INTRODUCTION TO NAIL PATHOLOGIES IN ORTHOPAEDICS
Disorders of the nail unit, while frequently perceived as minor dermatological or cosmetic issues, can precipitate severe morbidity in the orthopedic patient population. In the context of foot and ankle surgery, the management of dystrophic nails—specifically onychogryposis and onychomycosis—and structural lesions such as subungual exostosis requires a comprehensive understanding of phalangeal biomechanics, nail matrix anatomy, and underlying systemic comorbidities.
Deformed nails in elderly, diabetic, or neuropathic patients can be exceedingly difficult to manage at best, and catastrophic at worst. In an insensitive foot, a hypertrophic nail acts as a rigid lever arm against the shoe toe-box, translating sheer and compressive forces directly into the underlying nail bed. This focal pressure frequently leads to subungual ulceration, secondary bacterial infection, and ultimately, distal phalangeal osteomyelitis. Consequently, the orthopedic surgeon must be adept at both the conservative and surgical management of these pathologies to prevent limb-threatening complications.
DYSTROPHIC NAILS: ONYCHOGRYPOSIS AND ONYCHOMYCOSIS
Pathophysiology and Clinical Presentation
Onychogryposis
Onychogryposis, colloquially referred to as "ram's horn nails," is an acquired dystrophy characterized by asymmetrical, extreme hypertrophy, elongation, and curvature of the nail plate. It is most commonly observed in the hallux of elderly patients. The etiology is multifactorial, typically stemming from chronic microtrauma, poor footwear, peripheral vascular disease, or neglect. The asymmetrical growth of the nail matrix leads to the characteristic spiraling deformity.

Onychomycosis
Onychomycosis is a fungal infection of the nail unit, predominantly caused by dermatophytes (e.g., Trichophyton rubrum), yeasts, or non-dermatophyte molds. It presents as nail plate discoloration (yellow-brown), subungual hyperkeratosis, and onycholysis (separation of the nail plate from the bed). While primarily a cosmetic concern in healthy individuals, the resulting hyperkeratosis thickens the nail, mimicking the mechanical dangers of onychogryposis in the diabetic foot.
💡 Clinical Pearl: The Neuropathic Foot
In patients with peripheral neuropathy, a dystrophic nail is not a cosmetic issue—it is a pre-ulcerative lesion. The rigid, thickened nail plate fails to accommodate within standard footwear, driving the distal phalanx downward and creating a high-pressure nidus at the tip of the toe. Prophylactic reduction is mandatory to prevent subungual ulceration.
Non-Operative and Medical Management
Other than the mechanical reduction of the nail mass, onychomycosis can often be treated with "benign neglect" in asymptomatic, neuro-intact patients, as its primary effect is cosmetic.
If the patient desires eradication of the fungal infection, a multidisciplinary approach is highly recommended:
* Dermatological Referral: Referral to a dermatologist is warranted to obtain appropriate periodic acid-Schiff (PAS) stains and fungal cultures.
* Pharmacotherapy: Medical treatment involves topical agents (e.g., efinaconazole, ciclopirox) or oral agents (e.g., terbinafine, itraconazole).
* Monitoring: Most treatment regimens are prolonged (often 3 to 12 months) due to the slow growth rate of the nail plate and the difficulty medications face in penetrating the keratinized nail. Furthermore, oral antifungal medications carry risks of severe hepatotoxicity and drug interactions. Patients must undergo baseline and serial hepatic function monitoring.
Office-Based Surgical Reduction
For immediate relief of mechanical symptoms, particularly in the elderly or neuropathic patient, office-based reduction of the nail mass is highly effective.
Instrumentation Required:
* Heavy-duty double-action bone rongeur (Luer or Stille-Luer).
* English anvil nail splitter-cutter.
* Electric podiatric burr or Dremel tool (optional, for smoothing).
Reduction Technique:
1. Preparation: Soften the nail if possible (warm water soak or urea-based creams applied days prior).
2. Debulking: Utilize the double-action rongeur to systematically bite away the hypertrophic dorsal mass of the nail. Care must be taken not to avulse the nail plate from the underlying matrix, which can cause severe pain and bleeding.
3. Trimming: Use the nail splitter-cutter to trim the distal and lateral margins, ensuring no sharp spicules remain that could lacerate adjacent toes.
4. Smoothing: The remaining nail plate is filed or burred down to a normal physiological thickness, eliminating the mechanical lever arm.

These nails can be reduced quickly and safely in the outpatient clinic, immediately neutralizing the risk of pressure-induced ulceration.
SUBUNGUAL EXOSTOSIS
Pathology and Demographics
Strictly speaking, a subungual exostosis is not a primary nail abnormality; however, it invariably presents as a painful, deformed, and elevated nail, frequently leaving the uninitiated examiner perplexed as to the root cause of the deformity.
Subungual exostosis is a benign, sessile osteocartilaginous tumor (a variant of an osteochondroma) that arises from the dorsal aspect of the distal phalanx. It is most commonly seen in adolescents and young adults, with a slight female predilection. The hallux is involved in over 70% of cases. As the exostosis grows, it erodes dorsally through the nail matrix and frequently penetrates the nail plate itself, leading to severe pain, onycholysis, and secondary infection.

Clinical and Radiographic Evaluation
Clinical Presentation:
Patients typically present with a firm, exquisitely tender nodule emerging from beneath the distal or lateral margin of the nail plate. The overlying nail is pushed upward and may be partially destroyed. The lesion often features a hyperkeratotic or ulcerated cap due to chronic friction against footwear.
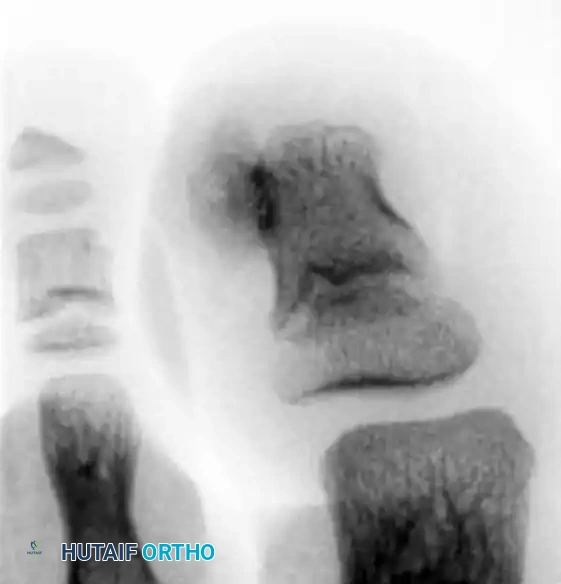
Radiographic Imaging:
Routine weight-bearing radiographs of the foot may completely miss the exostosis because standard anteroposterior (AP) and lateral techniques do not adequately isolate or emphasize the distal phalanx.
⚠️ Surgical Warning: Imaging Pitfalls
Never rely solely on standard foot series to rule out a subungual exostosis. Radiographs must be taken at oblique angles, specifically targeting the distal phalanx, and should be magnified. A true lateral of the isolated digit is the most sensitive view for identifying the dorsal bony outgrowth.
Surgical Management Principles
Surgical excision is the definitive treatment of choice. The primary goal is complete marginal resection of the exostosis, including its cartilaginous cap, to prevent recurrence, while simultaneously attempting to preserve as much of the normal nail bed anatomy as possible to ensure a cosmetically acceptable postoperative nail.
Two primary surgical techniques are utilized, depending on the size of the lesion and the degree of nail bed destruction.
SURGICAL TECHNIQUE I: The Lokiec et al. Approach (Nail Preservation)
This technique is highly effective for laterally or medially based exostoses where the central nail matrix remains intact. It emphasizes the preservation of the nail plate to act as a biological dressing and splint for the repairing nail bed.
Preoperative Preparation
- Anesthesia: Administer general anesthesia for young children or a comprehensive digital/ankle block for adolescents and adults.
- Hemostasis: Apply a digital tourniquet (e.g., a sterile Penrose drain clamped at the base of the toe) or an ankle tourniquet to ensure a bloodless surgical field. Exsanguinate the digit prior to inflation.
Step-by-Step Procedure
- Partial Nail Avulsion: Remove a narrow strip of the nail (less than one-fourth of the total nail width) on the side of the toe corresponding to the lesion (medial or lateral) to expose the exostosis.
- Nail Plate Elevation: Carefully introduce a Freer elevator to dislodge part of the remaining nail from its proximal attachments at the larger side of the exostosis. Leave the remainder of the nail firmly in place. This maneuver fully exposes the exostosis that is abutting and penetrating the nail bed.
- Osteotomy: Utilize a fine osteotome or a microsagittal saw. Make a small osteotomy strictly parallel to the dorsal cortex of the distal phalanx. The objective is to remove the exostosis flush with the normal bone in one complete piece.
- Debridement and Contouring: Use a fine Luer rongeur or a high-speed diamond burr to produce a perfectly smooth cortical surface. It is critical to remove any residual osteochondroma tissue or cartilaginous cap, as retained cartilage is the primary cause of recurrence.
- Closure and Reconstruction: Irrigate the wound copiously with sterile saline to remove bone debris. Relocate the elevated nail plate back over the nail bed. Suture the nail fold with two small absorbable stitches (e.g., 5-0 Vicryl or chromic gut) to secure the nail and cover the raw bone of the phalanx.
SURGICAL TECHNIQUE II: The Multhopp-Stephens and Walling Approach (Complete Excision)
This more aggressive approach is indicated for large, centrally located exostoses that have completely destroyed the overlying nail bed, or for recurrent lesions where aggressive resection is required.
Preoperative Preparation
- Anesthesia: Digital block (Mayo block) utilizing 1% Lidocaine and 0.5% Bupivacaine without epinephrine.
- Hemostasis: Digital tourniquet applied at the base of the hallux.
Step-by-Step Procedure
- Exposure: Expose the lesion by removing a significant portion of the nail, or perform a total nail avulsion if the exostosis is central and massive.
- Incision and Dissection: Create an elliptical incision directly around the exostosis. Carry the sharp dissection down through the soft tissues directly to the dorsal cortex of the distal phalanx where the stalk or base of the exostosis is attached.
- Crucial Step: Do not attempt to preserve the overlying, severely damaged nail bed. Attempting to dissect the nail bed off the cartilaginous cap often leaves microscopic cartilage cells behind, guaranteeing recurrence.
- Resection: Remove the exostosis en bloc, which must include the cartilaginous cap and the overlying adherent nail bed at its base, freeing it from the distal phalanx.
- Bone Contouring: Use a small high-speed burr to aggressively remove 1 to 2 mm of normal-appearing bone at the base of the lesion. Smooth the dorsal contour of the distal phalanx to ensure no microscopic stalk remains.
- Wound Management: Deflate the tourniquet and obtain meticulous hemostasis. The resulting nail bed defect is typically left to heal by secondary intention, or if large enough, can be covered with a non-adherent dressing. Primary closure is rarely possible without undue tension.
🔪 Surgical Pitfall: Incomplete Resection
The recurrence rate for subungual exostosis can be as high as 10-15% if the cartilaginous cap is not entirely excised. The surgeon must not compromise the oncologic margin of this benign tumor for the sake of preserving the nail bed. Always burr down 1-2 mm into the normal dorsal cortex.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Immediate Postoperative Care
- Dressing: A non-adherent dressing (e.g., Adaptic or Xeroform) is applied directly over the exposed nail bed or retained nail plate. This is followed by sterile gauze and a mildly compressive cohesive bandage.
- Weight-Bearing: Patients are typically allowed to weight-bear as tolerated in a rigid-soled postoperative shoe or a controlled ankle motion (CAM) boot to protect the distal phalanx from microtrauma and sheer stress.
- Elevation: Strict elevation of the operative extremity above the level of the heart is mandated for the first 48 to 72 hours to minimize throbbing pain and edema.
Outpatient Follow-Up
- First Visit (Days 5-7): The initial bulky dressing is removed. The wound is inspected for signs of infection, hematoma, or necrosis. If the nail plate was retained (Lokiec technique), its stability is assessed.
- Wound Care: Patients are instructed to perform daily warm saline or dilute Betadine soaks, followed by the application of a topical antibiotic ointment and a simple adhesive bandage until the nail bed epithelializes.
- Long-Term Follow-Up: Patients should be monitored at 3 months and 6 months postoperatively. The new nail plate will take approximately 9 to 12 months to fully grow out from the germinal matrix to the hyponychium.
Complications
- Recurrence: The most common complication, resulting from incomplete excision of the cartilaginous cap. Requires revision surgery with a more aggressive burring of the distal phalanx.
- Nail Dystrophy: Permanent deformity of the new nail plate (e.g., splitting, ridging, or non-adherence) can occur if the germinal matrix was inadvertently damaged during the resection.
- Infection: Superficial nail bed infections can occur, particularly if the exostosis was ulcerated preoperatively. Managed with oral antibiotics and local wound care.
- Phalangeal Fracture: Overzealous use of the osteotome or burr can lead to an iatrogenic fracture of the distal phalanx tuft. This is usually managed conservatively with a rigid splint but prolongs recovery.
