Comprehensive Introduction and Patho-Epidemiology
The initial management of a patient presenting with peripheral nerve damage must strictly adhere to Advanced Trauma Life Support (ATLS) principles. As with any high-energy or penetrating trauma, the preservation of life and limb takes absolute precedence over the restoration of neurologic function. Cardiopulmonary stabilization, hemorrhage control, and the prevention of shock are the primary objectives. Once major visceral injuries have been addressed and resuscitative measures are underway, the orthopedic surgeon must systematically evaluate the peripheral nerve deficit. Peripheral nerve injuries (PNIs) occur in approximately 2% to 3% of all Level I trauma admissions, frequently complicating fractures, dislocations, and penetrating wounds. The profound functional morbidity associated with these injuries demands an exhaustive understanding of nerve pathophysiology, microsurgical principles, and longitudinal rehabilitation.
The pathophysiology of peripheral nerve trauma is defined by a complex, highly orchestrated cellular cascade that dictates the potential for spontaneous recovery versus the absolute need for surgical intervention. Seddon’s classification (Neurapraxia, Axonotmesis, Neurotmesis) and Sunderland’s expansion into five distinct degrees of injury provide the foundational framework for understanding nerve pathology. In a complete transection (Sunderland Grade V), the distal nerve segment undergoes Wallerian degeneration. Within 24 to 48 hours, an influx of extracellular calcium activates calpains, leading to the rapid proteolysis of the axonal cytoskeleton. Concurrently, Schwann cells dedifferentiate, proliferate, and phagocytize myelin debris in concert with hematogenous macrophages recruited by monocyte chemoattractant protein-1 (MCP-1).
Proximally, the neuronal cell body undergoes central chromatolysis, characterized by the dissolution of Nissl bodies, peripheral displacement of the nucleus, and a massive upregulation of structural proteins (e.g., tubulin, actin) and neurotrophic receptors required for axonal elongation. The dedifferentiated Schwann cells in the distal stump align to form the bands of Büngner, creating biologically active endoneurial tubes that secrete Nerve Growth Factor (NGF), Brain-Derived Neurotrophic Factor (BDNF), and Glial Cell Line-Derived Neurotrophic Factor (GDNF). These neurotrophic factors guide the regenerating axonal growth cone via chemotaxis and haptotaxis. However, this optimal biological environment is highly time-sensitive; prolonged denervation leads to irreversible Schwann cell senescence, endoneurial fibrosis, and the ultimate degradation of motor endplates, rendering late surgical repair futile.
The epidemiology of peripheral nerve trauma highlights a bimodal distribution, predominantly affecting young, active males involved in motor vehicle collisions, industrial accidents, or violent altercations, and an older cohort suffering from low-energy falls resulting in traction injuries or fracture-associated nerve palsies. The mechanism of injury—whether sharp laceration, severe crush, high-velocity missile, or longitudinal traction—fundamentally alters the zone of injury. Sharp transections present with a minimal zone of microscopic trauma, whereas blast and avulsion injuries exhibit extensive intraneural hemorrhage, fascicular disruption, and microvascular thrombosis extending centimeters beyond the macroscopic lesion. Recognizing this pathophysiological distinction is the cornerstone of surgical decision-making regarding the timing and technique of neurorrhaphy.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of peripheral nerve microanatomy is the prerequisite for successful microsurgical reconstruction. Peripheral nerves are structurally complex composite tissues consisting of conducting neural elements embedded within a highly specialized, multi-layered connective tissue stroma. The outermost layer, the mesoneurium (or adventitia), is a loose areolar tissue that allows the nerve trunk to glide seamlessly across adjacent fascial planes and muscular beds during joint excursion. Deep to the mesoneurium lies the epineurium, which is subdivided into the epifascicular epineurium, enveloping the entire nerve trunk, and the interfascicular epineurium, which separates individual fascicles. The epineurium is predominantly composed of Type I and Type III collagen and serves as the primary load-bearing structure of the nerve, protecting the delicate fascicles from compressive and tensile forces.
The perineurium is a dense, metabolically active, lamellated sheath of specialized perineurial cells surrounding each individual fascicle. These cells are joined by tight junctions, forming the critical blood-nerve barrier that maintains the strictly regulated endoneurial microenvironment essential for axonal conduction. Violation of the perineurium during surgical repair or trauma leads to endoneurial edema, localized demyelination, and dense intraneural scarring. Deep to the perineurium is the endoneurium, a delicate network of reticular fibers surrounding individual myelinated and unmyelinated nerve fibers. The spatial organization of these fascicles is highly dynamic. In the proximal segments of major nerve trunks, the fascicular topography is polyfascicular and highly plexiform, with fascicles constantly dividing and anastomosing. Distally, as the nerve approaches its target end-organs, the topography becomes oligofascicular and distinct, allowing for precise identification of motor and sensory groups.
The vascular supply to the peripheral nerve is robust and highly specialized, categorized into an extrinsic and an intrinsic system. The extrinsic system consists of segmental vasa nervorum derived from adjacent major arteries, which enter the mesoneurium and form a macroscopic plexus on the epineurial surface. These vessels pierce the epineurium to anastomose with the intrinsic microcirculation—a longitudinally oriented capillary network located within the endoneurium. This intrinsic system is remarkably resilient to mobilization; however, excessive tension across a nerve repair rapidly compromises this microvascular network. Lundborg’s seminal microcirculatory studies demonstrated that a longitudinal strain of merely 8% to 15% completely occludes the intrinsic venules and arterioles, leading to profound ischemia, localized fibroblast proliferation, and the formation of a dense scar that acts as an impenetrable barrier to regenerating axons.
Biomechanically, peripheral nerves exhibit non-linear, viscoelastic properties. During normal extremity movement, nerves undergo significant longitudinal excursion—for example, the median nerve glides up to 15 mm at the wrist during full flexion and extension. The undulating course of the nerve fibers (the bands of Fontana) provides a physiologic buffer, allowing the nerve to stretch slightly before tension is transmitted to the connective tissue stroma. In the context of neurorrhaphy, the surgeon must respect these biomechanical limits. Attempting to close a critical nerve gap by placing the limb in extreme, non-physiologic flexion inevitably results in delayed failure. As the patient mobilizes post-operatively, the viscoelastic limits of the repair site are exceeded, resulting in micro-ruptures of the coaptation, catastrophic ischemia, and the development of a neuroma-in-continuity.
Exhaustive Indications and Contraindications
The decision-making matrix for the surgical management of peripheral nerve injuries is dictated by the mechanism of injury, the condition of the soft-tissue envelope, the patient’s physiological status, and the precise timing of presentation. The overarching goal is to perform a tension-free, anatomically precise coaptation within the optimal biological window.
Timing Paradigms and Surgical Indications
Immediate Primary Repair (Within 24-48 Hours): Immediate microsurgical repair is the absolute gold standard for clean, sharply incised wounds (e.g., glass lacerations, scalpel injuries) where the zone of trauma is minimal and visually distinct. The patient must be hemodynamically stable, and the operating theater must be equipped with a high-resolution operating microscope, microsurgical instrumentation, and an experienced surgical team. Immediate repair capitalizes on the lack of distal stump retraction and the absence of fibrotic tissue, allowing for optimal fascicular alignment.
Delayed Primary Repair (3 to 7 Days): This paradigm is indicated for patients with polytrauma requiring physiological optimization, or when the initial presentation occurs at a facility lacking microsurgical capabilities. It is also the preferred approach for blunt lacerations where the microscopic extent of the injury is slightly ambiguous. The wound is thoroughly irrigated, aggressively débrided, and provisionally closed. The delay allows for the initial inflammatory phase to subside and the true zone of injury to declare itself, while still permitting direct end-to-end coaptation before significant axonal retraction and soft-tissue contracture occur.
Secondary Repair (3 to 6 Weeks): Secondary repair is strictly indicated for complex, high-energy trauma, including high-velocity gunshot wounds, severe crush avulsions, blast injuries, and heavily contaminated agricultural wounds. In these scenarios, the acute zone of injury is entirely indistinguishable. Attempting an acute primary repair in a blast injury guarantees failure due to progressive intraneural necrosis. The wound undergoes serial débridement. The severed nerve ends are identified, tagged with radio-opaque non-absorbable sutures, and tacked to adjacent healthy fascia to prevent massive retraction. Definitive neurorrhaphy or interfascicular grafting is delayed until the soft-tissue bed is pristine, the risk of sepsis is eradicated, and the proximal neuroma and distal glioma are clearly demarcated, ensuring that resection yields perfectly healthy fascicles.
| Clinical Scenario | Recommended Intervention | Rationale | Absolute Contraindications |
|---|---|---|---|
| Clean, sharp laceration (e.g., knife) | Immediate Primary Repair (<48 hrs) | Minimal zone of injury, no retraction, optimal anatomical alignment. | Hemodynamic instability, active life-threatening hemorrhage. |
| Blunt laceration / Mild crush | Delayed Primary Repair (3-7 days) | Allows zone of injury to declare, accommodates polytrauma stabilization. | Gross contamination, impending compartment syndrome. |
| High-velocity GSW / Blast injury | Secondary Repair / Grafting (3-6 weeks) | Extensive microscopic necrosis; requires demarcation of healthy tissue. | Attempting primary end-to-end repair acutely (guarantees failure). |
| Closed traction injury / Fracture palsy | Observation + Serial EMG (3-4 months) | High likelihood of spontaneous recovery (neurapraxia/axonotmesis). | Immediate exploration (unless iatrogenic post-reduction is suspected). |
| Iatrogenic palsy post-reduction | Immediate Surgical Exploration | High suspicion of nerve entrapment within fracture site or acute laceration. | Expectant management (risks permanent mechanical damage). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the bedrock of successful peripheral nerve reconstruction. The evaluation begins with a meticulous, highly detailed clinical examination. The specific nerve deficit must be documented with discrete Medical Research Council (MRC) motor grading for every innervated muscle group. Sensory mapping must be performed using static and moving two-point discrimination, as well as Semmes-Weinstein monofilament testing, to establish a precise baseline. This examination must be completed and thoroughly documented before the administration of any regional or general anesthetic.
Advanced diagnostic modalities play a critical role, particularly in closed injuries or delayed presentations. High-resolution ultrasound (HRUS) has revolutionized the anatomical assessment of peripheral nerves, allowing the surgeon to visualize neuromas, partial lacerations, nerve entrapments, and the exact length of a nerve gap dynamically. Magnetic Resonance Neurography (MRN) provides unparalleled soft-tissue contrast, identifying longitudinal signal changes indicative of Wallerian degeneration, intraneural edema, and exact anatomical disruption. Electromyography (EMG) and Nerve Conduction Velocity (NCV) studies are utilized in delayed presentations; however, the surgeon must recognize that fibrillations and positive sharp waves (indicative of denervation) do not appear until 3 to 4 weeks post-injury.
In the operating theater, precise patient positioning is critical to facilitate wide extensile exposures and simultaneous autologous nerve graft harvesting. For upper extremity reconstructions, the patient is positioned supine with the arm extended on a radiolucent hand table. If a sural nerve graft is anticipated, the ipsilateral or contralateral lower extremity must be prepped and draped freely, often requiring the knee to be slightly flexed and internally rotated to access the posterolateral calf.
A pneumatic tourniquet is applied to provide a bloodless field during the initial macroscopic dissection and neuroma resection. However, the tourniquet must be deflated, and meticulous hemostasis achieved using bipolar micro-forceps, prior to the final microscopic coaptation. An endoneurial or epineurial hematoma at the repair site is profoundly neurotoxic and acts as a potent stimulus for fibroblast proliferation and dense scar formation. The surgical microscope must be draped and positioned early in the case. Operating loupes (3.5x to 4.5x magnification) are utilized for the macroscopic exposure, while the operating microscope (providing 10x to 40x magnification) is absolutely mandatory for the delicate fascicular dissection, preparation of the nerve ends, and the placement of 8-0 to 10-0 monofilament sutures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to a peripheral nerve injury must be extensile, respecting the internervous planes and minimizing devascularization of the surrounding soft-tissue envelope. The incision is designed to cross flexion creases obliquely to prevent post-operative scar contractures. The cardinal rule of peripheral nerve surgery is to identify the uninjured nerve in pristine, virgin tissue both proximally and distally before tracing it toward the zone of injury. This prevents inadvertent iatrogenic transection of the nerve embedded within dense fibrotic scar tissue.
Once the injured nerve ends are isolated, they are mobilized extensively to gain length. However, the surgeon must meticulously preserve the segmental vasa nervorum; stripping the nerve from its mesoneurium over extensive distances severely compromises the intrinsic microcirculation.
Preparation of the Nerve Ends
The most critical step in neurorrhaphy is the preparation of the nerve ends. The zone of trauma must be radically resected until perfectly healthy, pouting fascicles are visualized.
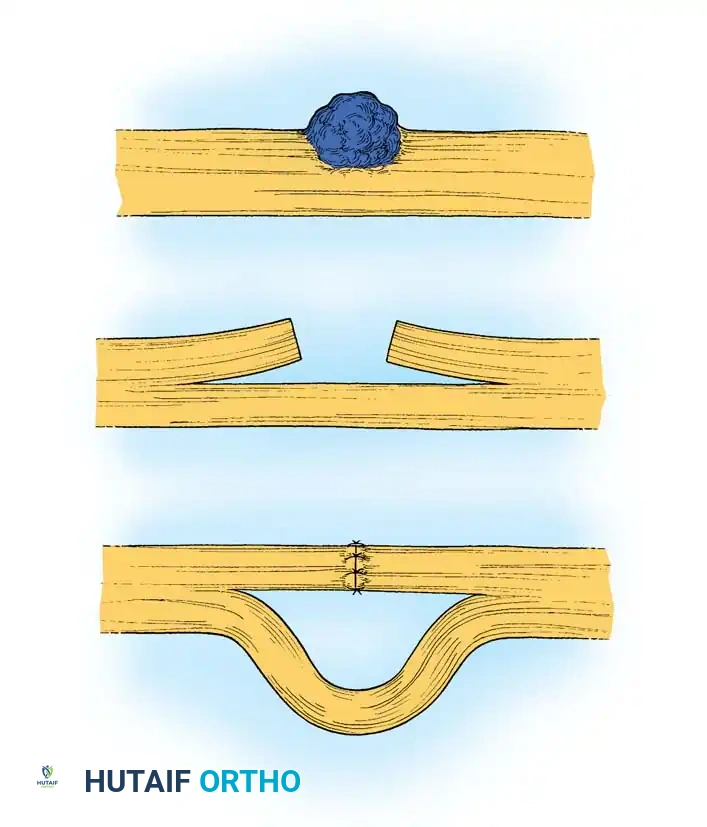
The image above illustrates the resection of a neuroma and the subsequent attempt at end-to-end repair. Note that excessive tension or extreme joint flexion used to close a large gap leads to ischemia, intraneural fibrosis, and ultimate failure of regeneration.
Using a specialized diamond nerve knife or ultra-sharp microscissors, the surgeon performs serial "bread-loaf" sections of the proximal neuroma and distal glioma. The cross-section is examined under high magnification. A healthy nerve end is characterized by a lack of interfascicular fibrosis, distinct perineurial rings, and fascicles that herniate slightly outward ("mushrooming") due to normal endoneurial pressure. If any dense scar tissue, hemorrhage, or foreign material remains, further resection is mandatory.
Coaptation Techniques
The choice between epineurial and group fascicular repair depends on the internal topography of the nerve at the level of injury.
- Epineurial Repair: This technique is indicated for pure motor or pure sensory nerves, or sharply lacerated mixed nerves where the topographical alignment perfectly matches. The epineurium is approximated using interrupted 8-0 or 9-0 non-absorbable monofilament sutures (e.g., nylon). The initial two sutures are placed exactly 180 degrees apart, utilizing surface landmarks such as longitudinal epineurial blood vessels to ensure correct rotational alignment.
- Group Fascicular Repair: This technique is strictly indicated for mixed nerves (e.g., the median or ulnar nerve at the wrist) where distinct motor and sensory fascicular groups can be anatomically or electrophysiologically identified.
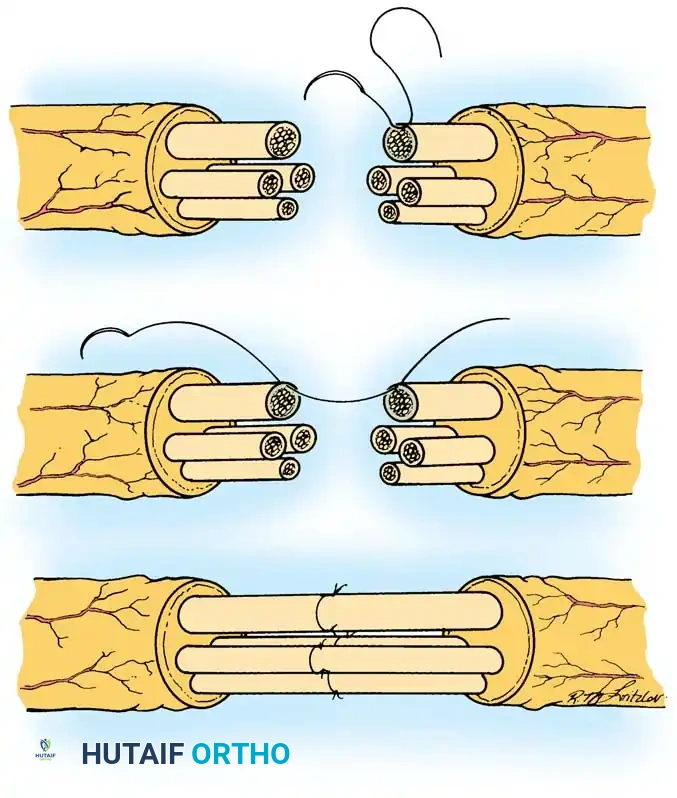
The image above demonstrates the technique of group fascicular repair. Precise alignment of corresponding motor and sensory fascicular groups is paramount to prevent axonal cross-innervation and ensure functional recovery.
Under high magnification, the interfascicular epineurium is carefully dissected to isolate matching groups of fascicles. Sutures (10-0 nylon) are meticulously placed through the perineurium of matching groups. This technique minimizes axonal misdirection but requires extensive intraneural dissection, which can theoretically increase localized scarring if performed aggressively.
Interfascicular Nerve Grafting
When a tension-free primary repair cannot be achieved—defined by Millesi as a gap exceeding 2.5 cm after maximal safe mobilization, or the inability of an 8-0 nylon suture to hold the nerve ends together without tearing—an autologous interfascicular nerve graft is strictly indicated. The sural nerve is the premier donor graft due to its expendability, favorable fascicular architecture, and available length (up to 40 cm).
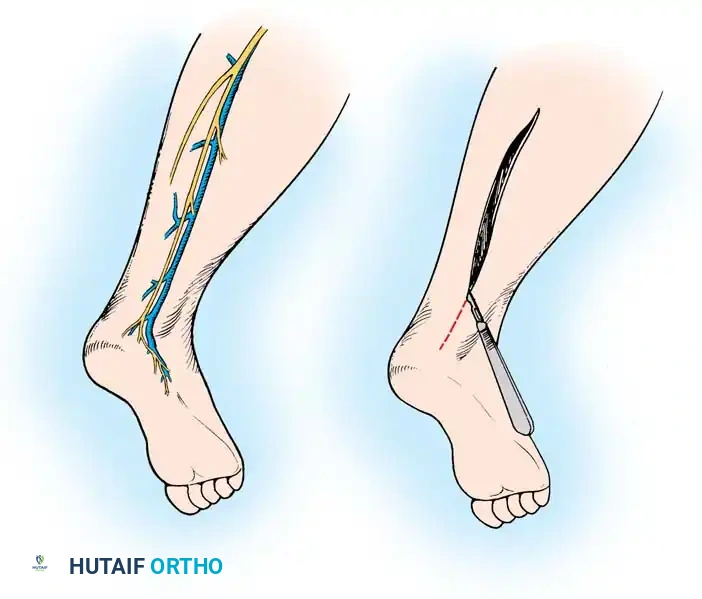
The image above depicts the surgical approach for harvesting the sural nerve. A longitudinal or step-ladder incision is made along the posterolateral calf, tracing the nerve alongside the lesser saphenous vein.
Sural Nerve Harvest Steps:
1. Identify the sural nerve immediately posterior to the lateral malleolus.
2. Make a longitudinal incision or a series of step-ladder incisions tracking proximally toward the popliteal fossa. Avoid blind stripping with a tendon stripper, as this causes severe traction injury and avulsion of the delicate fascicles.
3. Carefully dissect the nerve from the lesser saphenous vein, meticulously ligating crossing venous branches with micro-clips or bipolar electrocautery.
4. Transect the nerve sharply at the required length.
5. Critical Step: The harvested graft must be reversed during interposition. Because peripheral nerves naturally branch as they proceed distally, reversing the graft ensures that regenerating axons are channeled toward the distal target rather than escaping into severed side branches within the graft.
6. The graft is divided into multiple cables to match the cross-sectional area of the injured nerve. The cables are sutured in place using 10-0 nylon under zero tension. Fibrin glue may be utilized to augment the repair and seal the coaptation site, reducing the number of required sutures and minimizing foreign body reaction.
Complications, Incidence Rates, and Salvage Management
Despite flawless microsurgical execution, peripheral nerve repairs are fraught with complex complications. The biological limitations of axonal regeneration, combined with the hostile environment of traumatized soft tissue, frequently result in suboptimal functional outcomes. The surgeon must be profoundly aware of these complications, their incidence, and the definitive salvage pathways.
Neuroma-in-continuity represents one of the most challenging complications. It occurs when regenerating axons escape the confines of the epineurium at the coaptation site, or when dense intraneural scarring completely blocks axonal progression, resulting in a disorganized, highly sensitive mass of axons, Schwann cells, and fibroblasts. Clinically, this presents as an arrested Tinel’s sign that fails to advance distally at the expected rate of 1 mm per day, accompanied by severe, localized neuropathic pain.
Failure of regeneration is a catastrophic complication driven by excessive tension, inadequate resection of the initial neuroma, profound ischemia, or extreme delay in surgical intervention leading to irreversible motor endplate degradation. Proximal injuries (e.g., brachial plexus trauma) carry a significantly higher incidence of failure due to the massive distance regenerating axons must traverse before reaching distal targets.
Complex Regional Pain Syndrome (CRPS) Type II (Causalgia) is a devastating, sympathetically maintained pain syndrome triggered by partial nerve injuries or neuromas. It is characterized by burning neuropathic pain out of proportion to the injury, severe allodynia, hyperpathia, and profound sudomotor and vasomotor changes (edema, temperature asymmetry, trophic skin changes).
| Complication | Estimated Incidence | Pathophysiology / Etiology | Salvage Management Strategy |
|---|---|---|---|
| Neuroma-in-Continuity | 15% - 25% | Axonal escape at coaptation, intraneural scarring, excessive tension. | Resection of neuroma and interfascicular nerve grafting; wrapping with vascularized fascial flaps. |
| Failure of Motor Regeneration | 20% - 40% (varies by level) | Motor endplate degradation (>12-18 months denervation), severe ischemia, gap. | Tendon transfers, free functional muscle transfers (FFMT), regional nerve transfers (neurotization). |
| CRPS Type II (Causalgia) | 5% - 15% | Sympathetically maintained pain loop, partial nerve injury, hyperactive nociceptors. | Aggressive multimodal pain management, sympathetic blocks, targeted neuroma resection, spinal cord stimulation. |
| Deep Surgical Site Infection | 2% - 5% | Contaminated wound bed, prolonged operative time, ischemic soft tissue. | Aggressive serial I&D, targeted IV antibiotics, removal of non-absorbable sutures if grossly infected. |
Salvage management requires a paradigm shift from nerve repair to functional reconstruction. When nerve regeneration definitively fails, or when the time to target exceeds the viability of the motor endplates, tendon transfers become the primary reconstructive option. For example, in an irreversible high radial nerve palsy, the standard salvage involves transferring the Pronator Teres to the Extensor Carpi Radialis Brevis (wrist extension), Flexor Carpi Radialis to Extensor Digitorum Communis (finger extension), and Palmaris Longus to Extensor Pollicis Longus (thumb extension). In modern reconstructive microsurgery, distal nerve transfers (e.g., transferring a redundant fascicle of the median nerve to the extensor carpi radialis brevis branch of the radial nerve) have revolutionized salvage paradigms, allowing for targeted reinnervation close to the motor endplates before irreversible atrophy occurs.
Phased Post-Operative Rehabilitation Protocols
The success of a flawless microsurgical repair can be entirely undone by improper post-operative care. Rehabilitation following peripheral nerve repair is a highly structured, multidisciplinary endeavor requiring seamless communication between the orthopedic surgeon and specialized hand or neuro-physiotherapists. The protocol is divided into distinct, biologically driven phases.
Phase I: Immobilization and Protection (Weeks 0 to 3)
Immediately post-operatively, the limb is immobilized in a custom, well-padded plaster or thermoplastic splint. The primary objective is absolute protection of the microvascular coaptation site from any tensile stress. The joints are positioned in a neutral, relaxed posture. Historically, limbs were placed in extreme flexion to close massive gaps; however, this is now strictly condemned as it leads to catastrophic joint contractures and guarantees severe nerve traction upon mobilization. Elevation and strict edema control are mandatory to prevent microvascular compromise of the surrounding soft-tissue envelope.
Phase II: Early Progressive Mobilization (Weeks 3 to 6)
At 3 weeks, the initial biological healing of the epineurium is sufficient to withstand mild stress. The static splint is removed, and a supervised, highly controlled progressive active and passive Range of Motion (ROM) program is initiated. A hinged dynamic brace is often utilized to gradually increase extension by 10 to 15 degrees per week, preventing sudden traction on the regenerating nerve. Passive ROM of paralyzed joints is critical to maintain capsular suppleness and prevent fixed flexion or extension contractures that would render eventual muscle reinnervation functionally useless.
Phase III: Sensory Re-education and Desensitization (Weeks 6 to 12+)
As the advancing Tinel’s sign reaches the distal targets and early protective sensation returns, formal sensory re-education protocols are instituted. Because regenerating axons frequently misdirect into incorrect endoneurial tubes, the cerebral cortex receives chaotic, disorganized sensory input. Sensory re-education utilizes neuroplasticity to remap the somatosensory cortex. Patients undergo structured exercises involving the identification of varying textures, shapes, temperatures, and weights with their eyes closed. Concurrently, desensitization techniques (using progressively coarser materials and vibration) are employed to manage hyperalgesia and allodynia at the surgical site and advancing nerve front.
Phase IV: Motor Re-education and Strengthening (Months 3 to 24)
As voluntary muscle contraction returns (initially detectable only via EMG, then clinically as a flicker of movement), motor re-education begins. The use of electrical stimulation on denervated muscle remains highly controversial; while it may slow muscle atrophy, some evidence suggests it can inhibit the terminal sprouting of regenerating axons. Instead, the focus is on active-assisted exercises, biofeedback, and the
