Surgical Management of Complicated Nonunions
Key Takeaway
The management of complicated nonunions requires a comprehensive surgical strategy addressing infection, poor soft tissue envelopes, segmental bone loss, and complex deformities. Successful treatment hinges on radical debridement, rigid stabilization—often utilizing circular external fixation like the Ilizarov method—and meticulous restoration of the biological environment through decortication and targeted local antibiotic delivery.
Comprehensive Introduction and Patho-Epidemiology
The treatment of nonunions represents one of the most formidable and technically demanding challenges in the entirety of operative orthopaedics. A fracture transitions from a standard delayed healing process to a "complicated nonunion" when its biological and mechanical environment is compromised by one or more severe exacerbating factors. These factors include deep indolent or active infection, a profoundly deficient soft tissue envelope, short periarticular fragments that defy standard fixation, significant multidirectional angular or rotational deformity, and massive segmental bone loss. Successfully navigating these intricate pathologies requires profound clinical judgment, a mastery of local and systemic biological optimization, and advanced biomechanical stabilization techniques. The orthopedic surgeon must delicately balance the aggressive eradication of infection with the meticulous preservation of osteogenic potential, frequently employing staged reconstructive protocols, specialized local antibiotic delivery systems, and complex circular external fixation.
Considerable surgical judgment is required to treat a nonunion complicated by an infected fracture. When infection has been prolonged and destructive, all surrounding structures are presumed to be deeply penetrated, and a dormant infection is highly likely. Pathogens, most notably Staphylococcus aureus and Pseudomonas aeruginosa, possess the insidious ability to form complex extracellular polymeric biofilms. These biofilms allow bacteria to lie dormant within pocketed, avascular cortical bone (sequestrum) for years or even decades, only to reactivate following surgical intervention, altered host immunity, or subsequent trauma. This inherent danger must be explicitly accepted, anticipated, and mitigated when treating ununited open fractures. The biofilm provides a mechanical barrier against host macrophages and prevents the penetration of systemic antibiotics, rendering the infection virtually incurable without radical surgical debridement.
To standardize the approach to osteomyelitis and infected nonunions, the University of Texas Medical Branch (Cierny-Mader) Staging System is universally employed by musculoskeletal infection specialists. Unlike traditional classifications that rely solely on chronicity or etiology, this system categorizes the infection based on the dynamic interplay between anatomical involvement and the physiological status of the host. The anatomical types range from Type I (Medullary osteomyelitis) to Type IV (Diffuse osteomyelitis, characterized by circumferential involvement causing mechanical instability, which is the hallmark of the infected nonunion). The physiological class dictates the host's ability to mount a healing response: A-Hosts have normal immune and vascular function; B-Hosts are compromised either locally (BL, e.g., venous stasis, radiation fibrosis) or systemically (BS, e.g., diabetes, malnutrition, smoking); C-Hosts are severely compromised individuals for whom the surgical treatment would be worse than the disease itself.
The epidemiology of complicated nonunions is heavily skewed toward high-energy trauma, particularly open fractures of the tibial diaphysis. The tibia's precarious anteromedial soft tissue envelope, combined with its watershed blood supply, makes it uniquely susceptible to post-traumatic complications. Furthermore, the rising incidence of high-velocity motor vehicle collisions and complex periarticular fractures managed with extensive internal fixation has led to a parallel increase in iatrogenic devascularization, contributing to the prevalence of atrophic, infected nonunions. Understanding this patho-epidemiology is critical, as it dictates that the surgeon must not merely treat the bone, but rather orchestrate the resurrection of the entire composite tissue envelope.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of osseous vascular anatomy and fracture biomechanics is the absolute foundation upon which the successful treatment of a complicated nonunion is built. The diaphyseal blood supply of long bones, particularly the tibia and femur, is primarily derived from a dual system: the high-pressure endosteal nutrient artery network and the low-pressure periosteal capillary network. In the uninjured state, the endosteal system supplies the inner two-thirds of the cortex, while the periosteal system supplies the outer one-third. However, in the setting of high-energy trauma, intramedullary nailing, or aggressive surgical stripping, the endosteal supply is frequently obliterated. Consequently, the bone becomes entirely reliant on the periosteal blood supply, which is derived from the surrounding muscle bellies and fascial attachments.
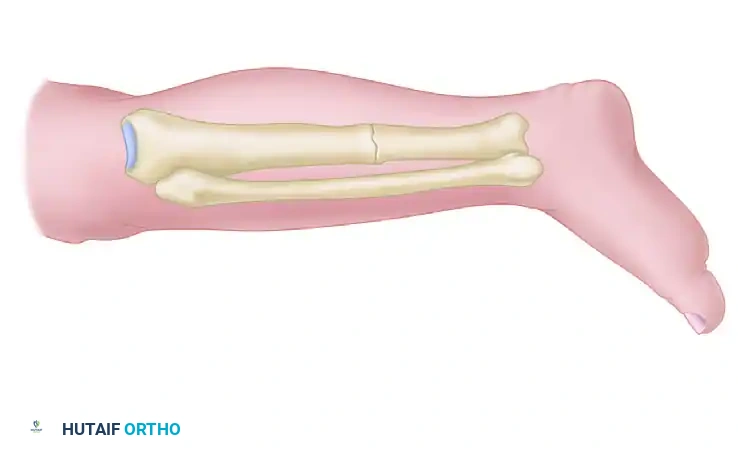
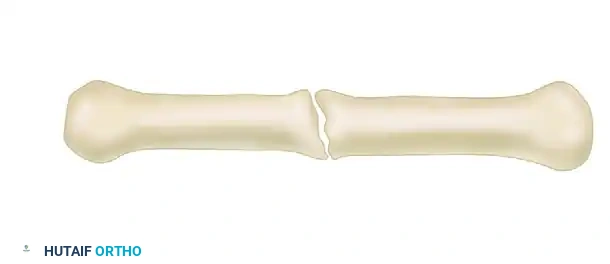
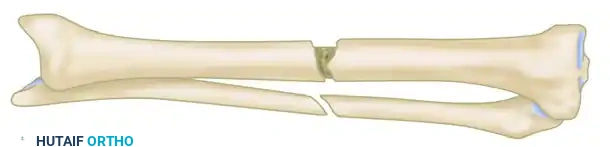
When a nonunion develops, it is fundamentally a failure of either biology or biomechanics, and frequently both. Hypertrophic nonunions are characterized by an exuberant, "elephant shoe" or "horse hoof" callus formation on radiographs. Biologically, these nonunions are highly viable and intensely vascularized; their failure to unite is purely mechanical. According to Perren’s Strain Theory, the interfragmentary strain exceeds the tolerance of woven bone formation, causing the tissue in the gap to remain as flexible fibrocartilage rather than ossifying. The treatment for a hypertrophic nonunion is therefore straightforward: provide absolute mechanical stability, typically via compression, which reduces the strain environment and allows the existing biological potential to cross the gap and achieve osseous union.
Conversely, atrophic nonunions present a much more daunting challenge. Radiographically, they appear inert, with tapered, sclerotic bone ends and an absolute absence of callus. Biologically, the fracture gap is avascular, filled with dense, poorly perfused fibrous tissue, and the adjacent bone ends are frequently necrotic. Mechanically, they are unstable, but correcting the instability alone is insufficient. The surgeon must fundamentally alter the biological environment. This requires radical resection of the avascular segments back to bleeding, healthy bone (the "paprika sign"), followed by the introduction of osteoconductive scaffolds, osteoinductive proteins (such as BMP-2 or BMP-7), and osteogenic cells (via autologous bone graft or bone marrow aspirate concentrate), combined with rigid stabilization.
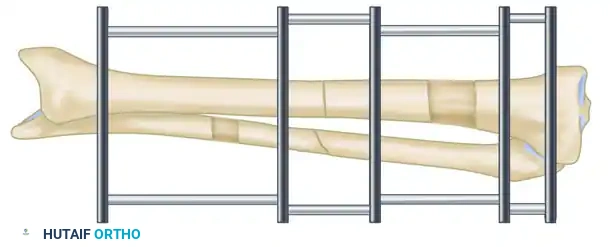
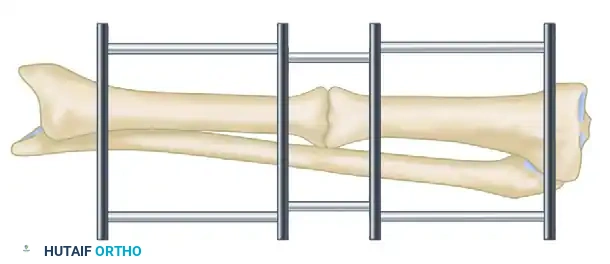
The biomechanics of external versus internal fixation also play a critical role in managing these complex scenarios. While rigid plates provide absolute stability and promote primary bone healing, they require extensive soft tissue stripping and introduce a large volume of foreign material into potentially infected beds. Intramedullary nails offer relative stability and promote secondary bone healing via callus, but reaming can further compromise endosteal blood supply and disseminate infection throughout the medullary canal. Circular external fixation (the Ilizarov method) offers a unique biomechanical environment: it provides axial dynamization while maintaining high bending and torsional stiffness. This specific mechanical milieu is highly conducive to distraction osteogenesis and the maturation of regenerate bone, making it the gold standard for managing nonunions complicated by significant bone loss or active infection.
Exhaustive Indications and Contraindications
The decision-making algorithm for treating a complicated nonunion requires a meticulous assessment of the host, the pathogen, the soft tissue envelope, and the mechanical deficiency of the bone. The indications for intervention are rarely straightforward and must be tailored to the specific physiological class of the patient. The primary indication for surgical intervention is a symptomatic, mechanically unstable nonunion that impairs the patient's functional mobility, particularly when complicated by active infection, progressive deformity, or impending pathological fracture.
Staged reconstructive protocols are strictly indicated for Cierny-Mader Type IV infections in A-Hosts or optimized B-Hosts where gross purulence, massive sequestration, or compromised soft tissue envelopes preclude immediate definitive fixation. In these scenarios, the initial stage focuses entirely on radical debridement, dead space management with local antibiotic delivery systems, and temporary stabilization. The Active Treatment Protocol (early bony continuity via decortication and external fixation) is indicated when the infection is localized, the soft tissues are relatively compliant, and the primary goal is to achieve rapid mechanical stability to harness its inherent anti-infective properties.
Contraindications to massive reconstructive efforts must be respected to avoid catastrophic outcomes, including unnecessary prolonged suffering or mortality. Absolute contraindications include C-class hosts whose systemic comorbidities (e.g., end-stage renal disease, severe cardiopulmonary compromise) make them unfit for multiple anesthetics. Additionally, a limb with an irreparable posterior tibial nerve injury, absent plantar sensation, and profound ischemic compromise is generally an absolute contraindication to limb salvage; in such cases, primary amputation is the most functional and humane reconstructive option.
| Parameter | Indications for Limb Salvage & Reconstruction | Contraindications (Consider Amputation/Suppression) |
|---|---|---|
| Host Status | Cierny-Mader A-Host or optimizable B-Host. | Cierny-Mader C-Host; severe uncorrectable malnutrition. |
| Neurological | Intact plantar sensation; functioning major motor nerves. | Irreparable sciatic or posterior tibial nerve transection. |
| Vascularity | Palpable pulses; biphasic Doppler; reconstructable vessels. | Non-reconstructable arterial tree; profound microvascular disease. |
| Soft Tissue | Amenable to local/free flap coverage; pliable skin. | Massive, unyielding circumferential scarring with no flap options. |
| Bone Loss | Any defect size if host is optimized (via transport). | Massive defects in a physiologically exhausted patient. |
| Psychological | High compliance; strong support system; realistic expectations. | Active substance abuse; severe non-compliance; psychiatric instability. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a complicated nonunion reconstruction is directly proportional to the rigor of the preoperative planning. This phase begins with the optimization of the host. Smoking cessation is an absolute prerequisite, as nicotine causes profound microvascular vasoconstriction and inhibits osteogenesis; many surgeons mandate negative serum cotinine levels prior to elective reconstruction. Glycemic control must be optimized, targeting a Hemoglobin A1c of less than 7.0%, to ensure adequate leukocyte function and soft tissue healing. Nutritional parameters, including serum albumin, prealbumin, and total lymphocyte count, must be evaluated and corrected.
Radiographic evaluation must be exhaustive. Standard orthogonal plain radiographs (anteroposterior and lateral) of the entire affected bone, including the joints above and below, are mandatory. For deformity analysis, full-length standing alignment films of both lower extremities are necessary to calculate the Mechanical Axis Deviation (MAD), the Center of Rotation of Angulation (CORA), and any leg length discrepancy. Computed Tomography (CT) with 3D reconstructions is invaluable for assessing the exact geometry of the nonunion, identifying occult sequestra, and planning the trajectory of osteotomies. Magnetic Resonance Imaging (MRI), particularly with contrast, is utilized to delineate the extent of intramedullary osteomyelitis and evaluate the viability of the surrounding soft tissue envelope.
When utilizing hexapod circular fixators such as the Taylor Spatial Frame (TSF), preoperative planning enters the digital realm. The absolute prerequisite for successful TSF application is pristine preoperative imaging. True orthogonal views of the entire limb are mandatory to determine the correct ring diameter based on preoperative sizing of the limb (allowing for at least two fingerbreadths of clearance to accommodate postoperative swelling). The surgeon must define the "mounting parameters"—the exact position of the reference ring relative to the bone in the coronal, sagittal, and axial planes. These parameters, along with the deformity parameters, are inputted into a web-based software program that generates a highly precise daily prescription for strut adjustments.
Patient positioning in the operating room must facilitate both the extensive surgical approach and unhindered fluoroscopic imaging. The patient is typically positioned supine on a completely radiolucent Jackson or OSI table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position. The entire limb is prepped and draped free, from the iliac crest (to allow for autogenous bone graft harvesting) down to the toes. The C-arm fluoroscopy unit must be able to freely rotate to obtain true AP and lateral views without moving the compromised limb, ensuring that the surgeon can continuously verify alignment, pin trajectory, and osteotomy completeness throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a complicated nonunion repair is a highly orchestrated, multi-stage endeavor that demands meticulous soft tissue handling, aggressive biological debridement, and precise biomechanical stabilization. The techniques described below represent the pinnacle of reconstructive orthopaedics.
Radical Debridement and Infection Control
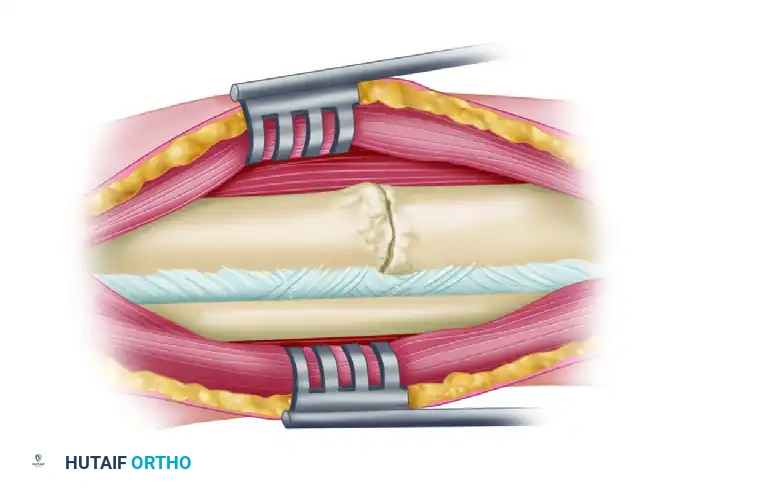
The bedrock principle of treating an infected nonunion is that antibiotics cannot sterilize avascular, necrotic bone. The operation begins with an aggressive approach through the previous surgical scars, incorporating any draining sinus tracts into the elliptical excision. The surgeon must meticulously separate the soft tissues from the underlying bone, preserving as much periosteal attachment as possible to viable fragments.
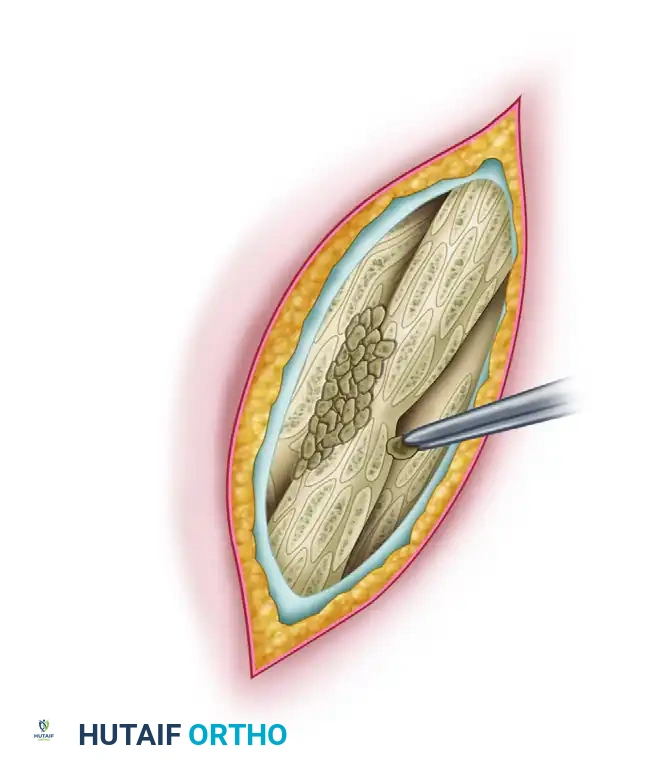
All devitalized bone, fibrous nonunion tissue, and infected soft tissues are meticulously excised using sharp osteotomes and high-speed burrs. The debridement must continue sequentially until punctate cortical bleeding—the "paprika sign"—is universally observed across all bony surfaces. This signifies that the remaining bone has adequate microvascular perfusion to support an immune response and osteogenesis. If a large segmental defect is created, the dead space must be managed. Antibiotic-impregnated Polymethyl Methacrylate (PMMA) beads or spacers are deployed to provide massive local concentrations of antibiotics (up to 200 times the systemic concentration) without systemic toxicity. Palacos cement is preferred due to its superior porosity and elution kinetics. Only heat-stable antibiotics, such as tobramycin, gentamicin, and vancomycin, are utilized.
The Active Treatment Protocol
Pioneered by Judet and Patel, and further refined by Weber and Cech, the "Active Treatment" method shifts the paradigm away from prolonged staging. The primary objective is to obtain early bony continuity, postulating that absolute bony stability is inherently a potent anti-infective measure.
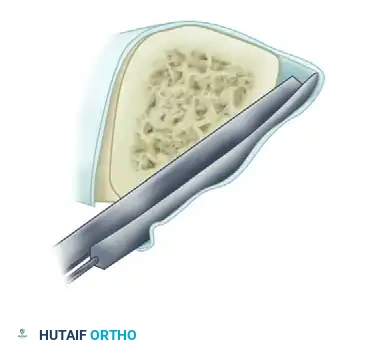
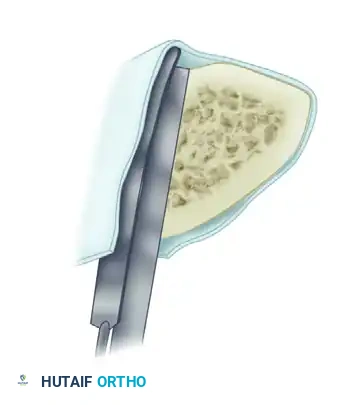
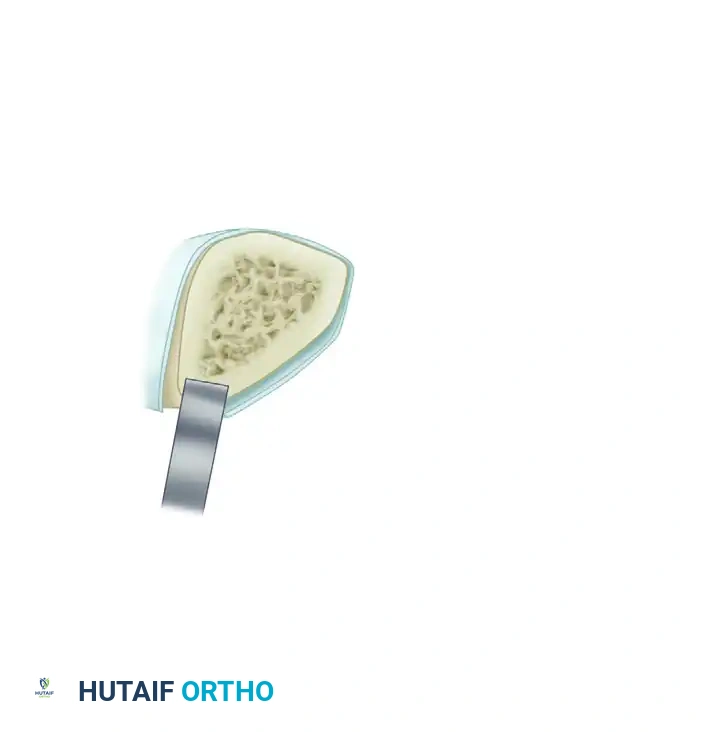
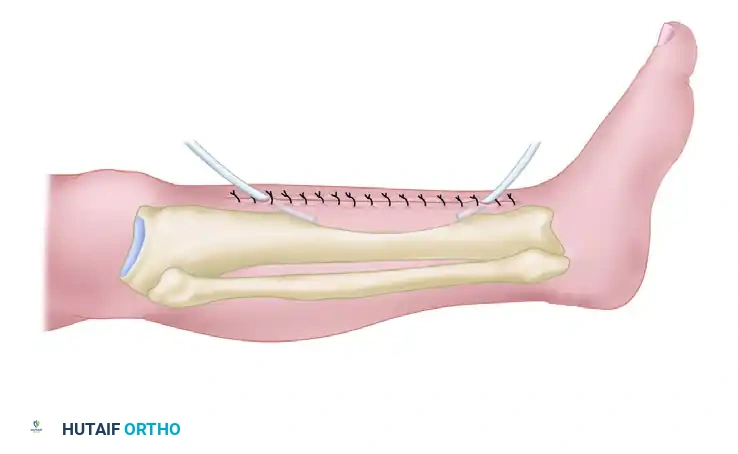
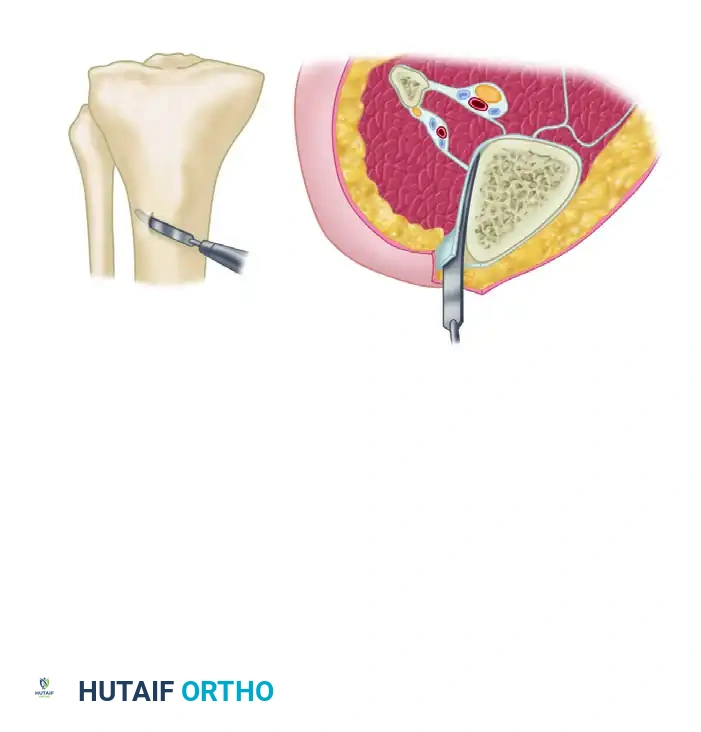
Following the radical debridement described above, the ends of the fragments are decorticated subperiosteally using a sharp, curved osteotome. This crucial step creates multiple small, vascularized osteoperiosteal grafts (shingling) that remain attached to the surrounding soft tissue envelope, effectively expanding the biological surface area of the nonunion. Any grafts that become completely detached are discarded to prevent them from acting as new sequestra. The fragments are then aligned and stabilized, predominantly utilizing an external fixation device. If the fracture geometry allows, profound axial compression is applied across the nonunion site to eliminate interfragmentary strain. Autogenous cancellous bone grafts, typically harvested from the posterior iliac crest or via the Reamer-Irrigator-Aspirator (RIA) system from the femur, are packed into any remaining defects to stimulate osteogenesis.
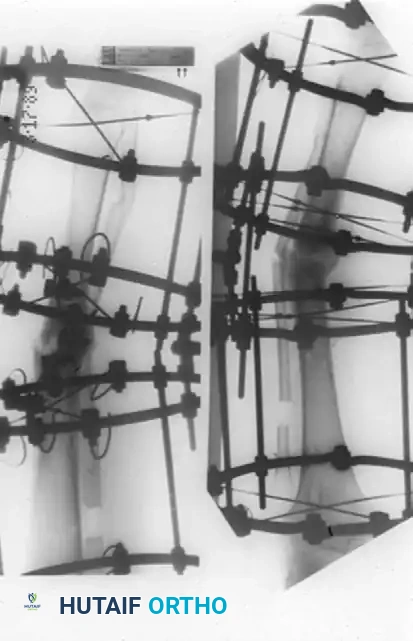
Application of Circular External Fixation (Ilizarov Method)
The management of complicated nonunions featuring multidimensional deformities, shortening, and segmental bone loss was revolutionized by Gavriil Ilizarov. The Ilizarov method is predicated on the biological principle of distraction osteogenesis—applying tension stress to living tissues to activate metabolic pathways that regenerate bone and soft tissue.
For hypertrophic nonunions with minimal infection, a Monofocal treatment mode is utilized. The inherent biology is excellent; it simply lacks stability. Compression via the Ilizarov frame provides rigid stability and stimulates the existing fibrocartilage to ossify.
Conversely, atrophic nonunions with diffuse infection or sequestered bone require a Bifocal approach. After open resection of the infected segment, the bone is acutely shortened and stabilized to allow the compromised soft tissue envelope to heal without tension.
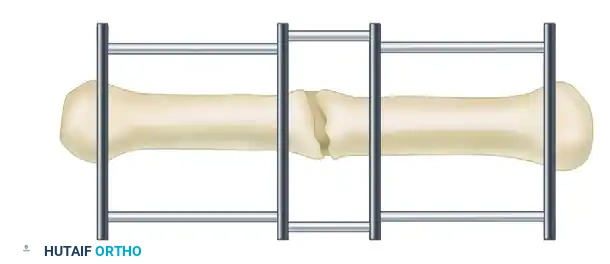
Once the infection has regressed and the skin is pristine, a low-energy metaphyseal corticotomy is performed. This is executed through a subperiosteal approach using multiple drill holes and a thin osteotome, twisting rather than levering, to preserve the endosteal and periosteal blood supply.
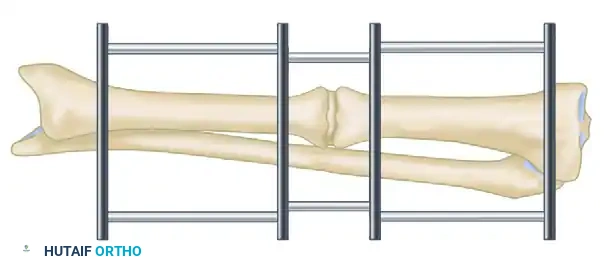
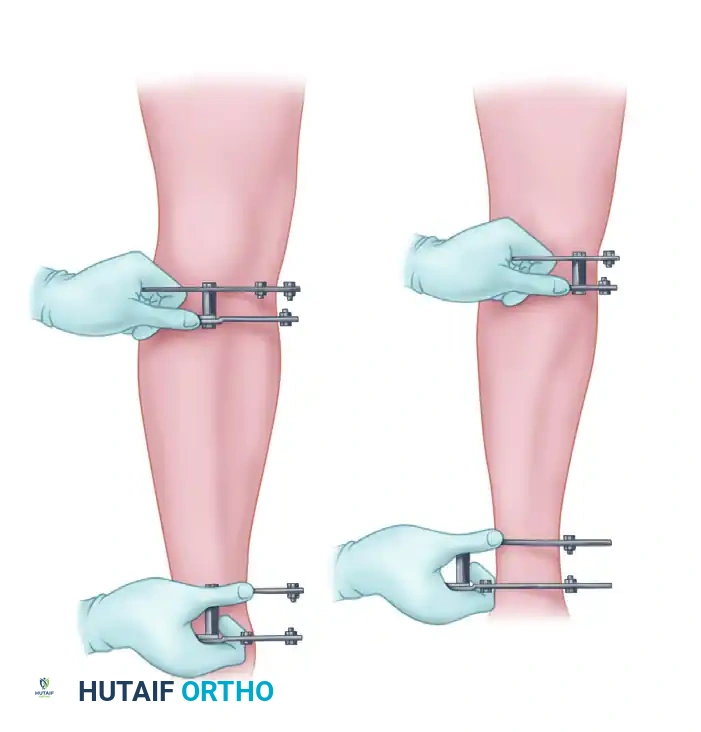
Bifocal compression-distraction is then initiated. The nonunion site is compressed to achieve union, while the corticotomy site is gradually distracted (typically at a rate of 1 mm per day, divided into four 0.25 mm increments) to restore limb length and generate new, highly vascularized bone.
For massive segmental defects, a Trifocal approach may be employed, utilizing simultaneous transport from both proximal and distal corticotomies to close the defect twice as fast, minimizing the time the patient spends in the frame.
Advanced Deformity Correction and the Taylor Spatial Frame
The Ilizarov method allows for the simultaneous correction of angular, rotary, and translational deformities. Deformities of 10 to 15 degrees can often be corrected acutely during frame application; however, larger deformities must be corrected gradually using hinges and motors to prevent tethering of neurovascular structures.

While traditional Ilizarov frames rely on complex hinge placements that can be technically unforgiving, the Taylor Spatial Frame (TSF) utilizes a Stewart platform—two rings connected by six telescopic struts. By adjusting the lengths of these six struts daily according to the software-generated prescription, the system allows for the simultaneous, gradual correction of 6-axis deformities.

The sequence of correction for complex deformities varies, but a fundamental rule is that limb length must generally be reestablished before severe angular or translational deformities are fully corrected, preventing the premature stretching of the peroneal or tibial nerves.


Bone Transport and Docking Site Management
When managing segmental bone loss via bone transport, the leading edge of the transported bone fragment (the "docking site") slowly traverses the soft tissue defect. During this journey, it frequently becomes covered in a dense cap of fibrous tissue and fibrocartilage.
Upon arrival at the principal target fragment, this docking site rarely unites spontaneously. It usually requires a secondary surgical procedure known as "docking site modification." This involves surgically opening the site, freshening the bone ends back to bleeding tissue, decorticating the adjacent cortex, and adding robust amounts of autogenous cancellous bone graft to ensure a solid, definitive bony union.
Complications, Incidence Rates, and Salvage Management
The surgical management of complicated nonunions is fraught with potential pitfalls. The extended duration of treatment, often spanning 6 to 18 months, virtually guarantees that complications will arise. The surgeon must be hyper-vigilant, adopting a proactive rather than reactive approach to complication management.
Pin tract infections are the most ubiquitous complication, occurring in up to 80% of patients undergoing circular external fixation. These are classified using the Checketts-MacKenzie system. Grades 1-3 (superficial soft tissue involvement) are managed aggressively with oral antibiotics and intensified local pin care (chlorhexidine or half-strength hydrogen peroxide). Grades 4-6 involve deep infection or osteomyelitis at the pin site, necessitating immediate pin removal, debridement of the tract, and replacement of the wire or half-pin at a distant, uninfected site to maintain frame stability.
Neurovascular compromise is a devastating complication that can occur acutely during wire insertion or gradually during deformity correction and lengthening. To mitigate acute injury, the surgeon must possess an encyclopedic knowledge of cross-sectional anatomy and safe anatomical corridors. Wires must be pushed through the soft tissues to the bone, never drilled through the soft tissues, to avoid winding up nerves or vessels. Gradual nerve stretch injuries (neuropraxia), most commonly affecting the common peroneal nerve during tibial lengthening, manifest as paresthesias or foot drop. Immediate management involves halting the distraction, or even reversing it by a few millimeters, until symptoms resolve, followed by a slower rate of distraction.
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Pin Tract Infection | 60% - 80% | Prevention: Meticulous insertion technique; low-speed drilling; daily pin care. Salvage: Oral antibiotics; pin removal/exchange for deep osteolysis. |
| Joint Contracture | 20% - 30% | Prevention: Aggressive daily physiotherapy; dynamic splinting; spanning frames across joints if necessary. Salvage: Soft tissue releases (e.g., Achilles lengthening). |
| Premature Consolidation | 5% - 10% | Prevention: Maintain consistent 1mm/day distraction rate; avoid delays in initiating distraction. Salvage: Repeat corticotomy under anesthesia. |
| Delayed Docking Site Union | 30% - 50% | Prevention: Meticulous preservation of blood supply. Salvage: Open docking site debridement; autogenous bone grafting; compression. |
| Wire/Pin Breakage | 5% - 15% | Prevention: Proper wire tensioning (130kg for olive wires); avoid excessive cantilever loading. Salvage: Immediate replacement to prevent loss of correction. |
| Psychological Burnout | 15% - 25% | Prevention: Extensive preoperative counseling; peer support groups. Salvage: Psychiatric support; temporary cessation of active transport; early frame removal and transition to internal fixation if biologically safe. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation is not an afterthought in the management of complicated nonunions; it is a critical, active component of the treatment protocol that dictates the ultimate functional outcome. The rehabilitation process is divided into distinct, highly monitored phases.
The Immediate Post-Operative Phase (Days 1-7) focuses on pain management, edema control, and the initiation of pin site care. The limb is elevated continuously. Passive and active range of motion (ROM) of all adjacent, unspanned joints is initiated immediately. For tibial frames, preventing equinus contracture of the ankle is paramount; patients are fitted with a dynamic foot splint attached to the distal ring to maintain the ankle at neutral dorsiflexion.
The Distraction/Correction Phase begins after a latency period of 7 to 10 days (to allow the corticotomy hematoma to organize into a pro-callus). Distraction typically proceeds at a rate of 1 mm per day, divided into 0.25 mm increments every 6 hours (the "rhythm" of distraction). During this phase, the soft tissues (muscles, nerves, vessels, skin) are under immense tension. Intensive, daily physical therapy is mandatory to stretch the myofascial units and prevent joint subluxation or devastating contractures. Weight-bearing is strongly encouraged, as the axial micro-motion provided by the circular frame stimulates osteoblastic activity and mechanotransduction within the regenerate bone.
The Consolidation Phase begins once the desired length and alignment have been achieved. The frame is locked, and the regenerate bone is allowed to mineralize and mature. This phase typically takes twice as long as the distraction phase. Progressive, full weight-bearing is essential during this time to promote corticalization of the regenerate. Radiographic evaluation is performed monthly, assessing the density of the regenerate bone in at least three out of four cortices.
Frame Removal and Post-Frame Protection is the final hurdle. The frame is removed only when the regenerate bone demonstrates solid corticalization and the docking site is fully united. Following removal, the bone remains temporarily osteopenic and vulnerable to bending forces. A custom-molded functional brace or cast is applied for 4 to 6 weeks, and the patient is gradually weaned off crutches to prevent a catastrophic late fracture through the regenerate or docking site.
Summary of Landmark Literature and Clinical Guidelines
The modern surgical management of complicated nonunions is built upon the shoulders of giants in the field of orthopaedics. A thorough understanding of this literature is essential for any reconstructive surgeon.
The foundational principles of distraction osteogenesis were established by Gavriil Ilizarov in the mid-20th century. His seminal papers demonstrated that tension stress applied to living tissues stimulates regeneration, provided that the blood supply is meticulously preserved via low-energy corticotomies and rigid, yet dynamic, circular fixation. Ilizarov's work shifted the paradigm from massive amputations to the biological reconstruction of massive defects.
The classification and targeted management of osteomyelitis were revolutionized by Cierny and Mader. Their staging system emphasized that the host's physiological ability to heal is just as critical as the anatomical extent of the infection. This guideline remains the gold standard for determining whether a patient is a candidate for limb salvage or requires amputation.
The "Active Treatment" protocol championed by Judet and Patel, and later expanded by Weber and Cech, established
Clinical & Radiographic Imaging Archive