Comprehensive Introduction and Patho-Epidemiology
Severe contractures of the forearm and hand, universally recognized in their most advanced form as Volkmann’s ischemic contracture, represent the devastating, end-stage sequelae of an untreated, delayed, or inadequately decompressed compartment syndrome. The fundamental pathophysiological insult is a profound disruption of the microcirculation within the closed osseofascial compartments of the forearm. When intracompartmental pressure exceeds the capillary perfusion pressure, an ischemic cascade is initiated. This cascade rapidly progresses from reversible cellular hypoxia to irreversible myonecrosis, typically occurring within a narrow window of four to six hours. The highly metabolic skeletal muscle tissue undergoes liquefactive and coagulative necrosis, which is subsequently replaced by dense, unyielding fibrotic scar tissue.
The neurological compromise seen in these severe contractures is multifactorial and profound. The initial anoxic insult directly damages the peripheral nerve fascicles traversing the compartment, leading to primary ischemic axonotmesis or neurotmesis. Subsequently, as the necrotic muscle undergoes fibrotic contraction, the surviving neural structures—most notably the median and ulnar nerves—become encased in a dense cicatrix. This secondary compression further exacerbates the neuropathy, leading to a profound loss of distal sensory and motor function. The classic clinical presentation includes a flexed elbow, pronated forearm, flexed wrist, clawed digits, and an adducted thumb, creating a severely dysfunctional and often insensate extremity.
Epidemiologically, Volkmann’s contracture is most frequently encountered in the pediatric population following supracondylar fractures of the humerus, where the brachial artery is either directly injured or compressed by fracture displacement and subsequent edema. In adults, high-energy crush injuries, complex fractures of the radius and ulna, prolonged external compression (such as in drug-induced coma or "found down" scenarios), and arterial injuries are the primary culprits.
The surgical management of these severe, established contractures requires a highly structured, evidence-based, and multidisciplinary approach. In mild to moderate cases, where focal areas of muscle remain viable, targeted tenolysis, tendon lengthening, or selective tendon transfers may yield acceptable functional improvements. However, when the deep volar compartment musculature—specifically the flexor digitorum profundus (FDP) and flexor pollicis longus (FPL)—is entirely necrotic and replaced by confluent scar tissue, simple local reconstruction is biologically and mechanically futile. In these advanced, end-stage cases, the definitive standard of care is the two-stage reconstructive protocol pioneered and refined by Oishi and Ezaki. This protocol consists of an initial radical excision of all necrotic tissue coupled with extensive neurolysis, followed by a delayed free functioning gracilis muscle transfer (FFGMT) to restore active, voluntary digital flexion.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of both the recipient forearm anatomy and the donor gracilis anatomy is an absolute prerequisite for executing this complex reconstruction. The volar forearm is anatomically divided into three muscular layers: superficial, intermediate, and deep. The deep compartment, containing the FDP, FPL, and pronator quadratus, is the most severely affected in Volkmann’s ischemia due to its central location, proximity to the interosseous membrane, and tenuous collateral blood supply. The anterior interosseous artery, a branch of the common interosseous artery from the ulnar artery, provides the primary vascularity to this deep layer and is highly susceptible to occlusion during compartment syndrome.
The neurovascular topography of the volar forearm dictates the approach to neurolysis and recipient vessel selection. The median nerve courses between the two heads of the pronator teres and descends deep to the flexor digitorum superficialis (FDS). Its critical motor branch, the anterior interosseous nerve (AIN), arises proximally in the forearm and courses along the interosseous membrane. In the context of FFGMT, the AIN is the preferred donor motor nerve due to its high density of motor fascicles and its synergistic physiological role in digital flexion. The ulnar nerve enters the forearm between the heads of the flexor carpi ulnaris (FCU) and descends along its deep surface. Both nerves must be meticulously dissected from the fibrotic bed during the first stage of reconstruction.
The gracilis muscle is the workhorse donor for free functioning muscle transfer in the upper extremity. It is a superficial, strap-like muscle in the medial thigh, originating from the body and inferior ramus of the pubis and inserting into the medial surface of the proximal tibia as part of the pes anserinus. Its biomechanical profile is exceptionally well-suited for finger flexor reconstruction. The muscle fibers run parallel to its longitudinal axis, providing an excursion of approximately 5 to 7 centimeters, which closely matches the physiological excursion required for full FDP and FPL function.
The vascular supply to the gracilis is classified as Mathes and Nahai Type II, with a dominant primary pedicle and several minor secondary pedicles. The dominant pedicle is the ascending branch of the medial circumflex femoral artery (MCFA) and its paired venae comitantes, which enter the muscle laterally, approximately 8 to 10 centimeters distal to the pubic tubercle. The motor innervation is provided by the anterior branch of the obturator nerve, which enters the muscle obliquely, slightly proximal to the vascular pedicle. This nerve contains a rich supply of myelinated motor axons, making it ideal for coaptation to the AIN.
Within the hand, the intrinsic musculature—comprising the lumbricals, dorsal interosseous, and volar interosseous muscles—plays a critical role in the pathophysiology of severe contractures. These muscles flex the metacarpophalangeal (MCP) joints and extend the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints via their insertion into the lateral bands of the extensor aponeurosis. The extensor hood itself is a complex biomechanical structure consisting of transverse fibers (responsible for MCP flexion) and oblique fibers (responsible for IP extension). When the intrinsic muscles become fibrotic and contracted secondary to ischemia, they exert an unyielding pull on the lateral bands, resulting in the classic "intrinsic plus" hand deformity: severe MCP flexion and PIP/DIP extension contractures.
Exhaustive Indications and Contraindications
The decision to proceed with a two-stage excision and free functioning muscle transfer is complex and must be highly individualized. It is reserved for patients with severe, end-stage ischemic contractures where local reconstructive options have been exhausted or are anatomically impossible. The primary goal is the restoration of basic hand prehension—specifically, key pinch and gross grasp. Patients must be rigorously evaluated to ensure they possess the necessary neurological and vascular prerequisites to support a microvascular muscle transfer.
Preoperative electromyography (EMG) and nerve conduction studies (NCS) are non-negotiable requirements. These studies must demonstrate the viability of the median and ulnar nerves for protective sensation, as well as the presence of a functional donor nerve—almost exclusively the AIN—to provide motor input to the transferred gracilis. Vascular imaging, either via conventional angiography or high-resolution CT angiography, is strongly recommended to map the arterial anatomy of the recipient forearm, particularly given the high likelihood of concurrent vascular injury or occlusion from the initial trauma.
| Parameter | Indications for Two-Stage FFGMT | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Muscle Viability | Complete necrosis/fibrosis of the deep volar compartment (FDP/FPL). | Presence of viable, functional FDP/FPL amenable to tenolysis or local transfer. | Partial necrosis where a local tendon transfer (e.g., BR to FPL) might suffice. |
| Neurological Status | Viable AIN (confirmed by EMG) and intact protective sensation in the hand. | Complete, irreversible avulsion or necrosis of the brachial plexus or proximal median nerve. | Severe, unrecovered median/ulnar neuropathy lacking protective sensation. |
| Vascular Bed | Patent recipient artery (brachial, radial, or ulnar) and adequate venous outflow. | Irreparable arterial occlusion rendering the extremity dependent on tenuous collateral flow. | Severe venous stasis or lack of suitable recipient veins (venae comitantes). |
| Joint Mobility | Supple passive range of motion (PROM) at the wrist, MCP, and IP joints. | Severe, fixed, bony ankylosis of the wrist and digits preventing passive flexion. | Moderate joint contractures requiring extensive simultaneous capsulotomies. |
| Patient Factors | High motivation, cognitive ability to participate in extensive rehabilitation. | Active, uncontrolled localized or systemic infection. | Poor compliance, severe psychiatric illness, or inability to tolerate prolonged rehab. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful outcomes in complex microvascular reconstruction. The clinical evaluation must meticulously differentiate between fixed joint contractures and musculotendinous tethering. The intrinsic tightness test (Bunnell test) is performed to assess the interosseous and lumbrical muscles. If the PIP joints cannot be passively flexed when the MCP joints are held in extension, but can be flexed when the MCP joints are flexed, intrinsic tightness is confirmed. The severity of this tightness dictates the necessity and extent of intrinsic release (Littler release, muscle sliding, or complete tenotomy) required either prior to or concurrent with the muscle transfer.
Radiographic evaluation includes standard orthogonal views of the forearm, wrist, and hand to rule out occult fractures, heterotopic ossification, or joint subluxations that may impede functional recovery. As previously noted, neurophysiological and vascular mapping are mandatory. The surgeon must predetermine the recipient artery (typically the brachial artery or the proximal radial/ulnar arteries) and the recipient nerve (AIN).
The surgical procedure, particularly the second stage, demands a highly coordinated two-team approach to minimize total operative time and, critically, the ischemia time of the harvested gracilis muscle. The patient is positioned supine on the operating table. The affected upper extremity is extended onto a radiolucent hand table. A sterile pneumatic tourniquet is applied high on the brachium. Concurrently, the ipsilateral lower extremity is prepped and draped freely to allow for circumferential access to the medial thigh for gracilis harvest. The knee is slightly flexed and the hip abducted and externally rotated ("frog-leg" position) to expose the medial thigh. An operating microscope must be positioned and balanced prior to the commencement of the procedure, ensuring it can easily swing into the surgical field without compromising sterility.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management is strictly divided into two distinct stages, typically separated by an interval of three to six months. This delayed approach is critical; it allows the massive soft-tissue wounds of the initial debridement to heal, permits the resolution of chronic inflammation, and provides a window for neurological recovery following neurolysis before subjecting the bed to a free tissue transfer.
Stage One: Excision of Necrotic Muscles and Neurolysis
The primary objective of the first stage is to convert a scarred, contracted, and neurologically compromised extremity into a clean, supple, and optimized recipient bed.
-
Incision and Extensile Exposure:
A curvilinear, extensile incision is designed to prevent straight-line scar contractures across joints. The incision begins proximal to the elbow at the medial epicondyle, crosses the antecubital fossa obliquely to the radial aspect, and extends distally along the volar forearm, crossing the wrist joint in a zigzag fashion to enter the palm if carpal tunnel release is indicated. Thick fasciocutaneous flaps are elevated to widely expose the volar forearm compartments. -
Neurovascular Identification and Radical Neurolysis:
The dissection begins proximally in virgin tissue. The ulnar nerve is identified at the cubital tunnel and traced distally. The brachial artery and median nerve are isolated in the antecubital fossa. Meticulous dissection is required to free these structures from the dense, unyielding fibrotic mass of the necrotic flexor-pronator origin.
Surgical Warning: The nerves are frequently encased in dense cicatrix, structurally attenuated, and highly susceptible to iatrogenic injury. The use of loupe magnification (3.5x to 4.5x) or the operating microscope is mandatory. Epineurotomy may be required if the nerve is severely constricted by intrinsic scarring. -
Radical Debridement of Myonecrosis:
This is the most critical step of Stage One. All necrotic, fibrotic, and non-functional muscle must be radically excised. Surgeons often err on the side of caution, leaving fibrotic muscle behind; this is a critical error that will physically impede the placement and excursion of the future gracilis transfer. The deep layers (FDP, FPL, pronator quadratus) are typically completely excised. By the conclusion of the debridement, the volar forearm should essentially consist of bare radius and ulna, the interosseous membrane, the mobilized neurovascular bundles, and the distal tendon stumps. -
Tendon Management and Tagging:
The distal tendinous insertions of the FDP and FPL are preserved. The proximal ends of these tendons are identified at the distal third of the forearm. To facilitate the second stage, the FDP tendons are sutured together to create a unified tendinous mass. The FPL may be included in this mass or tagged separately. These stumps are secured to the distal forearm fascia using heavy non-absorbable sutures to prevent retraction into the carpal tunnel. -
Closure and Immobilization:
Following tourniquet deflation and meticulous hemostasis, closed-suction drains are placed. The skin is closed loosely; if tension is excessive, split-thickness skin grafting may be required. The extremity is immobilized in a well-padded long-arm splint or cast.
Stage Two: Free Functioning Gracilis Muscle Transfer
Once soft-tissue equilibrium is achieved (3-6 months), Stage Two is executed.
Recipient Site Preparation (Team A):
The previous incision is reopened. The brachial artery or dominant forearm artery is isolated and prepared for microvascular anastomosis. A robust recipient vein, preferably a deep vena comitans, is isolated. The AIN is identified, mobilized, and transected proximally. Under the microscope, the AIN is serially sectioned until healthy, bleeding fascicles with visible axonal pouting are confirmed. The previously tagged FDP and FPL tendons are freed from adhesions.
Donor Site Harvest (Team B):
A longitudinal incision is made over the medial thigh. The gracilis is exposed. Surgical Warning: If a skin paddle is harvested for monitoring, it must be designed over the proximal two-thirds of the muscle, as the distal cutaneous perforators are highly unreliable.
Before detachment, marking sutures are placed exactly 2 cm apart along the longitudinal axis of the muscle. This is the Manktelow technique, which is absolutely critical for restoring the physiological length-tension relationship (the Blix curve) during inset. The dominant neurovascular pedicle (MCFA branches and obturator nerve) is meticulously dissected. Once the recipient bed is ready, the pedicle is ligated, the muscle is detached from its pubic origin and tibial insertion, and the flap is transferred.
Microvascular Anastomosis and Nerve Coaptation:
The proximal origin of the gracilis is securely anchored to the medial epicondyle using heavy (e.g., #2 or #5) non-absorbable sutures, taking immense care to protect the adjacent ulnar nerve. The microvascular anastomosis is performed under the microscope. The gracilis artery is anastomosed to the recipient artery (end-to-side or end-to-end), and the vein is coupled or hand-sewn to the recipient vein. An implantable Doppler probe is placed around the arterial anastomosis.
The nerve coaptation is performed between the AIN and the obturator nerve using 9-0 or 10-0 nylon epineurial sutures. The coaptation should be placed as close to the muscle hilum as possible to minimize the distance regenerating axons must travel.
Tenodesis and Tensioning:
The distal tendon of the gracilis is woven into the unified FDP mass using a Pulvertaft weave. Tension is applied to the gracilis muscle until the previously placed marking sutures, which relaxed upon harvest, are stretched back to exactly 2 cm apart. This guarantees the muscle is set at its optimal physiological resting length. The FPL is woven into the construct, setting the thumb in slight flexion. A tenodesis check is performed: passive wrist extension must produce full digital flexion, and passive wrist flexion must allow complete digital extension.
Management of Established Intrinsic Muscle Contractures
Severe forearm ischemia is virtually always accompanied by intrinsic muscle ischemia within the hand. The management of these intrinsic contractures is dictated by their severity and the remaining viability of the interosseous and lumbrical muscles.

FIGURE 74-9: Abduction contracture of the fifth finger in a patient who developed fibrosis in the abductor digiti quinti, likely secondary to ischemic myositis from a compressive bandage.
Mild Contractures: The Littler Release
In mild cases, the intrinsic muscles retain active function but are adaptively shortened. The Bunnell intrinsic tightness test is positive, but fixed deformity is absent. The Littler release targets the oblique fibers of the extensor hood, which are responsible for the PIP extension contracture, while preserving the transverse fibers to maintain MCP flexion.
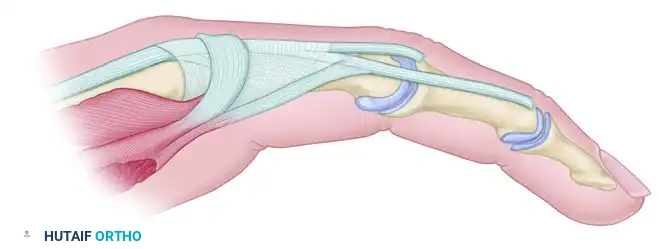
FIGURE 74-10A: Extensor aponeurosis at the level of the metacarpophalangeal joint. It consists of the long extensor tendon, transverse fibers (which flex the MCP joint), and oblique fibers (which extend the IP joints). The crosshatched part represents the oblique fibers to be resected.
Through dorsal longitudinal incisions, the lateral bands are exposed. The oblique fibers of the intrinsic wing are sharply excised from the extensor mechanism on both the radial and ulnar aspects of the hood.
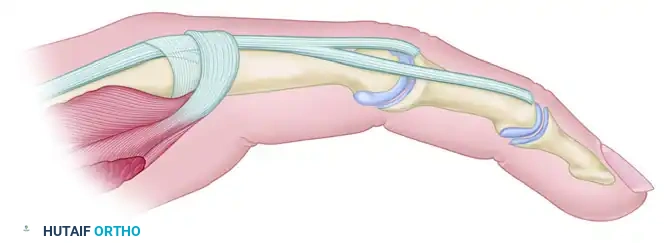
FIGURE 74-10B: Appearance of the aponeurosis after the Littler release. The transverse fibers and sagittal bands remain intact.
Moderate Contractures: Interosseous Muscle Sliding
When the interosseous muscles are viable but significantly contracted, a muscle sliding operation is indicated.
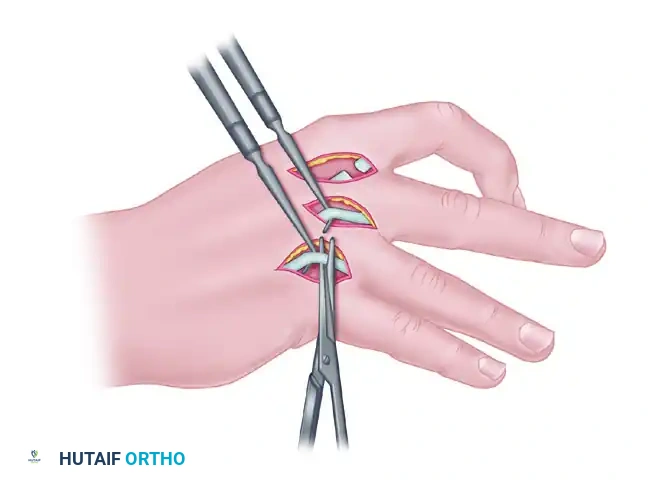
FIGURE 74-11A: Method of stripping and advancing interosseous muscles to slacken them, allowing proximal finger joints to extend and distal joints to flex. This is performed only when muscles retain considerable function. The nerve supply must be meticulously spared.
The contracted interosseous muscles are subperiosteally elevated and released from their origins on the metacarpal shafts. This proximal release allows the muscle bellies to slide distally, effectively lengthening the musculotendinous unit without destroying active function. Extreme care must be taken to preserve the deep motor branch of the ulnar nerve.
Severe Contractures: Complete Intrinsic Tenotomy
In end-stage ischemic contracture, the intrinsic muscles are completely necrotic and replaced by dense fibrosis. Useful muscle excursion is absent, rendering sliding procedures ineffective.
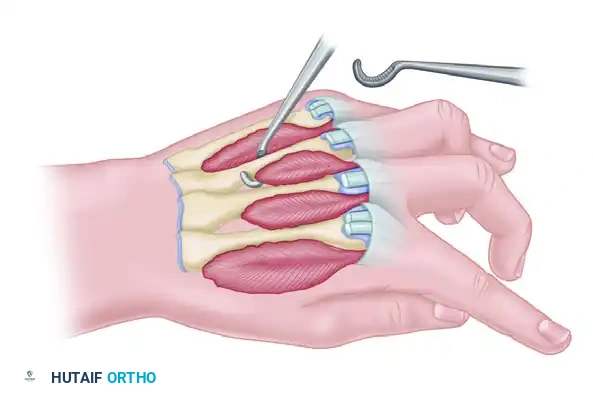
FIGURE 74-11B: Complete intrinsic tenotomy for severe intrinsic contractures in which nonfunctioning, fibrotic interosseous muscle remains.
A complete intrinsic tenotomy is required. The lateral bands and the tendinous insertions of the fibrotic interossei and lumbricals are completely divided at the level of the proximal phalanx. This radical release abolishes the tethering effect on the PIP joints, allowing passive flexion and preparing the hand for the forces generated by the FFGMT.
Complications, Incidence Rates, and Salvage Management
The two-stage reconstruction of severe forearm contractures is fraught with potential complications, ranging from microvascular failure to poor functional recovery. Patient counseling regarding these risks is paramount.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Microvascular Thrombosis (Flap Failure) | 3 - 5% | Meticulous intimal preparation; use of healthy recipient vessels outside the zone of injury; continuous postoperative Doppler monitoring. | Immediate return to OR for thrombectomy/revision. If total necrosis occurs, debridement and alternative tendon transfers (if available) or pedicled flaps. |
| Failure of Nerve Regeneration | 10 - 15% | Confirm AIN viability with intraoperative frozen section or visual axonal pouting; tension-free coaptation close to the muscle hilum. | Delayed tendon transfers (e.g., ECRL to FDP) if local muscles are available, or tenodesis procedures to establish a fixed grip. |
| Over/Under Tensioning of Gracilis | 15 - 20% | Strict adherence to the Manktelow 2-cm marking technique; intraoperative tenodesis checking. | Secondary surgical revision: re-exploration and adjustment of the Pulvertaft weave tension. |
| Infection / Wound Dehiscence | 5 - 10% | Radical debridement during Stage One; tension-free closure; judicious use of skin grafts over the muscle belly. | Aggressive serial surgical debridement, targeted intravenous antibiotics, and vacuum-assisted closure (VAC) therapy. |
| Joint Contracture Recurrence | 20 - 30% | Aggressive, protocol-driven postoperative rehabilitation; prolonged use of dynamic/static progressive splinting. | Secondary capsulotomies, intrinsic releases, or serial casting protocols. |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of an FFGMT represents only half of the reconstructive effort; the ultimate functional outcome is heavily dependent on a rigorous, highly specialized, and phased rehabilitation protocol.
Phase I: Protection and Monitoring (Weeks 0-4)
Immediately postoperatively, the patient is transferred to a specialized microvascular unit. The extremity is elevated to optimize venous drainage and prevent congestion, which is a primary cause of microvascular failure. The implantable Doppler is monitored continuously. The arm is immobilized in a bulky, protective dorsal blocking splint with the wrist in neutral to slight flexion, MCP joints in 70 degrees of flexion, and IP joints extended. This posture completely unloads the distal tenodesis site. Absolute immobilization of the muscle and tendon weaves is maintained for four weeks.
Phase II: Passive Mobilization (Weeks 4-8)
At four weeks, the splint is converted to a removable orthosis. A specialized hand therapist initiates a controlled passive range of motion (PROM) protocol. The goal is to ensure smooth gliding of the transferred tendon through the fibrotic forearm bed without applying active contractile force that could rupture the immature Pulvertaft weave. Passive wrist extension is combined with passive digital flexion, and vice versa, to maintain joint suppleness.
Phase III: Active Mobilization and Biofeedback (Weeks 8-12+)
Active motion is cautiously introduced. Because the gracilis is denervated, true active contraction will not occur until axonal regeneration reaches the motor endplates—a process that typically takes 3 to 6 months, progressing at approximately 1 mm per day. During this phase, patients are instructed to perform "place and hold" exercises. Biofeedback and electrical muscle stimulation (EMS) are critical adjuncts. The patient is taught to cognitively fire the AIN (by attempting to flex the thumb and index finger) while observing the gracilis muscle belly for early signs of reinnervation (flicker of contraction).
Phase IV: Strengthening and Functional Integration (Months 6-12)
Once visible and palpable muscle contraction is confirmed, the focus shifts to progressive resistance training and functional integration. The gracilis muscle, originally an adductor of the thigh, must be cortically remapped by the patient to function as a digital flexor. Occupational therapy focuses on restoring key pinch, chuck pinch, and gross grasp using adaptive tasks. Maximum functional recovery may not be realized until 18 to 24 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the surgical management of severe forearm contractures is anchored by several landmark publications that dictate current clinical guidelines.
The foundational two-stage protocol was established by Oishi and Ezaki, who definitively demonstrated that radical excision of all fibrotic tissue, rather than attempted salvage of necrotic muscle, is the prerequisite for successful reconstruction. Their work highlighted that residual fibrosis mechanically tethers any subsequent transfer and acts as a barrier to neurovascular regeneration.
The biomechanical principles of free muscle transfer tensioning were revolutionized by Manktelow et al. Their description of placing 2-cm marking sutures on the gracilis prior to harvest to capture the muscle's physiological resting length remains the gold standard. Adherence to this technique ensures the muscle operates at the peak of its length-tension curve (the Blix curve), maximizing the active force generated for digital flexion.
Long-term outcome studies by Chuang et al. have provided extensive data on the expected functional results of FFGMT using the AIN as a donor nerve. Their series confirmed that while grip strength rarely exceeds 20-30% of the contralateral normal hand, the restoration of functional, independent digital flexion and key pinch profoundly improves the patient's quality of life and independence in activities of daily living. These studies reinforce the clinical guideline that FFGMT, despite its complexity, is the most reliable and effective intervention for end-stage Volkmann’s ischemic contracture.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
