INTRODUCTION AND HISTORICAL CONTEXT
The management of recalcitrant nonunions, particularly congenital pseudarthrosis of the tibia (CPT) and osteoporotic periarticular nonunions, remains one of the most formidable challenges in orthopedic surgery. Because union in congenital pseudarthrosis of the tibia is notoriously difficult to obtain due to inherent biological and mechanical deficiencies, H.B. Boyd devised the Dual Onlay Graft operation in 1941.
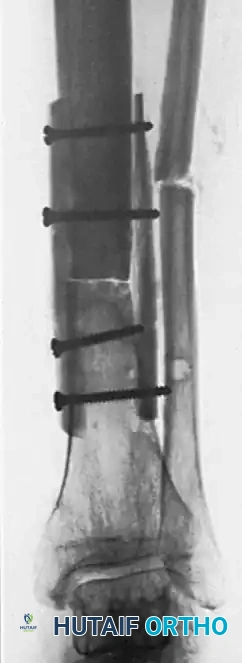
This ingenious technique utilizes two cortical onlay grafts placed opposite each other on the host bone, bridging the nonunion site. Fixed with a single set of through-and-through screws, the grafts grip the host bone fragments like a vise. Any intervening space at the bone ends is meticulously packed with cancellous bone chips to provide osteogenic and osteoconductive properties.
While the advent of modern locked plating, intramedullary nailing, and circular external fixation (Ilizarov methods) has reduced the frequency of this procedure, the dual onlay graft remains an indispensable salvage technique in the armamentarium of the reconstructive orthopedic surgeon. It is particularly valuable in scenarios of severe osteoporosis where standard metallic implants fail to achieve adequate purchase.
INDICATIONS AND CONTRAINDICATIONS
Primary Indications
- Congenital Pseudarthrosis of the Tibia (CPT): Historically the primary indication, providing massive structural support and biological stimulation to a biologically inert and mechanically unstable segment.
- Osteoporotic Nonunions in the Elderly: Used in old nonunions of the shafts of long bones where the host cortex is paper-thin and severely osteoporotic. Standard screws will strip and fail in such fragments; however, they achieve excellent purchase in the dense cortical bone of the dual autografts or allografts.
- Short Juxta-Articular Nonunions: When a nonunion occurs near a joint, the short metaphyseal fragment is often osteoporotic and difficult to control. The short fragment is grasped between the ends of the two grafts, with screws seated securely in the strong cortical bone of each graft, compressing the osteoporotic host bone between them.

💡 Clinical Pearl: Modern Alternatives
While dual grafts provide excellent fixation for nonunions near a joint, contemporary practice often favors the use of anatomically contoured locked plating combined with autogenous cancellous bone grafting, or the application of a circular external fixator (e.g., Taylor Spatial Frame) to achieve compression and stability without extensive soft tissue stripping. The dual onlay graft is reserved for cases where these modern modalities have failed or are contraindicated due to massive bone loss or catastrophic implant failure.
Contraindications
- Active Infection: The presence of a massive cortical graft in an infected bed is a recipe for disaster, leading to sequestration and chronic osteomyelitis.
- Severe Soft Tissue Compromise: Two bulky cortical grafts materially crowd the soft tissues. If the soft tissue envelope is inadequate to achieve tension-free closure, the procedure is contraindicated unless combined with a vascularized soft tissue flap.
- Inadequate Host Bone Stock for Graft Harvest: If autograft is planned, the patient must have a healthy donor tibia.
BIOMECHANICAL PRINCIPLES
The biomechanical superiority of the dual onlay graft lies in its vise-like compression and load-sharing capabilities.
When screws are inserted through the first cortical graft, through the osteoporotic host bone, and into the second cortical graft, the host bone is subjected to significant compressive forces. The dense cortical grafts act as massive washers, preventing the screw heads and threads from pulling through the weak host bone.
Furthermore, placing two cortical struts on opposite sides of the mechanical axis significantly increases the area moment of inertia, providing exceptional resistance to bending and torsional forces. The construct effectively bypasses the mechanically incompetent nonunion site, transferring loads through the rigid cortical grafts until creeping substitution and bony consolidation occur.

PREOPERATIVE PLANNING
Meticulous preoperative planning is mandatory to prevent intraoperative complications, particularly regarding soft tissue management.
- Imaging: Obtain orthogonal radiographs and a fine-cut Computed Tomography (CT) scan of the nonunion site to assess bone stock, defect size, and the geometry of the host fragments.
- Graft Sizing: Calculate the required length and width of the grafts. The grafts must be long enough to allow at least two (preferably three) screws in each host fragment above and below the nonunion.
- Soft Tissue Assessment: Evaluate the pliability of the skin and subcutaneous tissues. The addition of two cortical struts will increase the cross-sectional area of the limb. Ensure that closure will be possible without excessive tension.
- Logistics: Plan for a two-team approach to minimize tourniquet time and overall operative duration. One team prepares the recipient site while the second team harvests the graft.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Exposure and Debridement of the Nonunion
Expose the defect in the bone through an extensile approach that respects angiosomes and previous surgical incisions.
* Perform a radical debridement. Excise all necrotic, avascular, and sclerotic tissue until healthy, bleeding bone is encountered (the "paprika sign").
* Open the medullary canals of both the proximal and distal fragments using drill bits or curettes to restore endosteal blood flow.
⚠️ Surgical Warning: Soft Tissue Crowding
Decide early which two opposite surfaces will hold the grafts most smoothly and from what direction the screws can be most skillfully inserted. Two cortical grafts will materially crowd the soft tissues. Unless well planned, they may interfere with neurovascular structures or make skin closure impossible.
2. Preparation of the Host Bed
Using a sharp, broad osteotome or an oscillating saw, prepare flat beds for the grafts on the chosen opposite sides of the host fragments.
* Do not countersink the beds deeply or expose the medullary canal excessively during this step.
* Remove just enough cortical bone to create a perfectly flat surface, allowing the rigid cortical grafts to be applied flush without bending or gapping.
3. Graft Harvesting (Two-Team Approach)
While the primary surgeon is preparing the host region, a second surgical team harvests the grafts to minimize operative time.
* Expose the donor tibial shaft (usually the contralateral leg).
* Harvest a massive, full-thickness cortical graft using an oscillating saw, ensuring the corners of the harvest site are rounded with a drill to prevent stress risers and subsequent donor site fracture.
* From the proximal tibial metaphysis (Gerdy's tubercle), harvest additional copious cancellous bone fragments.
4. Graft Preparation
Once the massive cortical strut is passed to the back table:
* Using an oscillating saw, carefully remove the cancellous surface of the graft. Preserve this highly osteogenic cancellous bone for future use in packing the defect.
* Divide the cortical graft transversely (if harvested long enough) or split it longitudinally to form two identical, robust cortical struts.
5. Application and Provisional Fixation
Place the two prepared cortical grafts on the opposite, flattened sides of the host fragments, bridging the defect.
* Hold the entire construct together with large, self-retaining bone-holding forceps (e.g., Verbrugge or Lewin clamps).
* Make any minor adjustments in their alignment. Ensure that the mechanical axis is correct and restore the length of the extremity as much as possible.

6. Definitive Fixation (The Alternating Screw Technique)
Fixing two unyielding cortical grafts to a mobile nonunion requires a specific, sequential technique to maintain compression and alignment. Fix the two grafts one at a time as follows:
- Provisional Short Screws: Drill and tap through the first graft and the near cortex of the host bone. Fix this first graft to both the proximal and distal host fragments using short temporary screws. This stabilizes the first graft and the host bone as a single unit.
- Definitive Long Screws: Move to the second graft. Drill through the second graft, through both cortices of the intervening host fragments, and into the first graft. Insert fully threaded cortical screws (typically 3.5mm or 4.5mm depending on the bone) that are long enough to pass through all four cortices (Graft 2 -> Host Near Cortex -> Host Far Cortex -> Graft 1).
- Screw Exchange: Once the second graft is secured with long screws, remove the short temporary screws from the first graft. Re-drill these holes through the host bone and into the second graft, and replace them with definitive long screws that pass completely through the entire construct.
💡 Clinical Pearl: Screw Purchase
In severely osteoporotic bone, the host fragments provide almost no screw purchase. The mechanical integrity of this construct relies entirely on the threads gripping the dense cortical bone of the two grafts. Ensure the drill bit and tap are perfectly sized for the chosen screws to maximize pull-out strength in the grafts.
7. Cancellous Bone Grafting
The rigid cortical grafts provide structural stability but are slow to incorporate. Biological stimulation is provided by cancellous bone.
* Meticulously fill the defect between the host fragments with the cancellous bone harvested from the proximal tibia and the cancellous scrapings from the grafts.
* If the defect is large, use additional autogenous iliac crest bone graft (ICBG) or allograft cancellous chips mixed with bone marrow aspirate concentrate (BMAC).
* Bridging Long Defects: When bridging long segmental defects, leave the cancellous bone attached to the part of each graft that spans the empty defect, but remove it from the parts that overlap and sit flush against the host fragments.

8. Closure
Deflate the tourniquet and achieve meticulous hemostasis. Because the limb volume has been increased by the grafts, close the deep fascia only if it does not cause tension. Close the subcutaneous tissue and skin carefully over closed suction drains. If skin closure is excessively tight, consider prophylactic fasciotomies or a local rotational flap.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative management of a dual onlay graft is characterized by extreme patience. Massive cortical grafts undergo incorporation via creeping substitution—a process where osteoclasts resorb the dead graft bone while osteoblasts simultaneously lay down new host bone. During this phase, the graft actually becomes temporarily weaker before it becomes stronger.
- Immobilization: The limb is typically placed in a well-padded, long-leg cast or a rigid custom orthosis immediately postoperatively.
- Weight-Bearing Restrictions: Dual grafts on weight-bearing bones must be protected for a significantly long time because they are slow to revascularize. Strict non-weight-bearing is enforced initially.
- Radiographic Monitoring: Serial radiographs are obtained at 6-week intervals.
- Progression: Unprotected weight-bearing should not be allowed until mature trabeculations are clearly seen crossing the defect and bridging the host bone to the grafts on multiple radiographic views. This process frequently takes 6 to 12 months.

COMPLICATIONS AND PITFALLS
- Soft Tissue Necrosis: The most immediate threat. Excessive tension on the skin over the bulky grafts can lead to wound breakdown, exposing the avascular bone grafts to infection.
- Infection: Deep infection in the presence of massive cortical autografts usually necessitates complete removal of the grafts, resulting in a massive segmental defect.
- Graft Fracture: During the creeping substitution phase, the grafts are mechanically vulnerable. Premature weight-bearing can lead to catastrophic fracture of the grafts.
- Donor Site Morbidity: Harvesting a massive cortical strut from the tibia carries risks of tibial plateau fracture, diaphyseal stress fracture, and hematoma. Prophylactic restriction of activities for the donor leg is required.
CONCLUSION
The dual onlay graft remains a masterclass in orthopedic biomechanics. By effectively sandwiching mechanically compromised bone between two rigid, biologically active struts, the surgeon can achieve stability in situations where modern implants would inevitably fail. While technically demanding and requiring meticulous soft-tissue management and prolonged postoperative protection, mastering this technique provides the reconstructive surgeon with a powerful tool for limb salvage in the face of the most daunting nonunions.
