Introduction to Burn-Induced Compartment Syndrome
Severe thermal injuries to the upper extremity, particularly deep partial-thickness and full-thickness circumferential burns, present a profound threat to limb viability. The thermal destruction of the dermis results in a rigid, inelastic, and unyielding layer of dead tissue known as an eschar. Concurrently, the systemic inflammatory response to severe burns induces a massive capillary leak syndrome. As the patient undergoes aggressive intravenous fluid resuscitation (e.g., via the Parkland formula), protein-rich plasma extravasates into the interstitial space, causing profound tissue edema.
When this rapidly expanding edema is constrained by the rigid eschar, interstitial hydrostatic pressure rises exponentially. Once the interstitial pressure surpasses capillary perfusion pressure, microvascular collapse occurs, initiating a devastating ischemic cascade. This phenomenon is clinically recognized as burn-induced compartment syndrome. If left untreated, it rapidly progresses to irreversible myonecrosis, ischemic nerve damage, and ultimately, the need for major limb amputation.
Escharotomy—the surgical incision through the eschar to release the underlying tension—is a critical, time-sensitive, limb-saving intervention. It restores distal perfusion and preserves the functional integrity of the upper extremity.
Pathophysiology and Biomechanics of Burn Edema
Understanding the biomechanics of burn edema is essential for the orthopedic surgeon managing the burned upper extremity. The pathophysiology is governed by Starling’s forces. Thermal injury causes direct microvascular thrombosis and the release of vasoactive mediators (histamine, bradykinin, prostaglandins, and oxygen free radicals). These mediators drastically increase capillary permeability.
In a normal physiological state, the fascial compartments and the elastic dermis can accommodate mild to moderate fluid shifts. However, a full-thickness burn destroys the elastic properties of the skin. The eschar acts as a biological tourniquet. As interstitial volume increases, the pressure within the closed space rises.
Clinical Pearl: Capillary blood flow is typically compromised when tissue pressure exceeds 30 mm Hg, or when the difference between diastolic blood pressure and compartment pressure (ΔP) falls below 30 mm Hg. In the burned upper extremity, this threshold can be reached within hours of the initial injury.
Clinical Evaluation and Indications
The decision to perform an escharotomy is primarily clinical, supported by objective vascular assessments. The classic "6 Ps" of compartment syndrome (Pain, Pallor, Pulselessness, Paresthesia, Paralysis, and Poikilothermia) are notoriously unreliable in the burn patient. Pain is often masked by the burn itself or by systemic analgesia, while pallor and poikilothermia are obscured by the charred eschar.
Objective Assessment Modalities
- Doppler Ultrasonography: The gold standard for non-invasive bedside assessment. The absence or progressive diminution of pulsatile flow in the radial, ulnar, and palmar arch arteries, or the digital vessels, is a definitive indication for immediate escharotomy.
- Compartment Pressure Monitoring: Direct measurement using a solid-state transducer or a slit-catheter technique. Pressures exceeding 30 mm Hg in the forearm or intrinsic hand compartments mandate surgical release.
- Pulse Oximetry: While less reliable due to peripheral vasoconstriction and carbon monoxide poisoning, a sudden drop in digital plethysmographic waveforms can serve as an early warning sign of impending ischemia.
Preoperative Preparation and Anesthesia
Escharotomies are frequently performed emergently, either in the burn intensive care unit (BICU) or the operating theater.
Hemodynamic and Hematologic Preparation
- Blood Transfusion Readiness: Prepare the patient preoperatively for potential blood transfusion. While the eschar itself is avascular, the incisions will inevitably traverse into the hyperemic, viable subcutaneous tissues and potentially muscle, leading to significant blood loss. Ensure a current type and crossmatch is available.
- Coagulation Profile: Assess for burn-induced coagulopathy and correct severe derangements if time permits, though the procedure should not be delayed in the face of acute ischemia.
Anesthesia and Positioning
- Anesthesia: With the patient supine, the procedure is usually performed under general anesthesia. In critically unstable patients, bedside escharotomy may be performed with intravenous sedation and local analgesia, as the full-thickness eschar is insensate.
- Positioning: The upper extremity is extended and abducted on a radiolucent hand table.
- Preparation: Thoroughly clean the entire extremity with an approved surgical antiseptic (e.g., chlorhexidine gluconate or povidone-iodine) and apply sterile draping, exposing the limb from the axilla to the fingertips.
Step-by-Step Surgical Technique
The goal of escharotomy is to completely release the constricting eschar from the level of healthy tissue proximally to healthy tissue distally. The incisions must be carried down through the eschar and the superficial fascia, allowing the wound edges to separate widely.
Forearm and Arm Escharotomy
- Incision Placement: Make medial and lateral midaxial longitudinal incisions through the eschar. The midaxial lines are chosen to avoid injury to the major superficial veins (cephalic and basilic) and the primary flexor and extensor tendon groups.
- Instrument Selection: Utilize an electrocautery device set to a cutting current. This provides simultaneous incision and preliminary hemostasis. A scalpel may be used, but electrocautery is preferred to minimize blood loss in the hyperemic subcutaneous layer.
- The Cubital Tunnel Warning:
> Surgical Warning: At the elbow, it is critical to alter the trajectory of the medial incision. The incision must be routed anterior to the medial epicondyle. A straight midaxial incision at this level risks catastrophic iatrogenic transection of the ulnar nerve as it passes through the cubital tunnel. - Distal Extension: Continue the incisions distally, stopping precisely at the level of the metacarpophalangeal (MCP) joints to avoid exposing the joint capsules or extensor mechanisms.
Transition to Fasciotomy
Escharotomy releases the skin envelope, but it does not release the deep fascial compartments.
* Indication for Fasciotomy: If the muscle compartments remain tense to palpation after the escharotomy, or if intracompartmental pressures remain elevated (>30 mm Hg), a formal fasciotomy must be performed.
* Execution: Extend the release through the deep investing fascia of the volar and dorsal forearm compartments, as well as the intrinsic compartments of the hand, to prevent deep myonecrosis.
Hand and Metacarpal Release
The dorsum of the hand is highly susceptible to burn edema due to its loose areolar tissue and thin skin.
1. Intermetacarpal Incisions: Make additional dorsal longitudinal intermetacarpal incisions.
2. Placement: These are typically placed between the index and middle metacarpals (2nd web space) and between the ring and little metacarpals (4th web space).
3. Deep Release: These incisions allow direct access for the release of the dorsal interosseous fascia, decompressing the intrinsic muscle compartments of the hand.
Digital Escharotomy
Following the proximal releases, immediately re-evaluate the adequacy of distal perfusion. Assess skin color, warmth, and most importantly, pulsatile flow in the hand and digits using a sterile Doppler probe. If finger perfusion remains unsatisfactory, digital escharotomies are strictly indicated.
- Instrument: Use a pinpoint electrocautery tip to ensure precision in the tight confines of the digit.
- Finger Incisions (Index, Middle, Ring, Little): Make longitudinal incisions along only the ulnar sides of the involved digits. The ulnar side is selected to preserve the critical tactile sensation on the radial side of the digits, which is essential for pinch grip.
- Trajectory: The incision must run from the distal phalanx proximally to the finger web spaces.
- Safe Zone:
> Surgical Pearl: The digital incision must be placed exactly in the midaxial line—specifically, between the volar digital neurovascular bundles and the dorsal extensor tendon apparatus. Straying volar risks nerve transection; straying dorsal risks exposing the extensor tendon, leading to desiccation and rupture. - Thumb Escharotomy: Make the incision for the thumb along the radial side, extending from the distal phalanx to the base of the thumb at the first metacarpal. This avoids the critical ulnar digital neurovascular bundle, which is vital for key pinch against the index finger.
Hemostasis and Final Assessment
- Hemostasis: Obtain meticulous hemostasis using electrocautery. Uncontrolled bleeding beneath postoperative dressings can lead to hematoma formation, which acts as a nidus for infection and can recreate a localized compartment syndrome.
- Final Doppler: Use the Doppler probe one final time to confirm the restoration of robust distal arterial flow in all digits and the palmar arch.
Postoperative Care and Rehabilitation
The immediate postoperative period is focused on maintaining perfusion, preventing infection, and initiating early rehabilitation to prevent devastating burn contractures.
Dressings and Positioning
- Wound Coverage: Apply a nonadhering, medicated gauze (such as bismuth tribromophenate or silver-impregnated mesh) directly to the escharotomy wounds.
- Wrapping: Cover the extremity with a bulky, highly absorbent, but strictly non-constricting dressing. Avoid circumferential taping.
- Elevation: The limb must be continuously elevated above the level of the heart to promote venous and lymphatic drainage, thereby reducing ongoing edema.
- Monitoring: Circulation must be monitored hourly. The nursing staff should be trained to perform capillary refill checks and Doppler assessments.
Rehabilitation
- Early Mobilization: Finger movement is encouraged immediately. Active and passive range of motion (ROM) exercises prevent tendon adhesions and joint stiffness.
- Splinting: When resting, the hand should be splinted in the "intrinsic-plus" (safe) position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and interphalangeal joints fully extended. This maintains the collateral ligaments at their maximal length, preventing extension contractures.
Definitive Coverage and Skin Grafting
Treatment after the initial emergent escharotomy depends heavily on the extent and depth of the burn. Escharotomy is a temporizing, limb-saving measure; it is not the definitive treatment for the burn wound itself.
If the burn is extensive and deep enough to require escharotomy, the necrotic eschar will eventually need to be surgically removed to prevent burn wound sepsis and to prepare the bed for definitive closure.
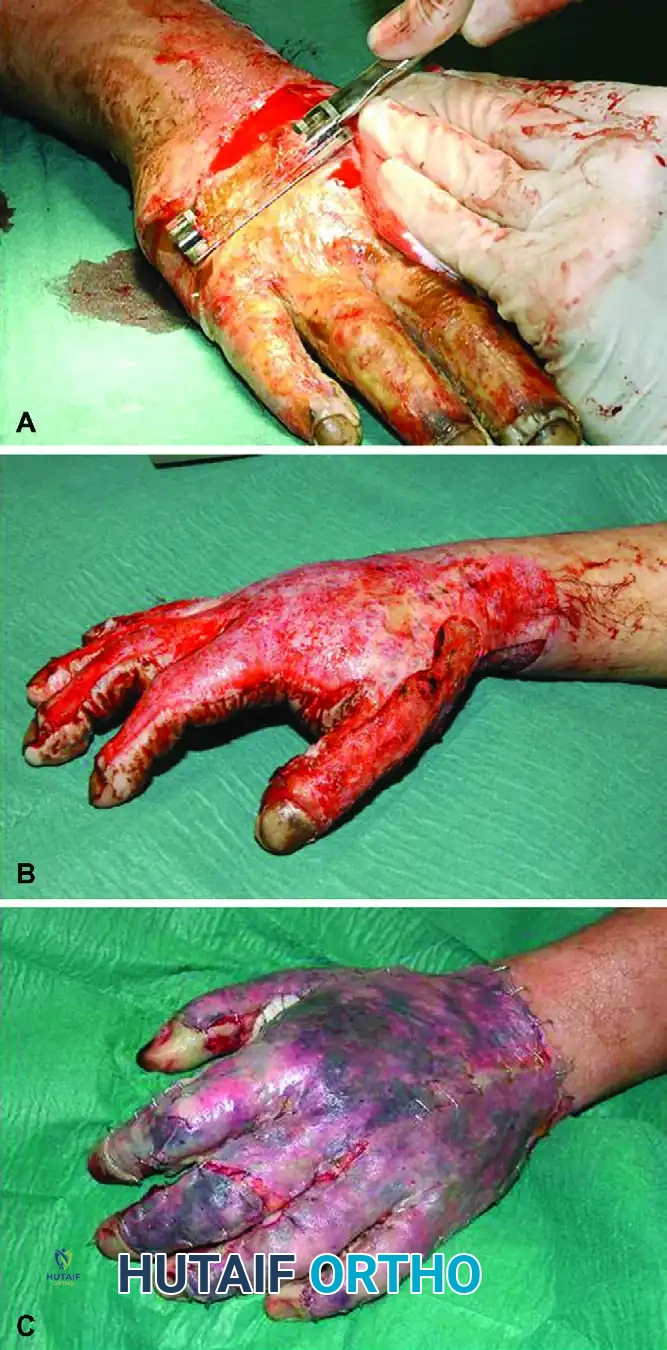
FIGURE 70-7 A, Tangential excision of deep partial-thickness burn on dorsum of hand. B, Sheet graft transplantation to excised areas. C, Short-term postoperative result. (From Germann G, Weigel G: The burned hand. In Wolfe SW, editor: Green’s operative hand surgery, ed 6, Philadelphia, 2011, Elsevier.)
As demonstrated in the clinical progression above, once the patient is hemodynamically stable, the patient is returned to the operating room for definitive management:
1. Tangential Excision (Figure 70-7 A): The necrotic eschar is tangentially excised using a Watson or Goulian knife down to healthy, punctate bleeding dermis or subcutaneous fat.
2. Sheet Graft Transplantation (Figure 70-7 B): The excised areas, particularly on the dorsum of the hand where cosmetic and functional demands are high, are covered with unmeshed sheet autografts. Sheet grafts are preferred over meshed grafts on the hand to minimize secondary contracture and optimize the functional glide of the underlying extensor tendons.
3. Postoperative Result (Figure 70-7 C): Meticulous surgical technique, combined with aggressive hand therapy, yields excellent short-term and long-term functional results, preserving the complex biomechanics of the upper extremity.
Complications and Avoidance
Even when performed correctly, escharotomies carry inherent risks that the orthopedic surgeon must anticipate and mitigate.
- Inadequate Release: The most common error is failing to extend the incisions far enough proximally or distally, leaving residual constricting bands. Always incise from unburned skin to unburned skin if possible.
- Iatrogenic Nerve Injury: As emphasized, the ulnar nerve at the elbow and the digital nerves in the hand are highly vulnerable. Strict adherence to the midaxial lines and anterior routing at the medial epicondyle is mandatory.
- Tendon Exposure: Incising too deeply over the dorsum of the hand or digits can expose the delicate extensor paratenon. Exposed tendons rapidly desiccate, leading to necrosis and rupture. If a tendon is inadvertently exposed, it must be kept continuously moist with saline or biologic dressings until definitive flap or graft coverage can be achieved.
- Infection: The open escharotomy wound is a direct portal for bacterial invasion. Strict aseptic technique during dressing changes and the use of topical antimicrobials (e.g., mafenide acetate or silver sulfadiazine) are critical to preventing invasive burn wound sepsis.
