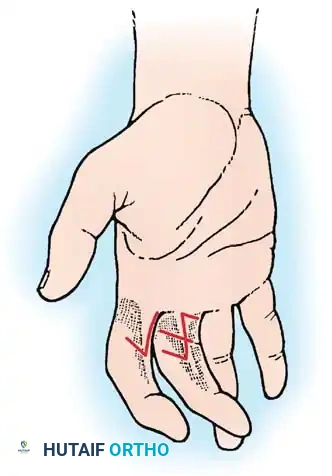
* Butterfly Flap: Devised by Shaw et al., and modified by Woolf and Broadbent, particularly useful for partial simple syndactyly ending proximal to the PIP joint.
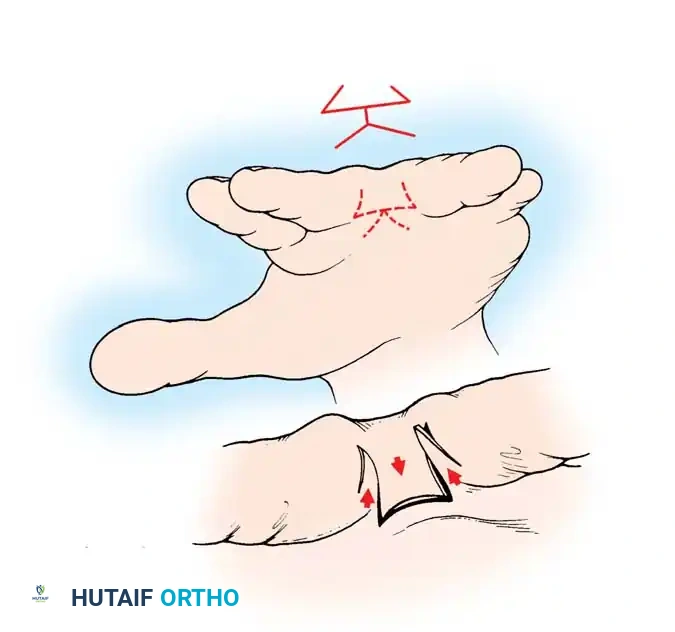
Fig. 76-37 Butterfly flap technique for release of syndactyly. Flaps are designed in the web space to form a dorsal rectangle, then rotated to deepen the web.
Skin Grafting Considerations
Because primary closure is rarely possible, skin grafting is typically required. Full-thickness skin grafts (FTSG) are generally preferred over split-thickness skin grafts (STSG). Deunk et al. demonstrated that while STSG results in higher rates of severe web contracture, FTSG carries a slightly higher risk of hyperpigmentation, hair growth, and minor web creep. Grafts should be meticulously avoided at the base of the ring finger, where the future wearing of a ring may cause chronic irritation.
Operative Techniques
Technique 76-21: Open Finger Syndactyly Release (Withey et al.)
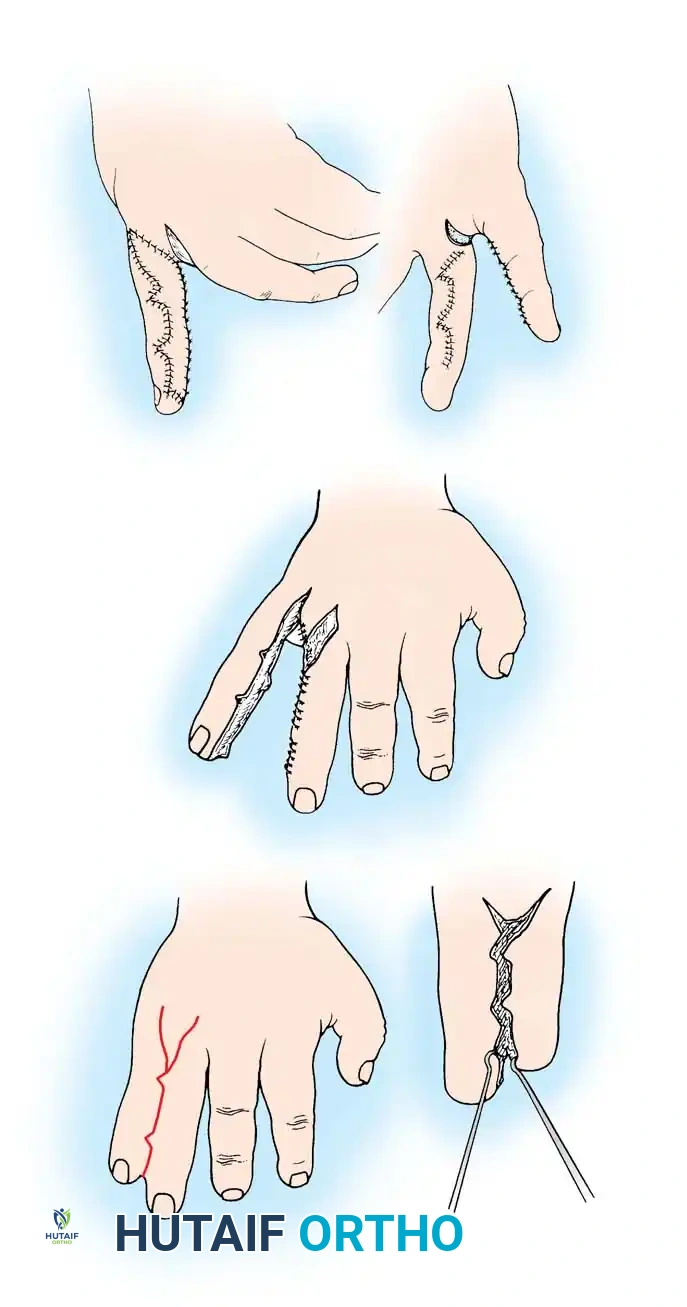
Withey et al. described an innovative "open" technique that avoids skin grafting entirely. By designing numerous, narrow interdigitating flaps and avoiding defatting, the flaps are secured without tension. The intervening raw areas are left to heal by secondary intention. Comparative studies show this method yields superior scar quality and significantly less contracture than closed grafting techniques.
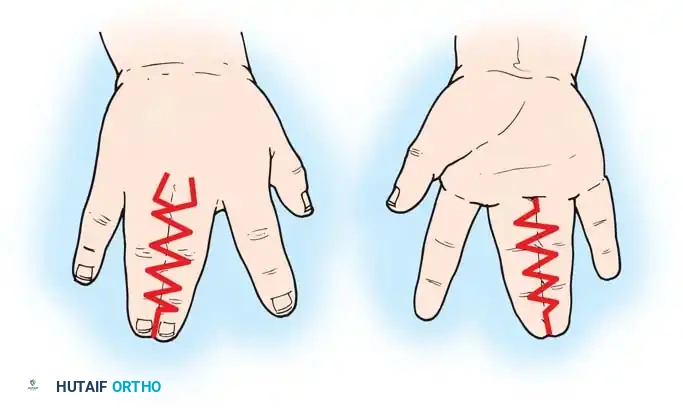
Fig. 76-38 Open technique of syndactyly release. A, Dorsal incisions. B, Palmar incisions.
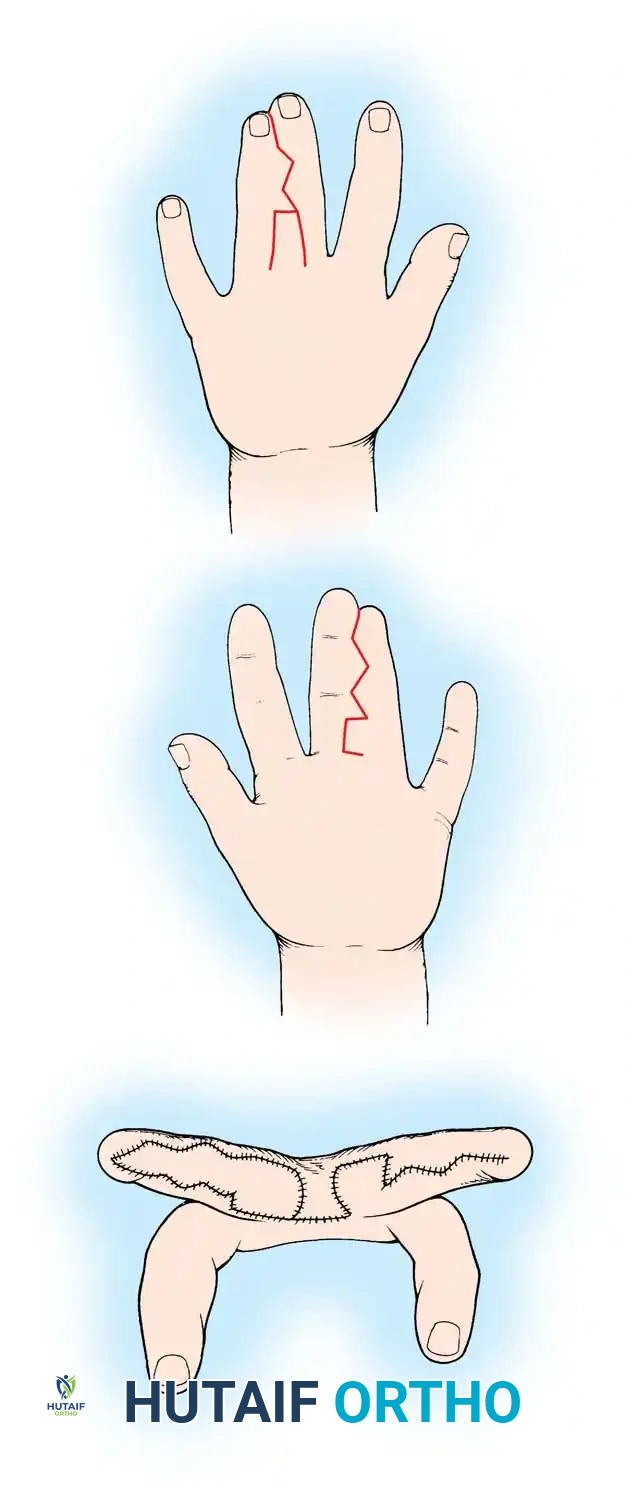
Healing progression of the open technique, demonstrating secondary intention healing without the morbidity of a donor graft site.
Step-by-Step Procedure:
1. Incision Marking: Mark the flaps as shown in Figure 76-38. Utilize a broad rectangular, proximally based dorsal flap to recreate the web commissure. Design seven or eight narrow zigzag flaps to interdigitate along the lateral borders of the fingers.
2. Flap Elevation: Raise each flap meticulously to the midaxial line. Due to the high number of flaps, each possesses a narrow base; handle tissue with atraumatic technique.
3. Vascular Preservation: Do not defat the digital flaps. Retaining the subcutaneous fat is critical to avoiding vascular compromise of these narrow-based flaps.
4. Separation: Carefully separate the digits, splitting any shared digital nerves longitudinally and ligating redundant arterial branches only if absolutely necessary.
5. Flap Inset: Tack the flaps in place using a single apical absorbable suture (e.g., 5-0 chromic gut or Vicryl Rapide). Ensure there is zero tension on the apices.
6. Secondary Intention: Leave the raw, uncovered areas between the flaps to heal by secondary intention.
7. Commissure Grafting (Optional): If the dorsal rectangular flap is insufficient to line the commissure without tension, a small split-thickness skin graft may be used exclusively at the web base.
8. Immobilization: Apply a bulky, non-adherent compressive dressing, extending above the elbow in young children to prevent removal.
Technique 76-22: Syndactyly Release with Dorsal Flap (Bauer et al.)
This is the classic, highly reliable technique utilizing a robust dorsal flap to reconstruct the web space, supplemented by full-thickness skin grafting for the lateral digital defects.

Dorsal flap design (Flap A) extending from the metacarpal heads to the proximal two-thirds of the proximal phalanx.
Palmar flap design (Flap B) with the proximal limb positioned just proximal to the adjacent normal commissures.
Step-by-Step Procedure:
1. Preoperative Marking: Outline all incisions carefully with a sterile skin-marking pen. Draw a dotted line along the central longitudinal axis of each involved digit to accurately determine the limits of the triangular zigzag flaps.
2. Dorsal Flap Design: Draw the dorsal flap ("A") so that its base begins at the level of the metacarpal heads and its apex extends distally to two-thirds the length of the proximal phalanx.
3. Palmar Flap Design: Incise the palmar flaps. The proximal limb of the palmar flap ("B") should terminate just proximal to the level of the adjacent normal commissures.
4. Dissection: Incise the dorsal flaps. Carefully defat the proximal dorsal flap to allow it to fold into the web space without bulk.
5. Neurovascular Protection: During midline separation, meticulously identify and protect the neurovascular bundles. Use loupe magnification to split shared digital nerves longitudinally.
6. Commissure Reconstruction: Remove excess dorsal fat from the newly created web space. Suture the dorsal flap ("A") into the palmar defect first. This establishes
Associated Surgical & Radiographic Imaging
You Might Also Like