INTRODUCTION TO THE LATERAL ARM FLAP
The lateral arm flap is a highly versatile, reliable, and anatomically consistent septocutaneous flap utilized extensively in reconstructive microsurgery. First described by Song et al. in 1982, it has become a workhorse for the coverage of small to medium-sized soft tissue defects, particularly in the hand, upper extremity, and head-and-neck regions. Classified as a Type B fasciocutaneous flap according to the Cormack and Lamberty classification, its blood supply is derived from the septocutaneous perforators of the posterior radial collateral artery (PRCA).
As an internationally recognized standard in operative orthopaedics and plastic reconstructive surgery, mastering the lateral arm flap requires a profound understanding of the lateral arm's cross-sectional anatomy. The flap offers numerous advantages: it is relatively thin, can be harvested as a sensate flap by including the posterior cutaneous nerve of the forearm, and can be modified into a composite flap incorporating vascularized triceps tendon or a segment of the lateral humeral cortex. Furthermore, the dissection can be performed in the supine position, allowing for a simultaneous two-team approach during complex reconstructions.
SURGICAL ANATOMY AND BIOMECHANICS
A meticulous understanding of the vascular, neural, and musculofascial anatomy of the lateral arm is paramount to safely executing this dissection without causing iatrogenic injury to the radial nerve or compromising the flap's pedicle.
Vascular Anatomy
The primary arterial supply to the lateral arm flap is the posterior radial collateral artery (PRCA).
* Origin: The PRCA is the terminal continuation of the profunda brachii artery. The profunda brachii arises from the brachial artery, travels through the spiral groove of the humerus alongside the radial nerve, and bifurcates at the level of the lateral intermuscular septum into the anterior radial collateral artery (ARCA) and the PRCA.
* Course: The PRCA descends within the lateral intermuscular septum, lying between the brachialis and brachioradialis muscles anteriorly, and the triceps muscle posteriorly.
* Perforators: As it courses distally toward the lateral epicondyle, the PRCA gives off 4 to 5 septocutaneous perforators that travel through the deep fascia to supply the overlying skin paddle.
* Venous Drainage: Drainage is primarily provided by the paired venae comitantes accompanying the PRCA, which drain into the profunda brachii veins. The cephalic vein can also be included for superficial venous drainage if required, though the deep system is usually sufficient.
Neural Anatomy
- Radial Nerve: The radial nerve is the most critical structure at risk during this dissection. It travels with the profunda brachii artery in the spiral groove, pierces the lateral intermuscular septum from posterior to anterior (approximately 10 cm proximal to the lateral epicondyle), and courses distally between the brachialis and brachioradialis.
- Sensory Innervation: The flap can be made sensate. The posterior cutaneous nerve of the arm (PCNA) and the posterior cutaneous nerve of the forearm (PCNF) run in close proximity to the PRCA within the septum. The PCNF can be harvested with the flap and coapted to a recipient sensory nerve to restore protective sensation.
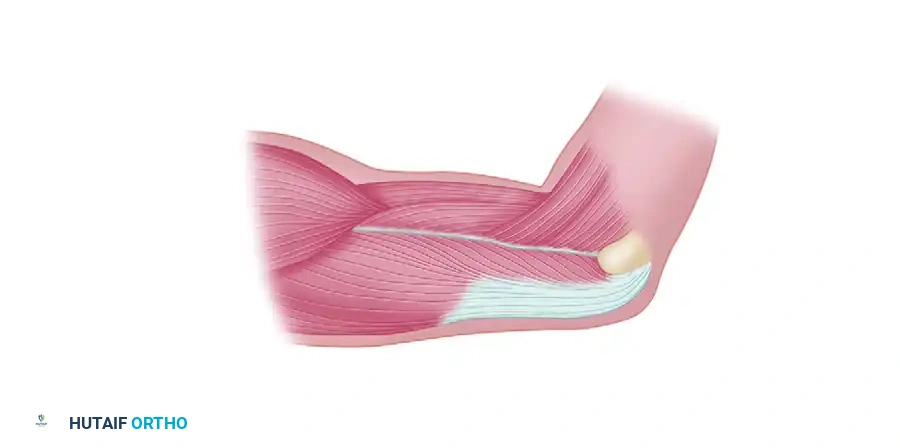
Musculofascial Anatomy
The flap is centered over the lateral intermuscular septum, a strong fascial band extending from the lateral humeral epicondyle to the insertion of the deltoid. The septum separates the anterior compartment (brachialis, brachioradialis) from the posterior compartment (triceps). The investing fascia of the triceps and the anterior compartment muscles must be included in the flap elevation to protect the delicate septocutaneous perforators.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Hand and Upper Extremity Reconstruction: Ideal for dorsal and palmar hand defects, web space contracture releases, and coverage of exposed tendons or joints due to its thin, pliable nature.
- Head and Neck Reconstruction: Used for intraoral lining, tongue reconstruction, and partial pharyngeal defects.
- Composite Tissue Defects:
- Osteocutaneous flap: Can include a sliver of the lateral humerus (up to 10 cm in length and 1 cm in depth) for reconstructing small bone gaps (e.g., metacarpals, mandible).
- Tendocutaneous flap: Can include a strip of the triceps tendon for simultaneous extensor mechanism reconstruction.
Contraindications
- Absolute: Previous severe trauma, burns, or surgical incisions over the lateral aspect of the donor arm that compromise the PRCA or its perforators.
- Relative: Obesity (which makes the flap excessively bulky), peripheral vascular disease affecting the upper extremity, or a requirement for a massive skin paddle (defects larger than 8-10 cm in width typically require skin grafting of the donor site, leading to poor aesthetic outcomes).
PREOPERATIVE PLANNING AND PATIENT POSITIONING
Preoperative Assessment
A thorough clinical examination of the donor arm is required. While routine angiography is rarely indicated, a handheld Doppler ultrasound is highly recommended to map the course of the PRCA and identify the dominant septocutaneous perforators along the axis of the lateral intermuscular septum.
Patient Positioning
- The patient is placed in the supine position.
- The donor arm is draped free to allow full mobility. It can be positioned on a radiolucent arm board or brought across the patient's chest, depending on the surgeon's preference and the location of the recipient site.
- A sterile tourniquet is applied high on the arm (near the axilla) to provide a bloodless surgical field during the initial dissection. The tourniquet is typically inflated after exsanguination with an Esmarch bandage, though some surgeons prefer to elevate the arm for 3 minutes without exsanguination to keep the perforators engorged and easily visible.
SURGICAL TECHNIQUE: STEP-BY-STEP DISSECTION
The dissection of the lateral arm flap requires meticulous technique to ensure the preservation of the septocutaneous perforators while safely separating the vascular pedicle from the radial nerve.
Step 1: Flap Design and Markings
The axis of the flap is defined by a line drawn from the insertion of the deltoid muscle to the lateral epicondyle of the humerus. This line corresponds to the lateral intermuscular septum.
- Dimensions: The flap is centered over this axis. For primary closure of the donor site, the maximum width of the flap should generally not exceed 6 cm, though this varies depending on the patient's skin laxity. The length can extend from the deltoid insertion down to the lateral epicondyle (typically 10-12 cm).
- Pinch Test: A pinch test is performed to confirm that the donor site can be closed primarily without excessive tension.
Step 2: Posterior Incision and Triceps Dissection
The dissection begins at the posterior margin of the designed skin paddle.
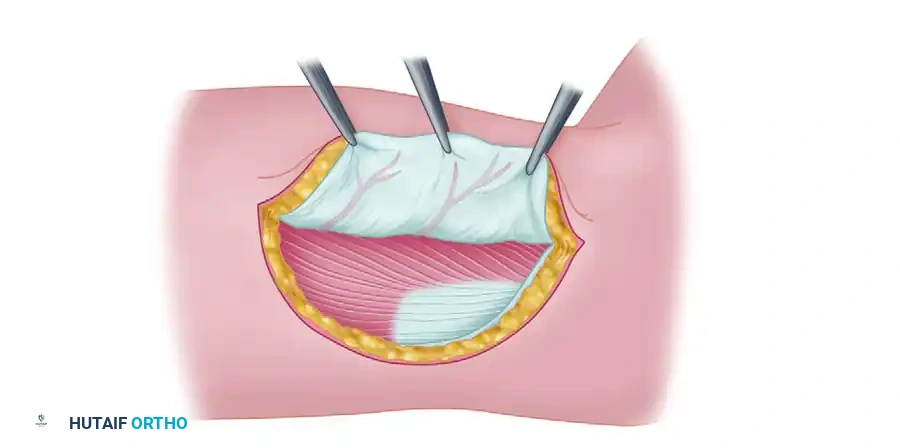
- Incision: The skin and subcutaneous tissues are incised along the posterior marking down to the deep investing fascia of the triceps muscle.
- Fascial Incision: The deep fascia is incised over the triceps muscle belly, ensuring that the fascia remains attached to the overlying skin and subcutaneous fat.
- Subfascial Elevation: The flap is elevated in a posterior-to-anterior direction in the subfascial plane. The dissection proceeds over the epimysium of the triceps until the lateral intermuscular septum is encountered.
- Perforator Identification: As the septum is approached, the cutaneous branches of the posterior radial collateral artery (PRCA) will be visualized traversing the septum to enter the deep fascia of the flap.
Surgical Warning: Do not separate the deep fascia from the subcutaneous tissue. The delicate septocutaneous perforators arborize within this fascial plexus. Shearing forces here will devascularize the flap.
Step 3: Anterior Incision and Pedicle Exposure
Once the posterior dissection reaches the septum and the perforators are confirmed, attention is turned to the anterior margin.
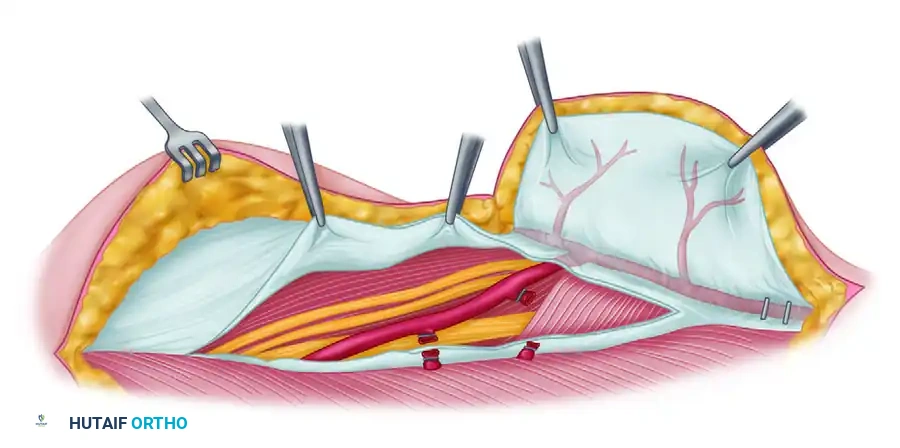
- Anterior Incision: The anterior margin of the flap is incised down through the deep fascia overlying the brachialis and brachioradialis muscles.
- Anterior Elevation: The flap is elevated in an anterior-to-posterior direction until the anterior aspect of the lateral intermuscular septum is reached.
- Identifying the Radial Nerve: At the proximal aspect of the incision, the space between the brachialis and brachioradialis is gently opened. The radial nerve must be identified as it pierces the lateral intermuscular septum and courses distally.
- Pedicle Isolation: Deep to the radial nerve, the profunda brachii artery and its bifurcation into the ARCA and PRCA are identified. The PRCA is seen entering the lateral intermuscular septum.
Clinical Pearl: The radial nerve is the key anatomical landmark in this dissection. It must be visually identified and protected with a vessel loop before any deep dissection or ligation of branches occurs within the septum.
Step 4: Flap Elevation and Pedicle Harvest
With both the anterior and posterior aspects of the septum exposed, the flap is ready to be isolated on its pedicle.
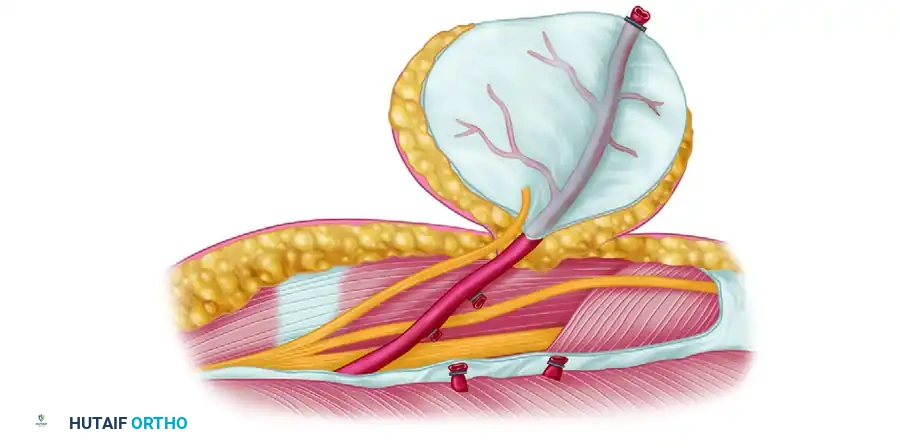
- Distal Release: The lateral intermuscular septum is divided at its distal extent, near the lateral epicondyle. The distal continuation of the PRCA is identified, ligated, and divided.
- Septal Elevation: The flap, now attached only by the lateral intermuscular septum and its vascular pedicle, is elevated from distal to proximal. The septum is carefully dissected off the lateral humerus. If an osteocutaneous flap is required, a cuff of the lateral humeral cortex is harvested en bloc with the septum using a sharp osteotome.
- Nerve Harvest: If a sensate flap is planned, the posterior cutaneous nerve of the forearm (PCNF) is identified within the septum, dissected proximally to obtain adequate length, and divided.
- Pedicle Dissection: The PRCA and its venae comitantes are dissected proximally toward the profunda brachii vessels. Small muscular branches to the triceps and brachialis are meticulously ligated with micro-clips or bipolar electrocautery. The radial nerve is gently retracted to allow the pedicle to be traced proximally into the spiral groove, maximizing pedicle length (typically 6-8 cm can be achieved).
- Flap Harvest: Once the recipient site is prepared, the tourniquet is deflated to confirm flap perfusion. After a period of reperfusion, the pedicle is ligated and divided, and the flap is transferred to the recipient site.
Step 5: Donor Site Closure
Meticulous closure of the donor site is essential to minimize morbidity and optimize aesthetic outcomes.
- Hemostasis: Absolute hemostasis is achieved using bipolar electrocautery.
- Drain Placement: A closed suction drain is placed deep into the wound bed to prevent hematoma formation, which could compress the radial nerve.
- Primary Closure: If the flap width was kept under 6 cm, the wound edges are widely undermined above the muscle fascia. The deep dermal layer is approximated with interrupted absorbable sutures (e.g., 3-0 Vicryl), and the skin is closed with a running subcuticular suture or surgical staples.
- Skin Grafting: If the defect cannot be closed primarily without excessive tension, a split-thickness skin graft is harvested from the thigh and applied to the muscle bed.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Flap Monitoring
- The transferred lateral arm flap is monitored strictly in a specialized microsurgical unit.
- Clinical assessment includes evaluating flap color, capillary refill time, and tissue turgor every hour for the first 24-48 hours.
- A handheld Doppler is used to assess the arterial signal over the marked perforator.
- Any signs of venous congestion (bluish discoloration, brisk capillary refill < 1 second) or arterial insufficiency (pallor, sluggish capillary refill > 3 seconds, loss of Doppler signal) warrant immediate surgical re-exploration.
Donor Site Management
- The donor arm is immobilized in a bulky, soft dressing with the elbow in slight flexion (30-45 degrees) to minimize tension on the closure line.
- The closed suction drain is typically removed when output is less than 15-20 cc over a 24-hour period (usually postoperative day 2 or 3).
- Mobilization: Gentle, active range of motion of the shoulder, elbow, and wrist is initiated early (postoperative day 3-5) to prevent stiffness. However, aggressive stretching of the lateral arm should be avoided for 3-4 weeks to allow the wound to heal securely.
- Complications: Patients should be counseled preoperatively regarding potential donor site morbidities, which include a widened or hypertrophic scar, lateral epicondylar pain, and a patch of numbness over the lateral proximal forearm (due to the sacrifice of the PCNF). Radial nerve palsy is a rare but severe complication that is entirely preventable with meticulous surgical technique and direct visualization during the dissection.
