INTRODUCTION TO COMPLICATED NONUNIONS
The treatment of nonunions represents one of the most formidable challenges in operative orthopaedics. A nonunion transitions from a standard delayed healing process to a "complicated nonunion" when it is compromised by one or more of the following factors: deep infection, a deficient soft tissue envelope, short periarticular fragments, significant angular or rotational deformity, and segmental bone loss.
Successfully navigating these pathologies requires profound clinical judgment, a mastery of local and systemic biological optimization, and advanced biomechanical stabilization techniques. The surgeon must balance the eradication of infection with the preservation of osteogenic potential, often employing staged reconstructive protocols, specialized local antibiotic delivery systems, and complex circular external fixation.
INFECTION: THE PRIMARY COMPLICATING FACTOR
Considerable surgical judgment is required to treat a nonunion complicated by an infected fracture. When infection has been prolonged and destructive, all surrounding structures are presumed to be deeply penetrated, and a dormant infection is highly likely. Bacteria, particularly Staphylococcus aureus, can form biofilms and lie dormant within pocketed cortical bone for years, only to reactivate following surgical intervention or subsequent trauma. This inherent danger must be accepted and mitigated when treating ununited open fractures.
The Cierny-Mader Staging System
To standardize the approach to osteomyelitis and infected nonunions, the University of Texas Medical Branch (Cierny-Mader) Staging System is universally employed. This system categorizes the infection based on anatomical involvement and the physiological status of the host.
Anatomical Type:
* Type I: Medullary osteomyelitis
* Type II: Superficial osteomyelitis
* Type III: Localized osteomyelitis (full-thickness cortical involvement but stable)
* Type IV: Diffuse osteomyelitis (circumferential involvement causing mechanical instability; typical of infected nonunions)
Physiological Class:
* A-Host: Good immune system and vascular delivery.
* B-Host: Compromised locally (BL) or systemically (BS).
* C-Host: Requires suppressive or no treatment; minimal disability; treatment is worse than the disease; not a surgical candidate.
Clinical Stage Example: Stage IVBS osteomyelitis represents a diffuse, mechanically unstable lesion in a systemically compromised host.
Clinical Pearl: The length of time since the last purulent drainage is not, in itself, a reliable index of safety for internal fixation. Reconstructive operations involving extensive internal hardware should traditionally be delayed until at least 6 months after all clinical and serological signs of infection have disappeared.
Traditional Staged Management
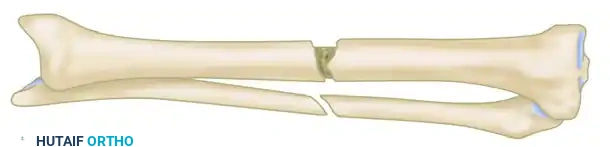
Controlling infection before attempting bone grafting has historically been a sound clinical principle. In cases of gross sequestration or active infection, particularly in the tibia, a staged approach is utilized.
The bone is approached anteriorly and aggressively saucerized to remove all necrotic tissue. The incision is closed, and the infection is treated with targeted systemic antibiotics and local irrigation/suction systems.
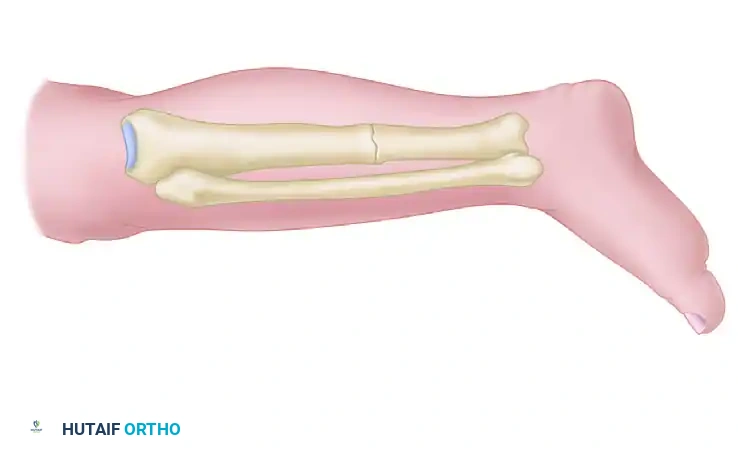
Once the infection is quiescent, bone grafting is considered. However, the anterior aspect of the tibia is strictly avoided due to the presence of old draining sinuses and compromised skin. Instead, the tibia is approached posterolaterally or posteromedially.
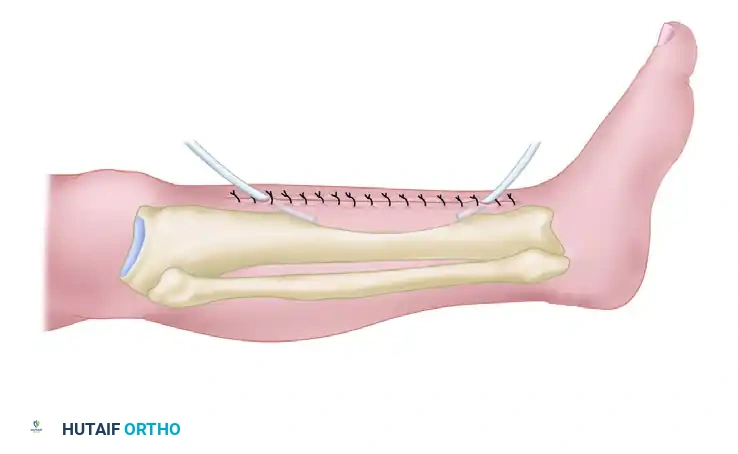
Through a posterolateral approach, the posterior aspect of the tibia (and often the fibula) is exposed and decorticated superior and inferior to the nonunion site. The entire roughened area is then covered with strips of highly osteogenic autogenous iliac crest bone graft. The actual nonunion site is intentionally not exposed, operating on the principle of bypassing the infected anterior zone to achieve a posterior synostosis.
THE ACTIVE TREATMENT PROTOCOL
Pioneered by Judet and Patel, and further refined by Weber and Cech, the "Active Treatment" method shifts the paradigm. The primary objective of this method is to obtain early bony continuity, which takes absolute priority over the complete, immediate eradication of the infection. Bony stability itself is a potent anti-infective measure.
Surgical Technique: Decortication and Stabilization
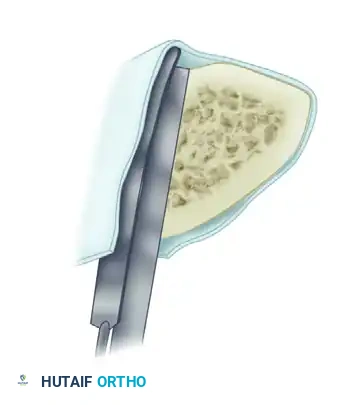
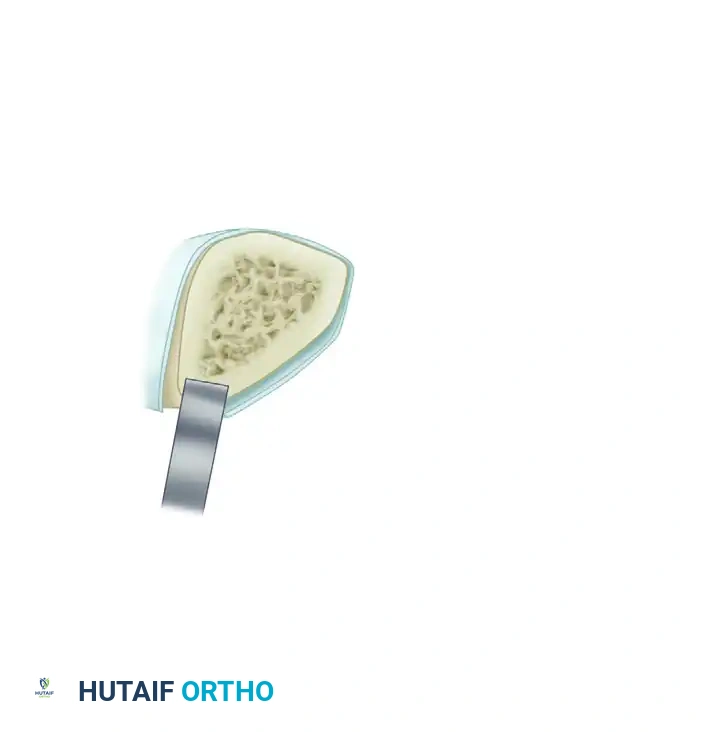
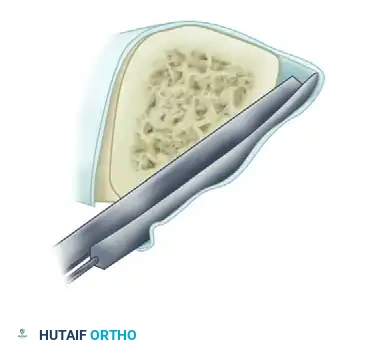
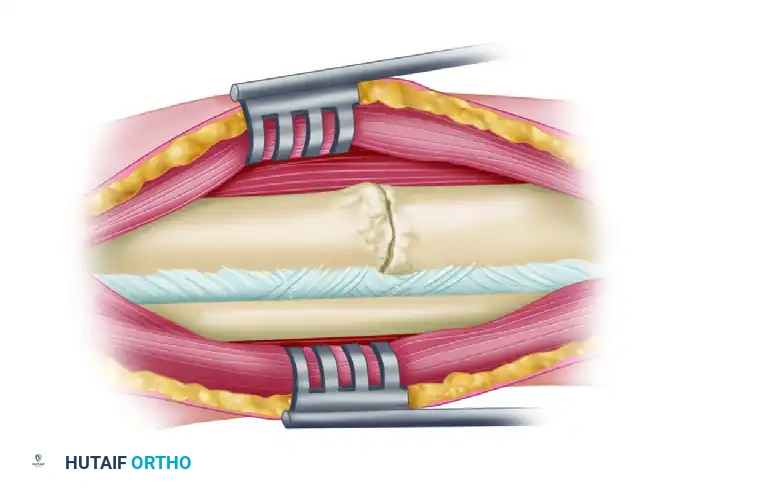
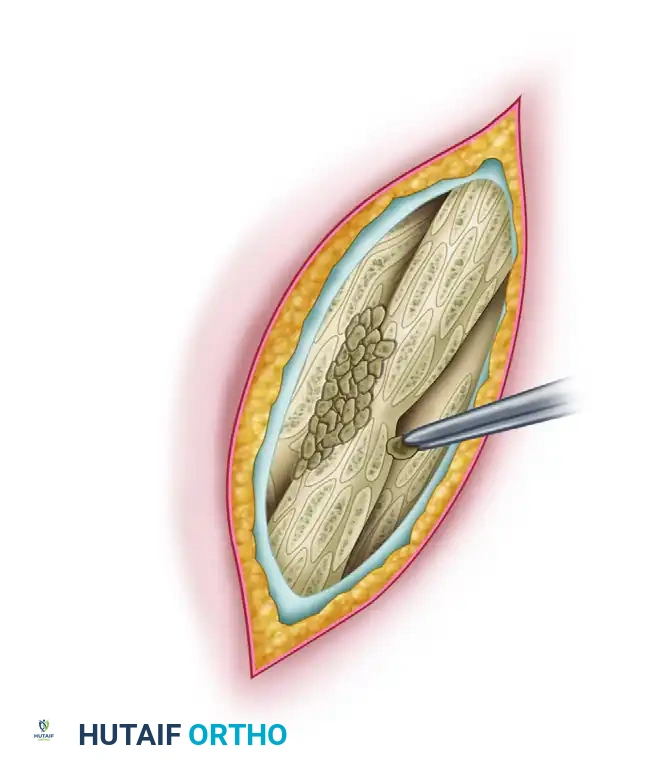
- Exposure and Decortication: The nonunion is exposed through the old scar and sinus tracts. The ends of the fragments are decorticated subperiosteally using a sharp osteotome. This creates multiple small, vascularized osteoperiosteal grafts (shingling) that remain attached to the surrounding soft tissue envelope. Any grafts that become completely detached are discarded.
- Radical Debridement: All devitalized bone, fibrous nonunion tissue, and infected soft tissues are meticulously excised until punctate cortical bleeding (the "paprika sign") is observed.
- Alignment and Stabilization: The fragments are aligned and stabilized, predominantly utilizing an external fixation device. If the fracture geometry allows, axial compression is applied across the nonunion site.
- Bone Grafting: Autogenous cancellous bone grafts are packed into any remaining defects to stimulate osteogenesis.
Surgical Warning: Internal fixation with a plate is reserved only for cases where drainage has completely ceased, the surgical approach can be made through pristine tissue away from old sinuses, or the infection is exceptionally mild and no other fixation method is viable.
If the fracture is already stabilized by a rigid intramedullary nail or plate, and the fixation remains absolutely secure, the hardware is retained. The operation proceeds with debridement and grafting, though decortication is omitted if an intramedullary nail is present to preserve the remaining cortical blood supply.
Local Antibiotic Delivery Systems
Systemic antibiotics often fail to penetrate the avascular environment of a nonunion. Therefore, local delivery systems are critical.
Polymethyl Methacrylate (PMMA) Antibiotic Beads:
Antibiotic-impregnated PMMA beads provide massive local concentrations of antibiotics—up to 200 times the concentration achieved via intravenous administration—without systemic toxicity.
* Cement Choice: Palacos (Zimmer) cement is vastly superior to Simplex (Stryker) regarding its porosity and antibiotic elution kinetics.
* Antibiotic Selection: Only heat-stable antibiotics can be used, as the exothermic reaction of curing PMMA will destroy heat-labile drugs. Tobramycin, gentamicin, and vancomycin are standard choices. Voriconazole can be incorporated for fungal/yeast infections.
* Contraindications: Quinolones must be strictly avoided. Evidence demonstrates that local quinolones significantly decrease osteoblastic function and impair fracture healing.
MANAGEMENT OF DEFORMITY, SHORTENING, AND SEGMENTAL BONE LOSS
Complicated nonunions frequently present with a combination of angular deformity, rotational malalignment, limb shortening, and segmental bone loss. The management of these multidimensional deformities was revolutionized by Gavriil Ilizarov.
The Ilizarov Method
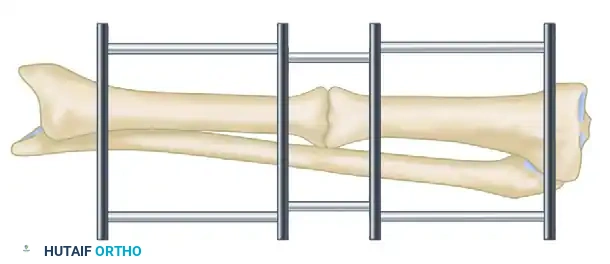
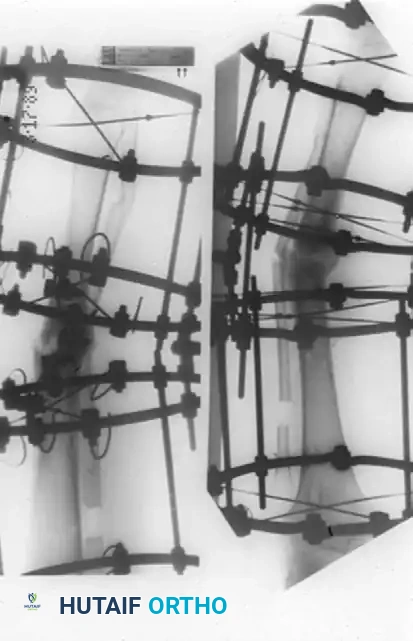
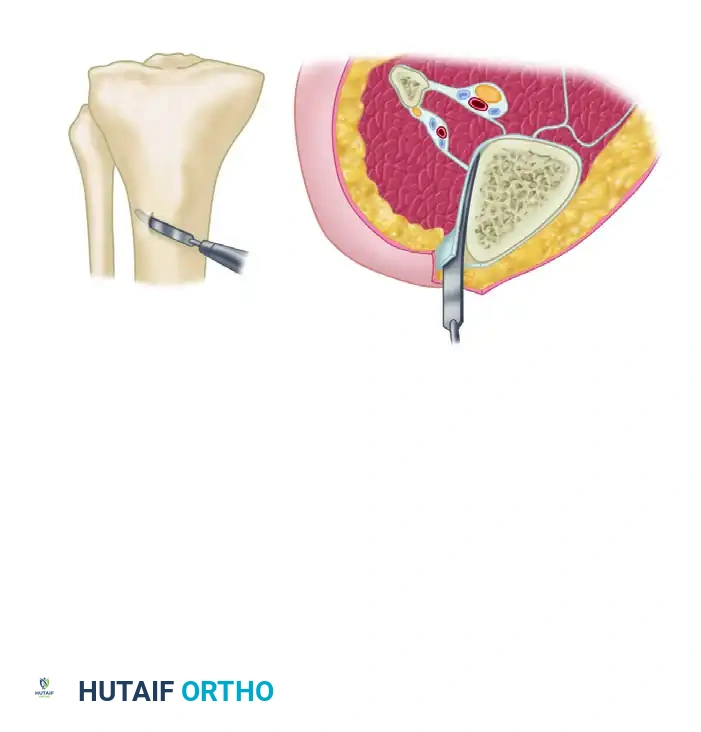
The Ilizarov method is predicated on the biological principle of distraction osteogenesis. By applying tension stress to living tissues, metabolic activation occurs, leading to the regeneration of bone and soft tissue. To eliminate infection and obtain union, local vascularity must be profoundly increased. This is achieved through a low-energy corticotomy and the application of a circular external fixator.
Ilizarov Treatment Modes:
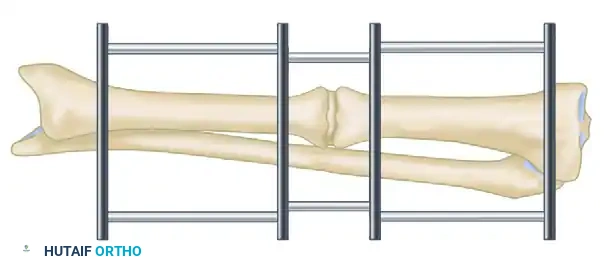
1. Monofocal: Treatment occurs at a single site (the nonunion). Techniques include pure compression, sequential distraction-compression, or pure distraction.
2. Bifocal: Treatment occurs at two sites (the nonunion and a separate corticotomy site). Techniques include compression-distraction lengthening or bone transport.
3. Trifocal: Treatment occurs at three sites, typically used for massive segmental defects requiring simultaneous transport from proximal and distal corticotomies.
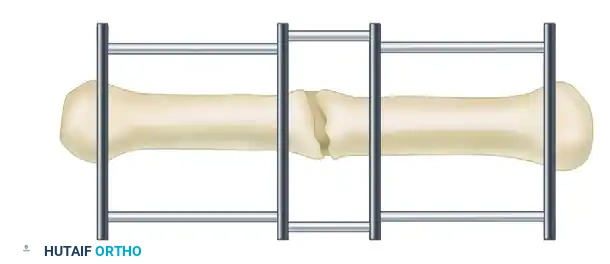
For hypertrophic nonunions with minimal infection and no sequestered bone, monofocal compression is utilized. The inherent biology of a hypertrophic nonunion is excellent; it simply lacks mechanical stability. Compression via the Ilizarov frame provides rigid stability and stimulates the existing fibrocartilage to ossify.
Conversely, atrophic nonunions with diffuse infection or sequestered bone require a bifocal approach. Open resection of the infected, necrotic segment is performed until healthy, bleeding bone is reached.
If the soft tissue envelope is poor, the bone is acutely shortened and stabilized with the external fixator to allow soft tissue healing.
Once the infection has regressed and the skin has healed, a metaphyseal corticotomy is performed.
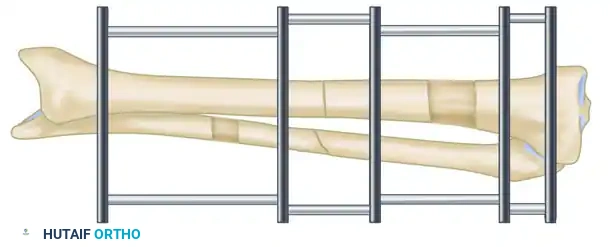
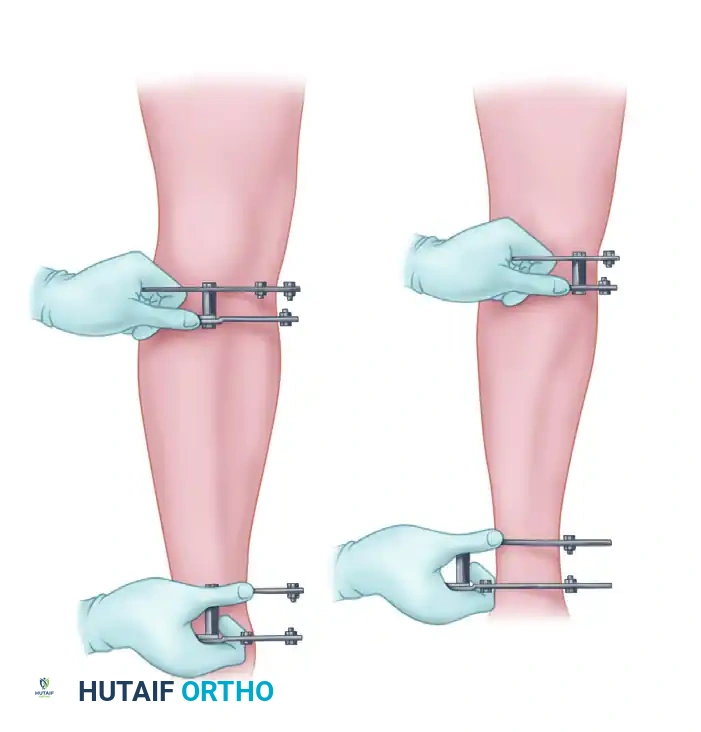
Bifocal compression-distraction is then initiated. The nonunion site is compressed to achieve union, while the corticotomy site is gradually distracted (typically 1 mm per day) to restore limb length.
Advanced Frame Application and Bone Transport
The Ilizarov method allows for the simultaneous correction of angular, rotary, and translational deformities alongside lengthening. Deformities of 10 to 15 degrees can often be corrected acutely during frame application; larger deformities must be corrected gradually using hinges and motors to prevent neurovascular compromise.

When managing segmental bone loss, the leading edge of the transported bone fragment (the "docking site") frequently becomes covered in fibrous tissue during its journey. Upon arrival at the principal fragment, this docking site usually requires surgical freshening, decortication, and the addition of autogenous bone graft to ensure a solid bony union.
The sequence of correction for complex deformities varies, but a fundamental rule is that limb length must generally be reestablished before severe angular or translational deformities are fully corrected, as premature correction can tether neurovascular structures.


The Spatial Frame Method (Taylor Spatial Frame)
While traditional Ilizarov frames rely on complex hinge placements that can be technically unforgiving, the development of hexapod circular fixators, such as the Taylor Spatial Frame (TSF), has revolutionized deformity correction. The TSF utilizes a Stewart platform—two rings connected by six telescopic struts.

By inputting the strut lengths and radiographic deformity parameters into a web-based software program, the system generates a daily prescription for strut adjustments. This allows for the simultaneous, gradual correction of 6-axis deformities (angulation, translation, and rotation in the coronal, sagittal, and axial planes).
Preoperative Planning for Spatial Frames:
The absolute prerequisite for successful TSF application is pristine preoperative imaging. True orthogonal (anteroposterior and lateral) views of the entire limb are mandatory.
These orthogonal views are used to:
1. Completely characterize the plane and extent of angulation and translational deformities.
2. Determine the correct ring diameter based on preoperative sizing of the limb (allowing for postoperative swelling).
3. Define the "mounting parameters" (the exact position of the reference ring relative to the bone).