Comprehensive Introduction and Patho-Epidemiology
The surgical management of congenital upper extremity anomalies demands a profound understanding of altered pathoanatomy, biomechanics, and the natural history of the developing pediatric skeleton. Embryogenesis of the upper limb occurs primarily between the fourth and eighth weeks of gestation, driven by a highly orchestrated sequence of molecular signaling. The apical ectodermal ridge (AER) directs proximo-distal growth via fibroblast growth factor (FGF) expression, while the zone of polarizing activity (ZPA) dictates radioulnar (anteroposterior) patterning through the secretion of the Sonic Hedgehog (SHH) morphogen. Disruptions in these intricate pathways lead to a spectrum of congenital anomalies, ranging from longitudinal deficiencies to failure of digital separation.
Ulnar longitudinal deficiency (ULD), historically referred to as ulnar clubhand, is a rare anomaly with an estimated incidence of 1 in 100,000 to 1 in 150,000 live births. Unlike radial longitudinal deficiency, ULD is predominantly non-syndromic and sporadic, though it can occasionally be associated with focal femoral deficiency or Cornelia de Lange syndrome. The condition is characterized by partial or complete absence of the ulna, frequently accompanied by a fibrocartilaginous band known as the ulnar anlage. This anlage acts as a non-yielding tether during longitudinal growth, leading to progressive bowing of the radius, dislocation of the radial head, and severe ulnar deviation of the carpus and hand, necessitating early and decisive surgical intervention.
In stark contrast to the rarity of ULD, syndactyly is one of the most common congenital hand anomalies, occurring in approximately 1 in 2,000 to 1 in 3,000 live births. It is characterized by the failure of digital separation during embryogenesis, specifically due to the incomplete apoptosis of the interdigital necrotic zones. Syndactyly occurs most frequently between the long and ring fingers (greater than 50% of cases) and presents bilaterally in approximately half of affected patients. The condition exhibits a strong male predilection and frequently follows an autosomal dominant inheritance pattern with variable penetrance and expressivity.
Figure A: Percentage incidence of pure syndactyly (simple or complex).
Figure B: Total count incidence including all associated webbed digit conditions.
Syndactyly is frequently associated with systemic syndromes, which fundamentally alters the surgical approach and prognostic counseling. Poland Syndrome is a classic presentation, characterized by unilateral brachysyndactyly, global hypoplasia of the hand, and the pathognomonic absence of the sternocostal portion of the ipsilateral pectoralis major muscle. Conversely, Apert Syndrome presents with complex, multiple syndactylies—often manifesting as a rigid "rosebud" or "mitten" hand—tightly associated with severe craniosynostosis and midface hypoplasia. Understanding these epidemiological and syndromic nuances is paramount for the orthopedic surgeon when formulating a comprehensive, staged reconstructive plan.

Figure: Poland syndrome in an 18-month-old child.

Figure A: Brachysyndactyly associated with Poland syndrome.

Figure B: Palmar view of brachysyndactyly.

Figure C: Hypoplasia of the pectoralis major muscle, a hallmark of Poland syndrome.
Detailed Surgical Anatomy and Biomechanics
The ulnar anlage is a pathological, fibrocartilaginous remnant of the distal ulna that fails to ossify but retains its distal attachments to the ulnar carpus (typically the pisiform and triquetrum) and the distal radial physis. Biomechanically, this structure is devastating. Because the anlage lacks a growth plate, it cannot elongate in tandem with the adjacent radius. As the radius grows longitudinally, the anlage acts as a rigid bowstring. This tethering force induces a progressive, secondary deformation of the radius, driving it into severe bowing and ultimately forcing the proximal radial head to dislocate, usually posterolaterally.
Furthermore, the absence of normal ulnar osseous anatomy in ULD fundamentally alters the soft tissue envelope of the forearm. The extrinsic flexor and extensor musculature on the ulnar aspect of the forearm is typically hypoplastic or entirely absent. Consequently, the ulnar neurovascular bundle is bereft of its normal muscular protection (e.g., the flexor carpi ulnaris). The ulnar nerve and artery lie directly adjacent to the fibrocartilaginous anlage within the subcutaneous tissue. This aberrant anatomy makes surgical dissection exceedingly hazardous; the surgeon must anticipate finding critical neurovascular structures immediately deep to the dermis along the postaxial border of the limb.
In the context of syndactyly, the pathoanatomy of the web space dictates the reconstructive strategy. The normal digital commissure is not a simple U-shaped valley; it is a complex, sloped structure that begins proximally on the dorsal aspect of the hand and slopes distally toward the palmar aspect. The normal web space is supported by the natatory ligaments (superficial transverse metacarpal ligaments) and the deep transverse metacarpal ligaments. In syndactyly, these fascial structures are thickened, disorganized, and tether the digits together. Recreating the normal proximal-dorsal to distal-palmar slope is the single most critical biomechanical objective in commissure reconstruction to prevent postoperative web creep.

Figure: Simple syndactyly, palmar view. Fingers are bridged only by skin and soft tissues.

Figure: Simple syndactyly, dorsal view.
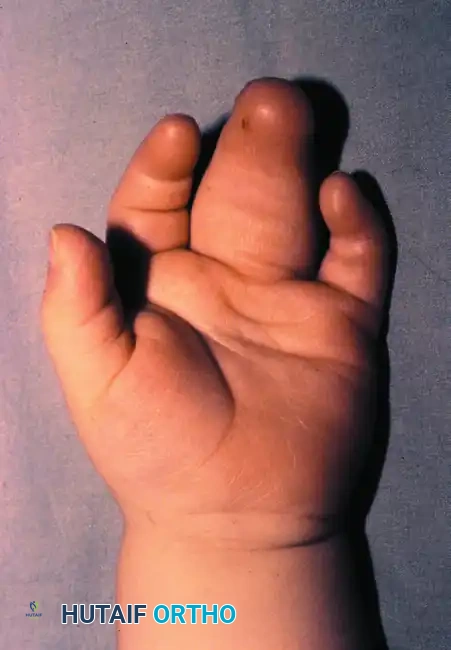
Figure: Radiograph of simple syndactyly. Note the angular deformity beginning to develop in the ring finger.
Neurovascular anatomy in syndactyly is notoriously unpredictable. While simple syndactyly often features normal, albeit distally bifurcating, common digital nerves and arteries, complex syndactyly frequently involves shared or absent neurovascular bundles. The bifurcation of the common digital nerve often lies distal to the normal commissure level, requiring meticulous intra-neural micro-dissection to separate the fascicles without inducing neuropraxia. Similarly, the arterial supply may be dominant to one digit and hypoplastic to the other, demanding careful preoperative evaluation and intraoperative decision-making before any vessel ligation is performed to facilitate separation.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in congenital upper extremity anomalies requires a rigorous assessment of the natural history of the specific deformity, the patient's functional adaptations, and the anticipated biomechanical gains. For ulnar longitudinal deficiency, the primary indication for excision of the ulnar anlage (Flatt technique) is progressive ulnar deviation of the hand or worsening radial bowing documented on serial radiographs. Surgery is typically performed in the first year of life (often between 6 and 12 months) to maximize the remodeling potential of the pediatric radius. Contraindications to anlage excision include a stable, mild deformity that does not progress, or severe elbow stiffness in extension, where the ulnar deviation of the hand paradoxically allows the child to reach their mouth for feeding.
The creation of a one-bone forearm (Straub technique) is a salvage procedure reserved for severe, functionally debilitating presentations. Indications include advanced ulnar longitudinal deficiency where the radial head is chronically dislocated, the anlage resection has failed to prevent severe recurrent bowing, or the forearm is profoundly unstable and functionally useless. It is also indicated in cases of severe radioulnar synostosis where the forearm is fixed in an extreme, non-functional position (e.g., severe hyperpronation). The primary contraindication is a functional, stable forearm with preserved hand function, as the procedure permanently sacrifices all pronosupination in exchange for a stable osseous lever arm.
In syndactyly reconstruction, the timing and indications are dictated by the specific digits involved and the complexity of the fusion. Border digits (thumb-index or ring-small fingers) represent an urgent indication for release between 6 to 12 months of age. Because these digits are of unequal length, the shorter digit acts as a tether, rapidly inducing flexion, lateral deviation, and rotational contractures in the longer adjacent digit. Conversely, central digits (index-long or long-ring fingers) of roughly equal length are an elective indication. Surgery for central syndactyly is optimally delayed until the child is 18 to 36 months old, as the larger anatomical structures reduce the technical difficulty of the procedure and significantly lower the incidence of postoperative scar contracture and distal web migration (web creep).
| Procedure / Anomaly | Primary Indications | Absolute Contraindications | Optimal Timing |
|---|---|---|---|
| Ulnar Anlage Excision (Flatt) | Progressive radial bowing; severe ulnar deviation of carpus; impending radial head dislocation. | Stable, non-progressive mild bowing; stiff elbow in extension (where deviation aids hand-to-mouth function). | 6 to 12 months of age. |
| One-Bone Forearm (Straub) | Severe forearm instability; chronically dislocated radial head with useless lever arm; severe fixed radioulnar synostosis. | Functional forearm stability; preserved active pronosupination; lack of functional hand/prehension. | Typically >2 years, or as a salvage procedure in older children. |
| Syndactyly Release (Border Digits) | Unequal digit length (e.g., thumb-index, ring-small) causing progressive angular/rotational deformity. | Medically unstable infant; active local infection. | 6 to 12 months of age (Urgent). |
| Syndactyly Release (Central Digits) | Simple or complex fusion of index-long or long-ring fingers without angular deformity. | Concomitant release of both sides of a single digit simultaneously (risks ischemic necrosis). | 18 to 36 months of age (Elective). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful congenital hand and forearm reconstruction. For ulnar longitudinal deficiency, standard orthogonal radiographs of the entire upper extremity are mandatory to assess the degree of radial bowing, the status of the proximal radial head, and the presence of any ossified ulnar remnants. Because the ulnar anlage is fibrocartilaginous and radiolucent, high-resolution ultrasound or magnetic resonance imaging (MRI) is often employed to delineate its exact proximal and distal attachments, its thickness, and its relationship to the ulnar neurovascular bundle. Genetic counseling and a comprehensive pediatric evaluation are also required to rule out associated syndromic conditions, particularly cardiac or renal anomalies.
When planning a one-bone forearm (Straub technique), precise radiographic templating is critical. The surgeon must determine the exact level of the radial and ulnar osteotomies to ensure that the distal radial fragment will perfectly abut the proximal ulnar fragment without excessive tension on the neurovascular structures. The desired resting posture of the fused forearm must be calculated preoperatively; typically, the forearm is fused in 10 to 20 degrees of pronation to optimize bimanual activities and keyboard use, though this may be adjusted based on the contralateral limb's function and the child's specific functional deficits.
For syndactyly reconstruction, preoperative clinical photography and detailed physical examination document the extent of the webbing, the presence of active and passive range of motion, and the vascular status of the digits. Plain radiographs are scrutinized to differentiate simple from complex syndactyly and to identify hidden bony anomalies, such as delta phalanges or symphalangism. The surgeon must meticulously plan the incision design, mapping out the dorsal and volar zigzag flaps (Pieri principle) and the commissure reconstruction flap (e.g., dorsal rectangular or butterfly flap) with a sterile surgical marker prior to exsanguination.
Patient positioning and operating room setup must be optimized for pediatric microvascular surgery. The patient is placed supine with the affected arm extended on a radiolucent hand table. A pediatric pneumatic tourniquet is applied to the proximal arm, and the limb is exsanguinated using an Esmarch bandage or elevation. The surgeon and assistant sit opposite each other, utilizing surgical loupe magnification (typically 3.5x to 4.5x) and specialized pediatric hand instruments. A sterile tourniquet may be utilized for infants to maximize the operative field. Strict attention to thermoregulation and blood loss is paramount, given the small total blood volume of the pediatric patient.
Step-by-Step Surgical Approach and Fixation Technique
Excision of the Ulnar Anlage (Flatt Technique)
The surgical approach for excision of the ulnar anlage demands meticulous superficial dissection due to the altered postaxial anatomy. Following exsanguination and tourniquet inflation, a lazy-"S" or zigzag incision is designed along the postaxial (ulnar) border of the forearm. The incision must carry distally across the wrist crease to the midcarpal level to allow full exposure of the ulnocarpal articulation and the distal insertion of the anlage. Straight incisions are strictly avoided to prevent longitudinal scar contracture, which could recreate a tethering effect on the growing forearm.
Upon incising the dermis, the surgeon must immediately identify and protect the ulnar neurovascular bundle. Because of the hypoplasia or complete absence of the flexor carpi ulnaris and other extrinsic flexors, the bundle is not protected by muscle bellies and lies intimately associated with the fibrocartilaginous anlage in the subcutaneous tissue. The nerve and artery are freed using blunt dissection under loupe magnification and retracted radially with vessel loops for absolute protection throughout the remainder of the procedure.
Once the neurovascular structures are secured, the fibrocartilaginous anlage is traced distally to its carpal attachments (often the pisiform, triquetrum, or the base of the fifth metacarpal) and proximally to the ulnar osseous remnant or the proximal radioulnar junction. The surgeon must resect at least one-third of the distal forearm length of the anlage, encompassing its carpal insertions. Inadequate resection is a critical technical error that risks recurrent tethering through postoperative scar tissue formation. The resected tissue is sent for histopathological confirmation.
Following resection, an aggressive soft tissue release is performed on the ulnar aspect of the wrist joint. The contracted ulnocarpal capsule and any fibrotic bands are incised. This release must be extensive enough to allow the carpus to translate radially and seat squarely on the distal radial articular surface. A crucial biomechanical check is performed: the hand should passively "flop" into neutral alignment or slight radial deviation. If the surgeon must actively push the hand into neutral, the soft tissue release is insufficient, and further ulnar-sided structures must be divided before meticulous hemostasis and skin closure.
Creation of a One-Bone Forearm (Straub Technique)
The creation of a one-bone forearm is a technically demanding procedure requiring precise osteotomies and rigid fixation. A curved longitudinal dorsoradial incision is made, beginning just proximal to the elbow joint and extending distally to the middle or distal third of the forearm. If an ulnar anlage is present, it is exposed and excised to free the proximal ulnar fragment. The internervous cleavage plane between the dorsal and volar muscle compartments is developed, taking extreme care to protect the antecubital neurovascular structures.
The most critical and hazardous step of the procedure is the identification and protection of the radial nerve and its posterior interosseous nerve (PIN) branch. The radial nerve is exposed at the level of the elbow and traced distally to its bifurcation. Surgical Warning: The PIN and the supinator muscle are often grossly displaced anteriorly or medially due to the congenital dislocation of the proximal radius. The nerve must be definitively identified and protected with a vessel loop before any osteotomies are performed.
With the neurovascular structures protected, the radial shaft is divided at the exact level corresponding to the distal end of the proximal ulnar fragment. The proximal portion of the radius, including the dislocated and deformed radial head, is excised. The proximal end of the distal radial fragment is then transposed ulnarly and abutted directly against the distal end of the proximal ulnar fragment, creating a single, continuous osseous strut.

Figure A: Resection of the distal ulnar anlage and the proximal radius (shaded areas).

Figure B: Alignment of the distal radius and proximal ulna to create a single osseous strut.
Rigid fixation of this newly created radioulnar construct is paramount for achieving bony union. A stout Kirschner wire or Steinmann pin is passed antegrade through the olecranon, across the ulnar-radial osteotomy site, and distally into the radial segment. Depending on the stability of the wrist, the pin may be advanced across the radiocarpal joint into the carpus to ensure absolute alignment. The deep fascia is closed loosely to prevent compartment syndrome, and the skin is approximated.
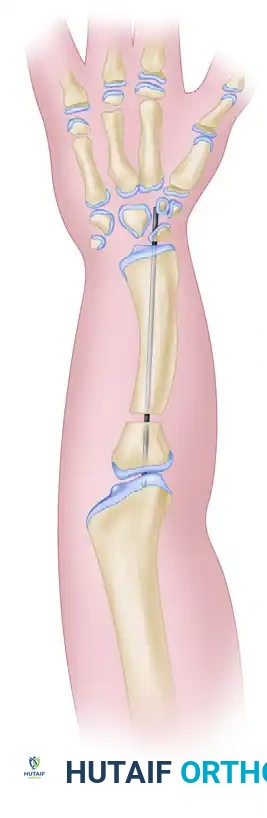
Figure C: Kirschner wire extending into the carpals, used to stabilize the newly created radioulnar segment.

Composite Diagram: Creation of a one-bone forearm demonstrating resection, alignment, and K-wire fixation.
Syndactyly Reconstruction and Commissuroplasty
Syndactyly reconstruction is a meticulous soft-tissue balancing act that involves separation of the digits, commissure reconstruction, and resurfacing of the intervening borders. Straight linear incisions are strictly contraindicated; instead, interdigitating zigzag incisions (Pieri principle) are designed to create volar and dorsal triangular flaps. These flaps break up the linear scar line, preventing longitudinal contracture that would otherwise lead to devastating flexion deformities of the growing digits.
Once the skin is incised, neurovascular dissection is performed under high magnification. The digital nerves and arteries are identified proximally in the palm and traced distally. Shared common digital nerves must be carefully split longitudinally (intra-neural neurolysis) to preserve innervation to both digits. If common digital arteries bifurcate excessively distally, it may be necessary to ligate one branch to allow digital separation; the surgeon must temporarily clamp the vessel and confirm adequate perfusion to both digits via the remaining dominant vessels before irreversible ligation. If the nail matrix is shared (complex syndactyly), a central longitudinal strip of the nail and matrix is excised to create two distinct, appropriately sized nail beds.
Commissure reconstruction is the most critical factor in preventing postoperative web creep. The normal web commissure slopes from proximal-dorsal to distal-palmar. Local flaps are vastly superior to skin grafts for the base of the commissure, as grafts inevitably contract. The dorsal rectangular flap is the workhorse technique, beginning at the transverse metacarpal ligament and extending distally. Alternatively, the Butterfly Flap (Woolf and Broadbent) is highly effective for partial simple syndactyly ending proximal to the PIP joint, where flaps designed in the web space are rotated to deepen the web and recreate the natural slope.
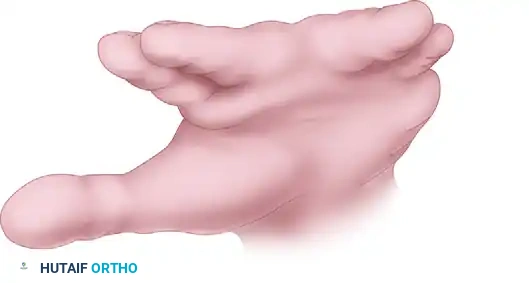
Figure: Woolf and Broadbent butterfly flap technique. Flaps are designed in the web space.
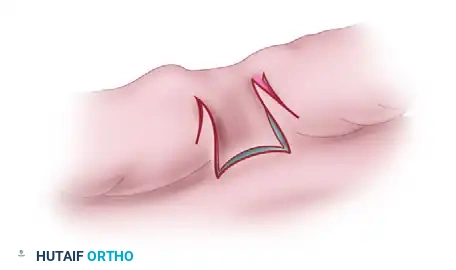
Figure: The butterfly flaps are rotated and interdigitated to deepen the web and recreate the commissure slope.
Finally, the digits must be resurfaced. The surface area of two conjoined digits is significantly less than the surface area of two separate digits; primary closure is almost never possible without inducing severe tension and subsequent ischemia. The zigzag incisions are designed so that the flaps interdigitate to close one digit primarily, while the adjacent digit requires full-thickness skin grafting (FTSG). Grafts are typically harvested from the groin crease or hypothenar eminence to provide optimal color match and minimize secondary graft contracture compared to split-thickness grafts.

Associated Diagram 1: Detailed schematic of complex syndactyly release.

Associated Diagram 2: Soft tissue balancing and graft placement in syndactyly.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for congenital upper extremity anomalies carries a unique set of complications related to the altered anatomy and the dynamic nature of the growing pediatric skeleton. In ulnar longitudinal deficiency, the most common complication following anlage excision is recurrent radial bowing or recurrent ulnar deviation of the hand. This is almost exclusively due to inadequate resection of the fibrocartilaginous tether (failing to resect the requisite one-third of the distal anlage) or insufficient soft-tissue release at the ulnocarpal joint. Salvage management requires revision surgery for wider resection, and in severe recurrent cases, corrective radial osteotomies may be necessary.
For the creation of a one-bone forearm, nonunion at the radioulnar osteotomy site is a
