Introduction & Epidemiology
Infections of the deep fascial spaces of the hand, while less common than superficial infections, represent critical surgical emergencies requiring prompt diagnosis and intervention to prevent debilitating sequelae. The lateral, or thenar, space is one such critical anatomical region prone to abscess formation. Infections in this space can arise from various etiologies, including direct penetrating trauma, spread from contiguous infections such as paronychia or felons, or through tenosynovitis of the flexor pollicis longus (FPL) tendon sheath, particularly if the distal extent of Parona's space communicates with the thenar space.
The incidence of specific deep space infections like thenar space abscesses is not extensively reported in isolation but is encompassed within the broader category of severe hand infections. A delay in diagnosis or inadequate treatment can lead to significant morbidity, including widespread fascial necrosis, septic arthritis, osteomyelitis, permanent digital stiffness, contractures, nerve damage, and in severe cases, systemic sepsis. The unique anatomical constraints and vital neurovascular structures within the thenar region necessitate a thorough understanding of its surgical anatomy for effective and safe drainage. Early and accurate surgical drainage, coupled with appropriate antibiotic therapy, remains the cornerstone of management.
Surgical Anatomy & Biomechanics
A precise understanding of the surgical anatomy of the thenar space is paramount for effective and safe drainage. The thenar space is one of the three major deep fascial spaces of the hand (along with the midpalmar space and Parona's space). Its boundaries are well-defined:
- Radial Border: Formed by the thenar septum, a fibrous partition extending from the palmar aponeurosis to the palmar surface of the third metacarpal.
- Ulnar Border: Defined by the midpalmar septum, which originates from the palmar aponeurosis and inserts onto the palmar surfaces of the fourth and fifth metacarpals, separating the thenar space from the midpalmar space.
- Dorsal Floor: Composed of the adductor pollicis muscle, the first dorsal interosseous muscle, and the metacarpal bones.
- Volar Roof: Consists primarily of the flexor pollicis longus tendon sheath and the intrinsic thenar muscles (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis). The deep surface of these thenar muscles contribute to the volar boundary.
- Proximal Border: The distal aspect of the flexor retinaculum and the carpal tunnel.
- Distal Border: The first web space and the base of the thumb.
The lateral (thenar) space typically contains the flexor pollicis longus tendon and its associated synovial sheath, the first metacarpal, and the adductor pollicis muscle. Infections within this space are often characterized by significant swelling of the thenar eminence, severe pain with thumb movement, and palpable tenderness. The relationship of the thenar space to other structures is crucial. Infections can spread to or from the flexor pollicis longus tendon sheath (Kanavel's sign if purulent tenosynovitis). Communication with the first web space distally is common, and rarely, infections can track proximally to Parona's space.
Critical Neurovascular Structures
Several critical neurovascular structures traverse or lie adjacent to the operative field during thenar space drainage, requiring meticulous dissection:
- Digital Nerves to the Index Finger: The common palmar digital nerve to the radial side of the index finger and the proper palmar digital nerve to the ulnar side of the index finger (arising from the common palmar digital nerve) are located superficially within the subcutaneous tissue along the ulnar side of the thenar crease. These nerves are directly in line with the initial skin incision and must be identified and preserved to avoid permanent sensory deficits.
- Recurrent Motor Branch of the Median Nerve (Thenar Motor Branch): This vital nerve innervates the thenar muscles (abductor pollicis brevis, opponens pollicis, and superficial head of the flexor pollicis brevis). Its origin from the median nerve as it exits the carpal tunnel is highly variable. It classically hooks around the distal edge of the flexor retinaculum, often lying superficial to the thenar muscles but deep to the palmar aponeurosis. Identifying this branch proximally in the incision is crucial to avoid iatrogenic injury, which would result in significant thumb weakness and impaired opposition. The variability in its course underscores the need for careful, layered dissection.
- Superficial Palmar Arch: While generally deeper and more centrally located, branches of the superficial palmar arch, particularly the radial digital artery to the index finger and the princeps pollicis artery, may be at risk during deeper dissection, especially in cases of extensive inflammation and anatomical distortion.
The absence of a true internervous plane in the standard approach implies that nerves will be encountered during dissection and must be carefully identified and protected. The flexor digitorum superficialis (FDS) tendon to the index finger serves as a key anatomical landmark, as the thenar space lies deep to it in this approach.
Indications & Contraindications
Effective management of thenar space infections hinges on timely and accurate identification of surgical indications, while recognizing situations where non-operative measures are appropriate.
Indications for Operative Drainage
The primary indication for operative drainage is the presence of a confirmed abscess within the thenar space. Clinical and imaging findings guide this decision.
-
Clinical Findings:
- Localized, throbbing pain in the thenar eminence.
- Significant swelling and erythema over the thenar eminence.
- Tenderness to palpation.
- Fluctuance (though this may be difficult to elicit in deep, tense spaces).
- Restricted and painful thumb movement, particularly opposition and abduction.
- Systemic signs of infection (fever, chills, elevated white blood cell count, elevated inflammatory markers like ESR and CRP).
- Failure of conservative management (e.g., antibiotics for cellulitis without abscess formation).
-
Imaging Findings:
- Ultrasound: Highly useful for confirming the presence of a fluid collection, assessing its size and depth, identifying loculations, and guiding needle aspiration if attempted.
- MRI: Provides detailed anatomical information, delineating the extent of infection, differentiating abscess from cellulitis, and identifying potential osteomyelitis or septic arthritis in complex cases.
Contraindications for Operative Drainage
Absolute contraindications are rare, as untreated deep space infections can be limb and life-threatening. However, relative contraindications and situations favoring non-operative management include:
- Early Cellulitis Without Abscess Formation: In the absence of a distinct pus collection, a trial of appropriate intravenous antibiotics with close monitoring is indicated. Imaging (ultrasound) is crucial to differentiate cellulitis from abscess.
- Severe Coagulopathy: While not an absolute contraindication in an emergency, significant coagulopathy should be corrected pre-operatively if time permits, to minimize bleeding complications.
- Patient Refusal or Unfit for Surgery: In rare circumstances where a patient is medically unstable for surgery, alternative non-operative strategies may be considered, though this is generally reserved for palliation.
Table 1: Operative vs. Non-Operative Indications for Thenar Space Infection
| Feature | Operative Management (Drainage) | Non-Operative Management (Antibiotics, etc.) |
|---|---|---|
| Clinical Signs | Fluctuance, severe localized pain, significant swelling, systemic toxicity, failure of conservative therapy | Early erythema, mild tenderness, no palpable fluctuance, stable vital signs |
| Imaging (Ultrasound) | Hypoechoic fluid collection, irregular margins, internal debris, loculations | Diffuse subcutaneous edema, hypervascularity, no distinct fluid collection |
| Microbiology | Culture-positive pus on aspiration or drainage | Presumed bacterial infection based on clinical context |
| Duration of Symptoms | Typically 24-48+ hours with worsening signs | Usually < 24-48 hours, early presentation |
| Systemic Response | Fever, chills, leukocytosis, elevated inflammatory markers | Mild or absent systemic signs |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to optimize outcomes and minimize complications.
Pre-Operative Planning
- History and Physical Examination: A detailed history should include the mechanism of injury (if applicable), onset and progression of symptoms, previous hand infections, and systemic health status. Physical examination focuses on the extent of swelling, tenderness, range of motion limitations, and neurovascular assessment.
- Laboratory Studies: Complete blood count (CBC) with differential, erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) are useful inflammatory markers. Blood cultures should be considered for systemic signs of sepsis.
-
Imaging:
- Ultrasound: This is the preferred initial imaging modality. It can definitively identify a fluid collection, delineate its size and location, identify loculations, and aid in distinguishing cellulitis from abscess. It can also guide needle aspiration for diagnostic purposes (Gram stain and culture) prior to formal drainage.
- Magnetic Resonance Imaging (MRI): Reserved for more complex or atypical presentations, MRI offers superior soft tissue contrast and can accurately map the extent of infection, identify osteomyelitis, septic arthritis, or involvement of adjacent deep spaces, and differentiate pus from granulation tissue.
- Plain Radiographs: Primarily to rule out foreign bodies or underlying osteomyelitis, although their utility for soft tissue infection is limited.
- Antibiotic Prophylaxis/Therapy: Empiric broad-spectrum intravenous antibiotics should be initiated immediately upon diagnosis, covering common hand pathogens (e.g., Staphylococcus aureus , streptococci, Gram-negative bacilli, anaerobes, especially if animal or human bite). Antibiotic selection should be tailored based on local antibiogram data and subsequently adjusted according to intraoperative culture and sensitivity results.
- Informed Consent: Detailed discussion with the patient regarding the diagnosis, the need for surgical drainage, potential risks (nerve injury, incomplete drainage, stiffness, chronic pain, recurrence, need for further surgery), expected recovery, and alternative treatments.
Patient Positioning and Anesthesia
- Anesthesia: Regional anesthesia (e.g., axillary block) or general anesthesia is typically employed. Regional anesthesia offers excellent post-operative pain control and allows for intraoperative patient cooperation if needed (e.g., assessing nerve function in complex cases), though this is usually not feasible for an active infection.
- Patient Positioning: The patient is positioned supine, with the affected arm abducted on a sterile hand table. This provides optimal exposure and ergonomic access for the surgeon.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm and inflated after exsanguination with an Esmarch bandage. This ensures a bloodless field, which is critical for identifying delicate neurovascular structures and meticulously dissecting through inflamed tissues.
- Sterile Preparation and Draping: The hand and forearm are prepared with an antiseptic solution (e.g., povidone-iodine or chlorhexidine) and sterilely draped to expose the entire hand, wrist, and distal forearm.
Detailed Surgical Approach / Technique
The goal of surgical drainage of the lateral (thenar) space is to completely evacuate pus, debride necrotic tissue, break up loculations, and establish a pathway for ongoing drainage, while meticulously protecting vital neurovascular structures.
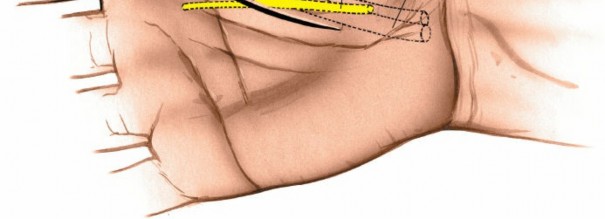
1. Incision
Make a curved incision approximately 4 cm long, situated just on the ulnar side of the thenar crease.
This specific placement is crucial. The curved nature of the incision follows the natural skin lines of the thenar eminence, promoting better wound healing and reducing scar contracture. Its position on the ulnar side of the thenar crease is chosen to avoid direct incision through the bulk of the thenar muscles and to provide optimal access to the lateral space while minimizing the risk of direct injury to the recurrent motor branch of the median nerve, which lies more radially.
2. Superficial Surgical Dissection
Deepen the dissection carefully in line with the initial skin incision through the subcutaneous fat.

At this superficial level, immediately identify and preserve the digital nerves to the index finger. These nerves, specifically the common palmar digital nerve to the radial side of the index finger, are located within the superficial subcutaneous tissue in the vicinity of the incision. Use fine dissecting scissors or a small scalpel with meticulous attention to detail. Retract these nerves gently.
There is no defined internervous plane in this approach, meaning nerves are encountered directly and must be identified and protected rather than dissected between fascial compartments.
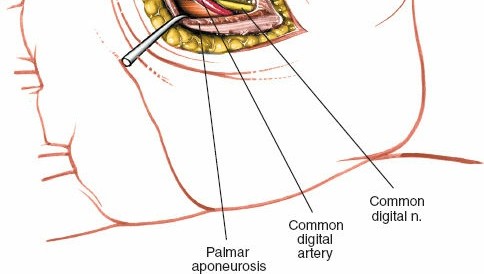
3. Identification of Key Anatomical Landmarks
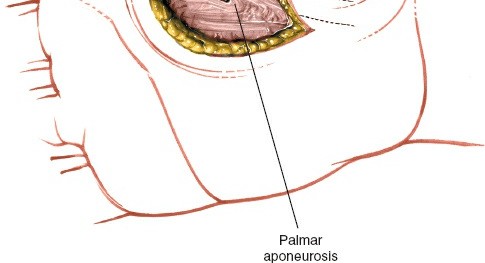
Continue careful dissection through the subcutaneous tissue and the palmar aponeurosis.
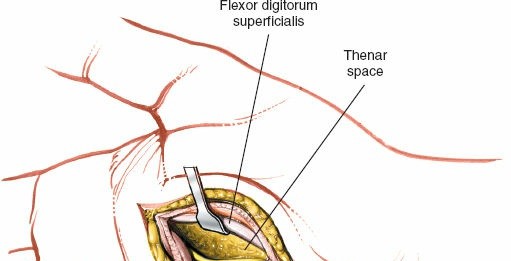
Identify the flexor digitorum superficialis (FDS) tendon to the index finger. This tendon serves as a critical landmark. It will be located deep to the subcutaneous tissue and generally superficial to the deeper structures of the thenar space.

Retract the digital nerves and vessels carefully.
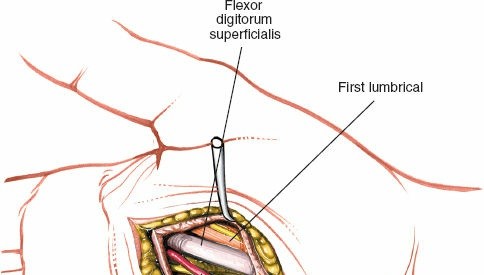
This image demonstrates a deeper view, likely showing the FDS tendon identified and retracted.
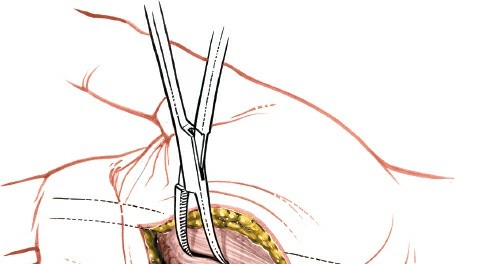
4. Entry into the Lateral Space
The lateral (thenar) space lies deep to the flexor digitorum superficialis tendon to the index finger.
Once the FDS tendon is identified and gently retracted radially, the thenar space can be entered by careful blunt dissection. A small curved hemostat, mosquito forceps, or a blunt-ended scissors can be used to penetrate the investing fascia and enter the purulent collection. The characteristic gush of pus confirms entry into the abscess cavity.
5. Drainage and Debridement
After initial entry, widen the opening into the thenar space using blunt dissection. Insert a finger (gloved, of course) or a curved clamp to explore the entire cavity. This is crucial for breaking down any loculations, which are common in deep space infections and can harbor pockets of pus. Ensure complete evacuation of all purulent material.
This image may show blunt dissection within the space. Debride any obviously necrotic tissue, but exercise extreme caution to avoid damaging underlying tendons or neurovascular structures. The wound should be thoroughly irrigated with copious amounts of sterile saline solution to remove debris and reduce the bacterial load.
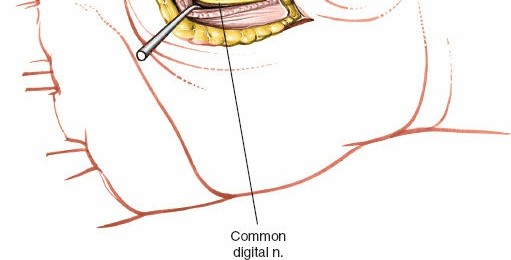
6. Managing Critical Nerves
Digital Nerves
The digital nerves to the index finger are directly in line with the initial skin incision. Continuous vigilance is required to ensure these delicate structures are not damaged during the incision of the palmar aponeurosis or during subsequent deeper dissection. Gentle retraction, not excessive tension, is key to their preservation.
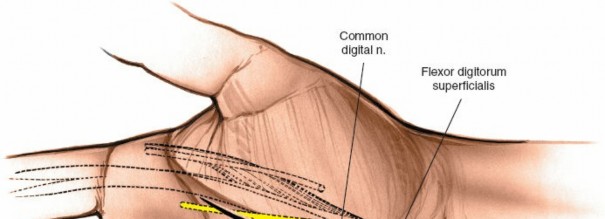
Motor Branch to the Thenar Muscles
The motor branch to the thenar muscles (recurrent motor branch of the median nerve) emerges from the deep surface of the median nerve as the median nerve leaves the carpal tunnel. Note, however, that the location of its division from the median nerve is quite variable. This nerve typically hooks around the distal end of the flexor retinaculum to supply the thenar muscles.
This illustration (potentially analogous to Fig. 5-39 from the original seed) highlights the variable course of the recurrent motor branch. It is imperative to make sure to identify this branch at the proximal end of the incision or just deep to the thenar crease so as to avoid damaging it during the entry into the thenar space or during subsequent deep exploration. Careful, layered dissection in this area is paramount.
7. Drain Placement and Wound Management
After complete drainage and irrigation, a passive drain (e.g., Penrose drain or corrugated drain) is typically placed into the deepest extent of the thenar space and brought out through a separate stab incision or through a portion of the main incision. The drain helps to maintain patency of the drainage tract and prevent premature wound closure, allowing for continued egress of exudate. Secure the drain with a single non-absorbable suture.
The primary incision is generally left open or partially closed loosely, depending on the extent of contamination and the surgeon's preference. Packing the wound gently with sterile gauze (e.g., iodoform gauze or plain saline-soaked gauze) facilitates ongoing drainage and prevents skin bridging. The hand is then dressed with a bulky, sterile soft dressing.
Complications & Management
Despite meticulous surgical technique, complications can arise following thenar space drainage, often due to the severity of the initial infection, anatomical complexity, or post-operative factors. Vigilant monitoring and timely intervention are crucial for salvage.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.)* | Salvage Strategy |
|---|---|---|
| Incomplete Drainage / Recurrence | 5-15% (varies with initial severity and technique) | Re-exploration, repeat drainage with meticulous breaking of loculations, aggressive debridement, consideration of wider incision or alternative approach. Optimize antibiotic regimen based on cultures. |
| Digital Nerve Injury (Index Finger) | 2-5% (higher with inexperienced surgeons or difficult anatomy) | Primary repair if recognized intraoperatively and feasible. Otherwise, secondary nerve repair, nerve grafting, or neurolysis for painful neuromas. Functional implications vary based on nerve involved (sensory loss). |
| Recurrent Motor Branch Injury | 1-3% (highly variable due to anatomical variability) | Primary repair if recognized and repairable. Delayed repair (up to 3-6 months) if incomplete recovery. Tendon transfers (e.g., FDS to APB, EIP to APB) for established deficits and thenar atrophy to restore thumb opposition. |
| Vascular Injury | <1% (usually minor vessels, rarely major) | Direct pressure, ligation of minor bleeders. For major vessel injury (e.g., superficial palmar arch branch), primary repair if feasible by microvascular surgeon, or ligation if collateral flow is sufficient (risk of digital ischemia). |
| Post-Operative Stiffness/Contracture | 10-25% (related to severity of infection, prolonged immobilization, scarring) | Aggressive hand therapy, early active and passive range of motion exercises (once acute infection resolves). Serial splinting, dynamic splinting. Surgical release of contractures, tenolysis, or capsulectomy in recalcitrant cases. |
| Spread of Infection | 1-5% (to midpalmar space, Parona's space, osteomyelitis) | Prompt identification via clinical signs, imaging (MRI). Immediate surgical drainage of newly involved spaces, more aggressive antibiotic therapy. Debridement of osteomyelitic bone if present. |
| Persistent Pain/Neuroma Formation | 5-10% | Analgesia, physical therapy. Neuroma excision with nerve capping or implantation into muscle/bone for symptomatic neuromas. Targeted nerve blocks. |
| Antibiotic-Related Complications | Variable (allergy, C. diff colitis, renal/hepatic toxicity) | Monitor drug levels (if applicable), adjust dosage, switch antibiotics based on sensitivities and side effect profile. Support for organ dysfunction. |
| Wound Dehiscence/Infection | 5-10% (often due to persistent infection or premature closure) | Daily wound care, open packing, local wound care dressings. If dehiscence with purulence, re-explore for residual infection. Delayed primary closure or secondary intention healing. |
* Incidence rates are approximate and vary widely based on patient population, infection etiology, surgical technique, and reporting standards.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical drainage itself for optimizing functional outcomes and minimizing long-term disability. A multidisciplinary approach involving the surgeon, hand therapist, and patient is essential.
Phase 1: Acute Inflammatory Control and Wound Care (Days 1-7)
- Elevation: Maintain continuous hand elevation above heart level (e.g., on pillows or in a sling) to reduce swelling, pain, and throbbing.
-
Wound Care:
- Dressings are changed daily or every other day, depending on the volume of exudate.
- The drain, if placed, is managed according to protocol (e.g., removal when drainage significantly decreases, typically within 24-72 hours).
- Wound irrigation with saline during dressing changes.
- Observe for signs of persistent infection (increasing pain, swelling, erythema, purulent discharge, fever).
- Antibiotics: Continue intravenous antibiotics, transitioning to oral antibiotics based on culture sensitivities and clinical improvement. The duration of antibiotic therapy (typically 10-14 days or longer for severe infections) is individualized.
- Pain Management: Administer appropriate analgesia to allow for comfortable participation in early therapy.
-
Early Motion:
- Gentle, pain-free active range of motion (AROM) exercises for the uninvolved joints (wrist, elbow, shoulder).
- Crucially, for the involved digits and thumb, very gentle, short-arc active flexion and extension are initiated as soon as acute pain and swelling subside, and wound stability allows. This is vital to prevent stiffness and adhesions, particularly around the FPL tendon sheath. Passive range of motion is generally avoided in the very early phase to prevent further trauma to inflamed tissues.
- Splinting: A protective, non-constrictive static splint may be used initially for comfort and protection, especially if the thumb is very painful, but should allow for judicious early motion.
Phase 2: Restoring Range of Motion and Strength (Weeks 1-6)
-
Progressive Range of Motion:
- Gradually increase the intensity and duration of AROM exercises for the thumb and fingers, focusing on full flexion and extension.
- Initiate gentle passive range of motion (PROM) for specific joints if AROM is limited, guided by the hand therapist.
- Tendon gliding exercises to prevent adhesion formation around the FPL tendon.
- Scar Management: Begin scar massage once the wound is epithelialized and sutures are removed (if applicable) to soften the scar and prevent contracture. Silicone gel sheeting or compression garments may be considered.
- Strengthening: Once a good range of motion is achieved without pain or signs of persistent infection, light isometric strengthening exercises can be introduced. Progress to resistance exercises with therapy putty or resistance bands.
- Edema Control: Continue elevation, retrograde massage, and compression techniques as needed.
Phase 3: Functional Restoration and Return to Activity (Weeks 6-12+)
- Advanced Strengthening: Progress to more functional grip and pinch strengthening exercises.
- Fine Motor Skills: Work on dexterity and coordination activities relevant to the patient's daily activities and occupation.
- Activity Modification: Guidance on modifying activities to prevent re-injury or excessive stress on the healing tissues.
- Return to Work/Sport: Gradual return to work or sports activities, emphasizing proper body mechanics and protective measures.
- Psychological Support: Address any fear-avoidance behaviors or psychological distress related to the injury and recovery.
Throughout all phases, close communication between the surgeon and hand therapist is paramount to adjust the protocol based on individual patient progress and complications. Long-term follow-up is necessary to monitor for potential issues such as chronic pain, stiffness, or delayed nerve recovery.
Summary of Key Literature / Guidelines
Deep space infections of the hand, including those involving the lateral (thenar) space, are well-recognized entities in orthopedic and hand surgery literature. The fundamental principles of management have remained consistent over decades, emphasizing early diagnosis and aggressive surgical drainage.
Classic texts by authors such as Kanavel laid the groundwork for understanding the fascial spaces of the hand and the patterns of infection spread. While modern imaging modalities (ultrasound, MRI) have significantly improved diagnostic accuracy, the core surgical tenets of incision, complete debridement, and drainage remain paramount.
Key Principles from Literature and Guidelines:
- Early Recognition and Diagnosis: Prompt clinical suspicion, supported by appropriate imaging (especially ultrasound for abscess confirmation), is critical. Delay in diagnosis directly correlates with worse outcomes and increased morbidity.
- Aggressive Surgical Drainage: Surgical incision and drainage are the definitive treatment for established abscesses. The literature consistently highlights the importance of thorough exploration to break down all loculations and ensure complete evacuation of purulent material. Inadequate drainage is a leading cause of recurrence and persistent infection.
- Anatomical Precision: A detailed understanding of the complex anatomy of the hand, particularly the fascial planes and vital neurovascular structures, is essential to perform safe and effective drainage. The risk of iatrogenic nerve or vessel injury during thenar space drainage is significant and must be mitigated by meticulous technique, as described in anatomical studies and surgical atlases.
- Targeted Antibiotic Therapy: Empiric broad-spectrum antibiotics should be initiated immediately and subsequently tailored based on intraoperative Gram stain results and definitive culture and sensitivity reports. The duration of antibiotic therapy is individualized but typically extended to 10-14 days or longer for severe cases.
- Post-Operative Rehabilitation: The importance of early, controlled mobilization and comprehensive hand therapy to prevent stiffness, adhesions, and optimize functional recovery is emphasized in numerous studies and professional guidelines (e.g., those from the American Society for Surgery of the Hand, ASSH). Prolonged immobilization is a known contributor to poor outcomes.
- Prevention of Recurrence: Strategies include complete drainage, appropriate antibiotic use, removal of foreign bodies if present, and patient education on wound care and adherence to antibiotic regimens.
While comprehensive, large-scale randomized controlled trials specifically on thenar space drainage are scarce due to the relatively low incidence and ethical considerations, the consensus for management is derived from extensive clinical experience, retrospective series, and expert opinion. Current guidelines advocate for a protocolized approach, combining prompt diagnosis, meticulous surgical technique, appropriate antimicrobial therapy, and structured post-operative rehabilitation for optimal patient outcomes in thenar space infections. Future research may focus on optimizing non-invasive diagnostic tools, novel antimicrobial strategies, and refining rehabilitation protocols.
Clinical & Radiographic Imaging