Introduction to Scapholunate Instability and Carpal Kinematics
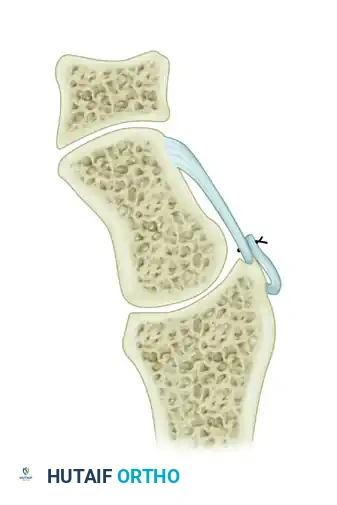
Scapholunate (SL) dissociation is the most common and clinically significant form of carpal instability. Disruption of the scapholunate interosseous ligament complex destabilizes the proximal carpal row, leading to a predictable pattern of kinematic failure. Without the tethering effect of the intact SL ligament, the scaphoid assumes an abnormally palmar-flexed and pronated posture, while the lunate extends, resulting in a Dorsal Intercalated Segmental Instability (DISI) deformity.
If left untreated, the altered contact mechanics between the scaphoid and the radial styloid inevitably progress to Scapholunate Advanced Collapse (SLAC), characterized by progressive radiocarpal and midcarpal arthrosis. To halt this degenerative cascade, surgical interventions such as dorsal capsulodesis and limited wrist arthrodesis (triscaphe fusion) have been developed. These procedures aim to restore the scaphoid to its anatomic alignment, thereby normalizing carpal kinematics and preserving joint longevity.
💡 Clinical Pearl: The Biomechanical Goal
The primary objective of dorsal capsulodesis is not to reconstruct the anatomic scapholunate ligament, but rather to create a robust dorsal tether that prevents the scaphoid from rotating into abnormal palmar flexion. This effectively neutralizes the deforming forces that drive DISI progression.
Dorsal Capsulodesis: The Blatt Procedure
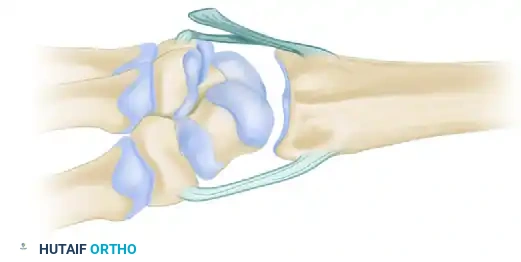
Originally described by Blatt, dorsal capsulodesis utilizes a proximally based flap of the dorsal wrist capsule to tether the distal pole of the scaphoid to the dorsal rim of the distal radius.
Preoperative Evaluation and Indications
Thorough radiographic evaluation is mandatory before proceeding with a dorsal capsulodesis. Standard posteroanterior (PA), lateral, and dynamic (clenched fist, ulnar deviation) views must be scrutinized to determine the extent of SL dissociation and rotary subluxation of the scaphoid.
⚠️ Surgical Warning: The Blatt Criterion
Blatt established a strict, singular criterion for this procedure: The surgeon must be able to anatomically reduce the scaphoid at the time of surgery. If the scaphoid is fixed in a flexed position due to secondary capsular contractures or early arthritic changes, a soft-tissue capsulodesis will fail, and a salvage procedure (e.g., proximal row carpectomy or limited arthrodesis) is indicated.
Step-by-Step Surgical Technique (Blatt)
1. Patient Positioning and Approach
* Ensure satisfactory regional or general anesthesia.
* Prepare and drape the upper extremity in a standard sterile fashion.
* Inflate a well-padded upper arm tourniquet to 250 mm Hg.
* Make a longitudinal dorsoradial incision centered over Lister's tubercle, extending distally toward the base of the third metacarpal.
2. Exposure and Retraction
* Identify and protect the sensory branches of the superficial radial nerve.
* Open the third dorsal extensor compartment and transpose the extensor pollicis longus (EPL) tendon radially.
* Elevate the fourth dorsal compartment subperiosteally and retract the wrist and finger extensors laterally (wrist extensors) and medially (finger extensors).
3. Capsular Flap Creation
* Make a longitudinal incision through the dorsal capsule near the longitudinal axis of the scaphoid to expose its full length.
* Preserve a 1-cm wide flap of the dorsal wrist capsule. Develop this flap from the ulnar side of the capsular incision.
* Release the flap distally, leaving its proximal origin firmly attached to the dorsum of the distal radius.
4. Joint Inspection and Scaphoid Reduction
* Inspect the interosseous and dorsal scapholunate ligaments to confirm their rupture and assess irreparability.
* Reduce the scaphoid by applying firm thumb pressure on the scaphoid tubercle from the palmar aspect.
* Simultaneously bring the wrist into slight ulnar deviation to assist in correcting the scaphoid's flexed posture.
5. Kirschner Wire Fixation
* Once anatomic reduction is achieved, transfix the scaphoid using 0.045-inch (1.16-mm) Kirschner wires.
* Drive the wires from the distal pole of the scaphoid into the capitate and the base of the third metacarpal to hold the reduction rigidly.
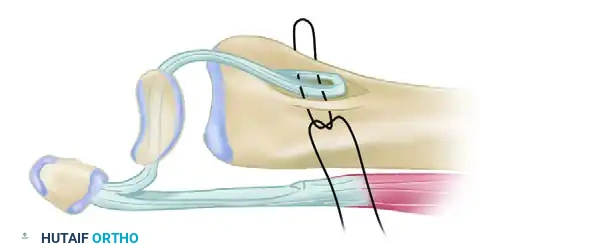
6. Scaphoid Preparation and Flap Insertion
* Using a narrow osteotome or a small rongeur, create a notch in the dorsal cortex of the distal pole of the scaphoid. This notch must be proximal to the distal articular surface and distal to the midaxis of rotation of the scaphoid.
- Trim the proximally based dorsal capsuloligamentous flap to the appropriate length.
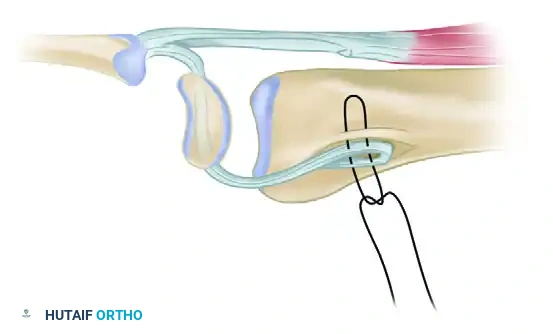
- Secure the flap into the prepared scaphoid notch using a 4-0 stainless steel pull-out wire suture.
- Pass the wire suture through fine drill holes directed toward the volar tubercle of the scaphoid.
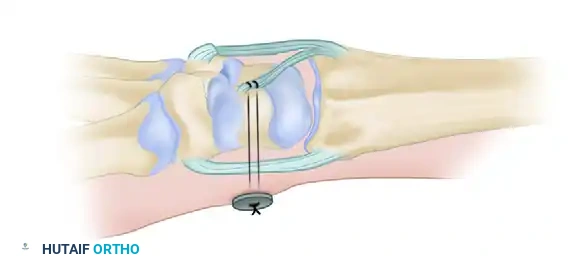
- Tie the pull-out wire at the level of the palmar skin over a felt pad and a button to secure the tenodesis effect.
7. Closure
* Deflate the tourniquet, obtain meticulous hemostasis, and close the skin in layers. Apply a sterile dressing and a thumb spica splint.
The Berger Modification: Dorsal Intercarpal (DIC) Ligament Capsulodesis
Recognizing the biomechanical importance of the intrinsic dorsal ligaments, Berger described a highly effective modification of the dorsal capsulodesis that utilizes the Dorsal Intercarpal (DIC) ligament rather than a non-specific capsular flap.
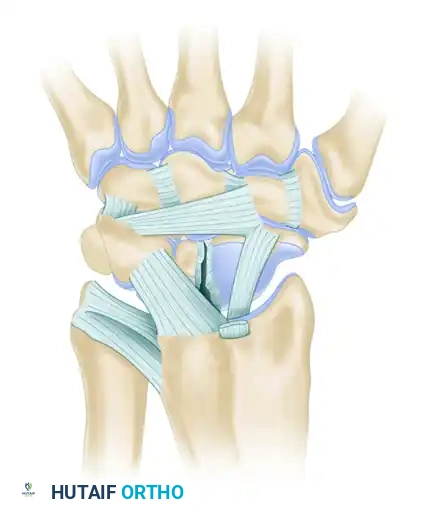
Surgical Technique (Berger Modification)
Instead of raising a standard capsular flap, the surgeon identifies the robust dorsal intercarpal ligament, which courses transversely across the proximal carpal row.
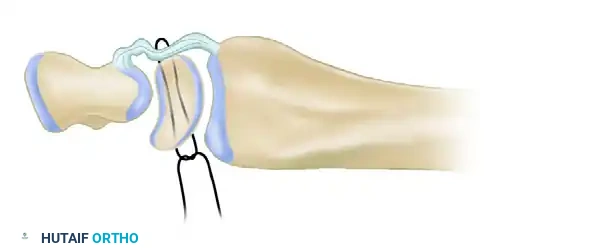
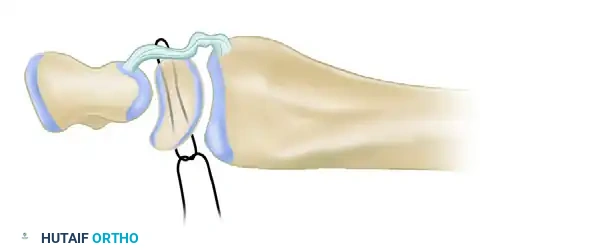
- Ligament Detachment: Incise down the length of the DIC ligament to detach its proximal half.
- Preservation of Scaphoid Insertion: Leave the lateral insertion of the ligament firmly attached to the distal scaphoid.
- Triquetral Release: Detach the medial (triquetral) end of the ligament, creating a robust, scaphoid-based ligamentous sling.
- Derotation and Fixation: Reduce the scaphoid into an extended, anatomic position. Suture the free, triquetral end of the DIC ligament to the dorsal rim of the distal radius. This attachment can be made directly to bone using suture anchors or sutured to the stout origin of the dorsal radiocarpal ligament.
💡 Biomechanical Advantage of the Berger Technique
By utilizing the DIC ligament, the Berger modification provides a stronger, more anatomically aligned vector of pull to resist scaphoid flexion compared to the traditional Blatt capsular flap. It directly counteracts the rotary subluxation forces while minimizing the loss of physiologic wrist flexion.
Postoperative Care for Dorsal Capsulodesis
Strict adherence to postoperative protocols is critical to prevent stretching of the capsulodesis before biologic healing occurs.
* 0 to 14 Days: The patient is immobilized in a rigid thumb spica cast. At 10 to 14 days, the cast is removed, skin sutures are extracted, and a new, well-molded thumb spica cast is applied.
* 2 to 8 Weeks: The secondary cast remains in place for an additional 6 weeks (totaling 8 weeks of continuous immobilization).
* 8 Weeks Post-op: The cast is removed. The pull-out wire (if the Blatt technique was used) and the transfixing K-wires are removed in the clinic.
* Rehabilitation: Gentle, active range-of-motion (ROM) exercises are initiated. Passive stretching and forceful gripping are strictly prohibited until at least 12 weeks postoperatively.
Limited Wrist Arthrodesis: Triscaphe (STT) Fusion
When soft-tissue capsulodesis is insufficient—either due to chronicity, fixed deformity, or early degenerative changes—limited wrist arthrodesis becomes the procedure of choice. Since the 1950s, various limited fusions have been employed for rotary subluxation of the scaphoid.
Historical Context and Biomechanical Rationale
In 1967, Peterson and Lipscomb described the successful fusion of the scaphoid, trapezium, and trapezoid (the triscaphe or STT joint). Later, Watson and Hempton popularized the triscaphe arthrodesis, demonstrating its profound effectiveness in resisting the massive forces of carpal movement.
By fusing the scaphoid to the distal carpal row (trapezium and trapezoid), the scaphoid is locked in a perpendicular position relative to the forearm. This permanently prevents the scaphoid from rotating into palmar flexion, thereby stabilizing the entire proximal carpal row and correcting the DISI deformity.
Kleinman’s extensive review of STT fusions confirmed that while carpal mechanics are permanently altered (due to the loss of the normal carpal shift relationship between the scaphoid and lunate), patients typically preserve 70 to 75 percent of their normal dorsiflexion-palmar flexion arc.
⚠️ Pitfalls in STT Arthrodesis
Kleinman noted that in a review of 41 cases, 11 patients experienced major surgical complications. Retrospective analysis revealed that the development of postoperative arthrosis was directly related to imperfect reduction of the scaphoid prior to fusion. The scaphoid must be anatomically extended before the arthrodesis is secured; fusing the scaphoid in a flexed position will lead to catastrophic radiocarpal impingement and rapid joint destruction.
Indications for Triscaphe Arthrodesis
Watson initially outlined three primary indications for STT arthrodesis, which were later expanded to include complex instability patterns:
1. Degenerative Arthritis: Isolated osteoarthritis of the scaphotrapezial-trapezoid joint (provided the thumb carpometacarpal joint is normal).
2. Radial Hand Dislocations: Complex carpal fracture-dislocations requiring stabilization of the radial column.
3. Rotary Subluxation of the Scaphoid: Chronic SL dissociation where primary ligament repair is impossible.
4. DISI Deformity: Static rotary instability caused by the disruption of volar ligaments tethering the lunate.
5. Resistant Scaphoid Nonunions: Combined with structural bone grafting to stabilize the nonunion site mechanically.
Kleinman further refined the clinical and radiographic criteria for STT fusion:
* Clinical Criteria: Pain at the end arcs of motion (especially in radial deviation); grip weakness caused by proximal row instability; and loss of motion secondary to pain.
* Radiographic Criteria:
* Scapholunate diastasis greater than 2 mm (the "Terry Thomas" sign).
* A scaphoid angle greater than 60 degrees on a true lateral radiograph.
* Foreshortening of the scaphoid on the AP view (the distance from the inferior margin of the distal pole to the proximal pole at the radioscaphoid joint measures less than 7 mm).
Contraindications for Triscaphe Arthrodesis
STT arthrodesis is strictly contraindicated in the presence of radioscaphoid arthritis. If degenerative changes have already progressed to the radioscaphoid articulation (early-phase SLAC wrist), locking the scaphoid will only exacerbate the pain and accelerate the arthrosis. In such cases, a Proximal Row Carpectomy (PRC) or a Scaphoid Excision and Four-Corner Fusion is the appropriate salvage procedure.
Surgical Principles and Postoperative Care
The surgical execution of an STT fusion requires meticulous decortication of the articular surfaces between the scaphoid, trapezium, and trapezoid down to bleeding subchondral bone. Cancellous bone graft, typically harvested from the distal radius (Lister's tubercle), is packed tightly into the interstices. The reduction is held with multiple divergent K-wires or headless compression screws.
Postoperative Protocol for STT Arthrodesis:
* If K-wires are used, they are left in place and cut beneath the skin.
* The wrist is immobilized in a cast or rigid removable splint.
* Progressive range-of-motion exercises for the digits are started immediately to prevent tendon adhesions.
* The K-wires are typically removed at 3 months postoperatively, once radiographic union is confirmed.
* Following wire removal, wrist ROM progresses gradually. Forceful stress activities and heavy lifting are strictly prohibited for approximately 4 months to ensure complete bony consolidation and remodeling of the arthrodesis mass.
