DISPLACEMENT OF TENDONS
Tendon displacement—encompassing subluxation, dislocation, and traumatic avulsion—presents a unique biomechanical challenge in orthopedic surgery. When dynamic muscular stabilizers overpower their static retinacular or osseous restraints, the resulting instability leads to chronic pain, tendinopathy, and functional impairment. This masterclass details the pathophysiology, classification, and operative management of two distinct but highly relevant clinical entities: peroneal tendon displacement at the ankle and triceps tendon avulsion at the elbow.
PERONEAL TENDON DISPLACEMENT
Subluxation and dislocation of the peroneal tendons are uncommon, frequently misdiagnosed, and often overlooked causes of lateral ankle pain. Because the acute injury mechanism closely mimics a lateral ankle sprain—and frequently occurs concomitantly with lateral ankle ligamentous disruption—achieving an accurate initial diagnosis can be exceedingly difficult. Literature suggests that only 60% of peroneal tendon disorders are accurately diagnosed at the first clinical evaluation.
These injuries are most prevalent in young, high-demand athletic individuals participating in sports requiring rapid changes of direction, such as skiing, soccer, basketball, rugby, ice skating, tennis, football, and gymnastics. However, chronic subluxation has also been reported in the absence of any specific traumatic event, often secondary to underlying anatomical variations.
Anatomy and Biomechanics
The superior peroneal retinaculum (SPR) is the primary static restraint preventing lateral and anterior instability of the peroneal tendons at the fibular malleolus. Anatomically, the SPR extends approximately 3.5 cm proximally from the tip of the lateral malleolus, attaching posterolaterally onto the calcaneus and blending with the deep investing fascia adjacent to the Achilles tendon.
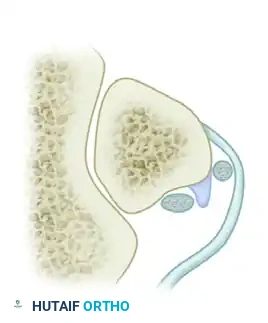
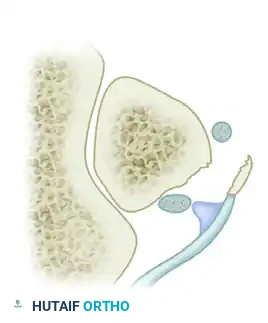
Displacement mechanics typically dictate that the peroneal tendons may subluxate within their tendon sheaths, but they are far more commonly displaced outside the sheaths and the retromalleolar tendon groove entirely. The pathophysiology involves the peroneal musculature contracting forcefully and overpowering the soft tissue restraints. Consequently, the tendons dislocate anteriorly from behind the distal fibula.
Clinical Pearl: The classic mechanism of injury involves a powerful, eccentric contraction of the peroneals with the foot in forced dorsiflexion and eversion. This dynamic overload causes catastrophic failure of the SPR, leading to subluxation or frank dislocation. Alternatively, a severe inversion injury with the foot in plantar flexion can stretch, attenuate, or avulse this critical structure.
Anatomical factors that predispose a patient to recurrent dislocation include:
* Incompetence or congenital laxity of the superior peroneal retinaculum.
* A shallow or absent retromalleolar sulcus.
* A convex posterior surface of the distal fibula.
* Congenital deformities, including congenital vertical talus and talipes planovalgus.
* Presence of an anomalous peroneus quartus muscle or a low-lying peroneus brevis muscle belly.
Classification of Peroneal Tendon Injuries
Peroneal tendon injuries are classified primarily by their anatomical location and the specific pattern of retinacular failure.
Shawen and Anderson Classification
This system categorizes injuries by anatomical zone:
* Zone I: Injuries involving the fibular groove, usually affecting the peroneus brevis tendon.
* Zone II: Injuries located in the cuboid tunnel, primarily involving the peroneus longus tendon.
Eckert and Davis Classification (Modified by Oden)
This is the most widely utilized surgical classification system, dividing SPR injuries into four distinct grades based on the pattern of retinacular avulsion from the fibula.
Grade 1 Lesion: The most common pattern (comprising >50% of cases). The superior peroneal retinaculum is elevated off the lateral malleolus, allowing the peroneal tendons to displace anteriorly and lie between the bone and the stripped periosteum.
Grade 2 Lesion: The fibrocartilaginous ridge located behind the lateral insertion of the SPR is avulsed along with the retinaculum. The tendons are displaced beneath this avulsed ridge.
Grade 3 Lesion: Involves a bony avulsion of a small cortical osseous fragment from the fibular insertion of the SPR. The tendons dislocate beneath the fibular bone fragment.
Grade 4 Lesion: The least common variant, characterized by a complete mid-substance avulsion or rupture of the superior peroneal retinaculum. The tendons lie external and superficial to the torn retinaculum.

Raikin Intrasheath Subluxation
More recently, Raikin et al. proposed a subgroup of peroneal subluxation termed intrasheath subluxation. This occurs within the peroneal groove beneath an otherwise intact superior peroneal retinaculum.
Normal Anatomy: The peroneus brevis lies anterior and deep, directly against the fibular groove, while the peroneus longus lies posterior and superficial.

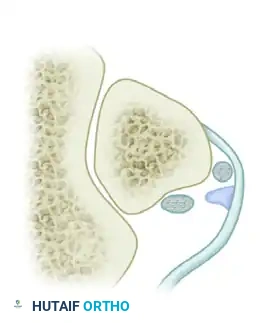
Type A Intrasheath Subluxation: There is no peroneal tendon tear. The tendons momentarily snap and switch their relative positions, with the peroneus longus tendon coming to lie deep to the peroneus brevis tendon.

Type B Intrasheath Subluxation: The peroneus longus subluxes anteriorly through a longitudinal split tear within the substance of the peroneus brevis tendon.

Clinical and Radiographic Evaluation
Diagnosis relies heavily on a high index of suspicion. Patients frequently report a painful "popping" or "clicking" sensation at the posterolateral ankle, particularly exacerbated when ascending stairs or pushing off on uneven ground.
Provocative Testing: The examiner places the patient's foot in active dorsiflexion, eversion, and external rotation while applying a resisting inversion–plantar flexion force. Dislocation or subluxation of the tendon can often be visually detected or palpated with circumduction of the foot while the examiner's fingers rest over the anterior tip of the peroneal groove. Note that patients with intrasheath subluxations (Raikin Types A and B) may not exhibit externally reproducible clinical signs.
Surgical Warning: Always differentiate peroneal tendon subluxation from a standard lateral ankle ligament sprain. While a sprain presents with tenderness distal and anterior to the lateral malleolus (ATFL footprint), peroneal subluxation presents with tenderness directly posterior and proximal to the tip of the fibula.
Differential Diagnosis of Lateral Ankle Pain (Box 48-6):
* Lateral ligament ankle sprain
* Achilles tendon rupture
* Fracture: lateral malleolus, fifth metatarsal base, cuboid
* Stress fracture: calcaneus or fibula
* Sinus tarsi syndrome
* Calcaneocuboid syndrome
* Peroneal tendinopathy or tenosynovitis
* Degenerative joint disease (subtalar or ankle)
* Tarsal coalition
* Osteochondral lesion of the talus (OLT)
* Loose bodies in the ankle or subtalar joint
* Sural neuritis
* L5/S1 Radiculopathy
* Accessory muscle (peroneus quartus) or symptomatic os peroneum
Imaging:
* Radiographs: Standard weight-bearing views are usually negative. However, in a Grade 3 Eckert and Davis injury, a cortical "fleck" sign (a small avulsion fracture) may be visible off the posterior distal fibula on the mortise or lateral view.
* MRI: The gold standard for identifying injury to the SPR, evaluating the integrity of the peroneal tendons (split tears), and identifying anomalous structures (low-lying brevis muscle belly). Kinematic (dynamic) MRI moving from dorsiflexion to plantar flexion is superior to static imaging, as the pathology is highly position-dependent.
* Ultrasonography: Highly effective, cost-efficient, and allows for real-time dynamic evaluation of peroneal tendon subluxation against the fibular groove.
Surgical Treatment
Treatment depends on the chronicity of the injury (acute vs. chronic), the underlying osseous and soft tissue anatomy, associated clinical findings, and the patient's activity level. Nonoperative treatment (cast immobilization) is rarely successful in athletes and carries a high recurrence rate. Operative intervention is the definitive standard of care.
Operative procedures fall into five general categories:
1. Periosteal Attachment / SPR Repair: Direct repair of the retinaculum to the fibula.
2. Groove Deepening: Excavation of the posterior fibula to create a deeper sulcus.
3. Tenoplasty: Tendon transfers or augmentations.
4. Bone Block Procedures: Fibular osteotomies to create a physical osseous barrier.
5. Rerouting Procedures: Transposing the tendons deep to the calcaneofibular ligament (CFL).
Preferred Technique: Soft Tissue Reconstruction with Groove Deepening
For the vast majority of chronic subluxations, a combination of SPR imbrication and fibular groove deepening yields the most reliable biomechanical outcomes.
Step-by-Step Approach:
1. Positioning: The patient is placed in the lateral decubitus position with a beanbag, or supine with a large ipsilateral hip bump to internally rotate the leg. A thigh tourniquet is applied.
2. Incision: A longitudinal posterolateral incision is made following the posterior border of the fibula, extending to the base of the fifth metatarsal.
3. Dissection: The sural nerve is carefully identified and protected. The SPR is incised longitudinally, leaving a small cuff on the fibula for later repair.
4. Tendon Inspection: The peroneus brevis and longus are inspected for longitudinal split tears. Any tears are debrided and tubularized using 4-0 non-absorbable suture.
5. Groove Deepening: The periosteum over the posterior fibula is elevated. A high-speed burr or a curette is used to deepen the retromalleolar groove. Alternative technique: A cortical window is hinged open, the underlying cancellous bone is impacted/tamped down, and the cortical flap is closed, preserving the smooth fibrocartilaginous gliding surface.
6. Retinacular Repair: The SPR is repaired tightly over the tendons using suture anchors placed into the posterolateral ridge of the fibula. A "pants-over-vest" imbrication technique ensures a robust, watertight restraint.
7. Closure and Post-op: The skin is closed in layers. The patient is placed in a non-weight-bearing short leg cast in slight plantar flexion and eversion for 4 weeks, followed by a CAM boot with progressive weight-bearing and physical therapy focusing on proprioception.
Note: Bone-block procedures (sliding fibular osteotomies) can provide excellent mechanical blocks but carry higher complication rates related to hardware prominence, nonunion, and altered joint kinematics.
TRICEPS TENDON AVULSION AND DISPLACEMENT
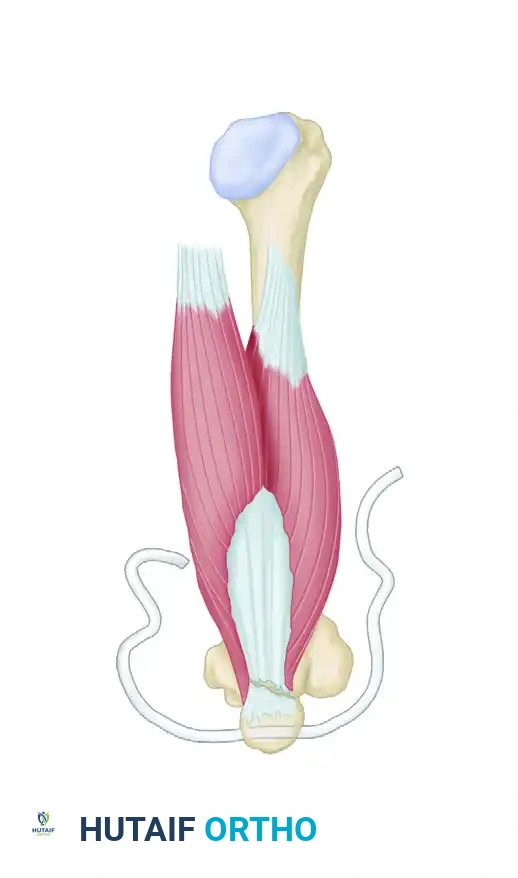
While peroneal instability dominates the lower extremity, displacement and avulsion of the triceps tendon represent a critical, albeit rare, upper extremity pathology. Triceps tendon ruptures typically occur at the osseous insertion on the olecranon following a sudden, eccentric deceleration force applied to an actively extending elbow.
Surgical repair is mandated for complete avulsions to restore elbow extension power. The goal is to achieve a rigid, anatomic fixation that permits early range of motion while utilizing remaining proximal and distal triceps tissue to augment the strength of the repair. Multiple procedures have been described for the treatment of chronic or acute ruptures, including the use of anconeus or Achilles rotation flaps, plantaris or hamstring tendon augmentation, and synthetic ligament augmentation devices.
Surgical Techniques for Triceps Repair
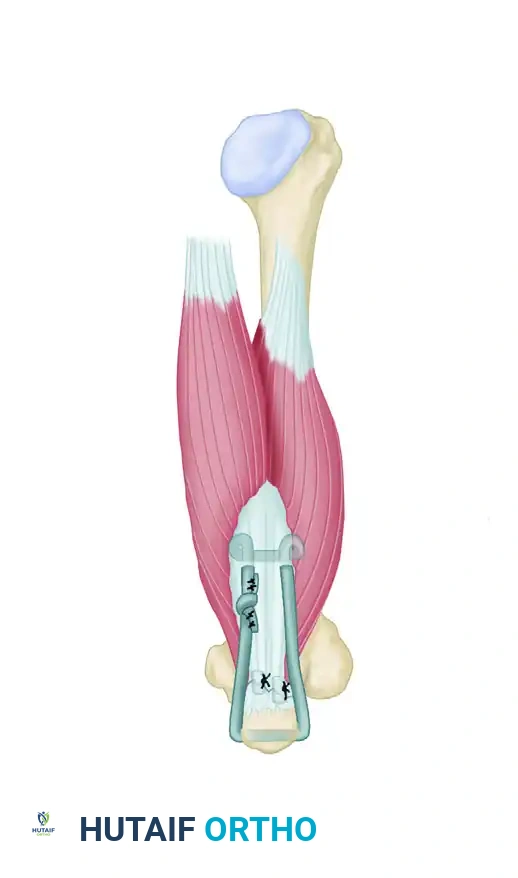
Transosseous Cruciate Repair (Mersilene Tape Technique)
For massive avulsions or revisions, a robust transosseous technique utilizing heavy non-absorbable tape (e.g., Mersilene) provides exceptional pull-out strength.
Step A: The avulsed triceps tendon is debrided to healthy tissue. The olecranon footprint is decorticated to a bleeding cancellous bed to promote healing. A transverse drill hole is created through the proximal ulna (olecranon). A heavy Mersilene strip is passed through the osseous tunnel.
Step B: The Mersilene strip is threaded through a large surgical needle. A locking loop is made through the medial aspect of the triceps tendon. The needle is then passed transversely through the tendon substance to the lateral side, where another locking loop is fashioned. The limbs are tensioned and tied securely with the elbow in 30 degrees of flexion, effectively docking the tendon into the decorticated footprint.
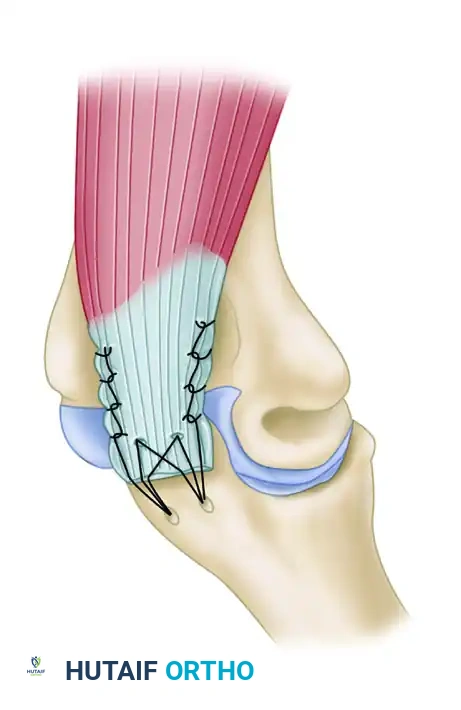
Anatomic Triceps Tendon Footprint Repair (Suture Anchor Technique)
Modern biomechanical studies advocate for an "anatomic footprint repair" utilizing double-row suture anchors. This technique maximizes the tendon-to-bone contact area, replicating the native broad insertion of the triceps.
In this technique, a proximal row of suture anchors is placed at the articular margin of the olecranon. The sutures are passed through the triceps tendon in a mattress fashion. The suture tails are then brought distally and secured with a second row of knotless anchors, creating a broad, pressurized footprint that resists displacement during early active rehabilitation.
Postoperative Protocol for Triceps Repair
Following rigid fixation, the elbow is immobilized in a posterior splint at 30 to 45 degrees of flexion for 2 weeks to protect the skin incision and the repair. At two weeks, the patient is transitioned to a hinged elbow brace. Passive and active-assisted range of motion is initiated, strictly avoiding active extension against resistance for the first 6 weeks. Progressive strengthening begins at 8 weeks, with a full return to heavy lifting or sports anticipated at 4 to 6 months postoperatively.
📚 Medical References
- [TECHNIQUE 46-33
• In the rare instance when no pathological condition exists in the rotator cuff, use an anterior approach through the deltopectoral interval. Identify the long head of the biceps tendon, and make an incision through the transverse humeral ligament, extending down through the proximal third of the pectoralis major tendon. Rarely, the biceps tendon can be placed back in the groove, and the transverse humeral ligament can be repaired using interrupted sutures. More commonly, tenodesis should be performed.
• If rotator cuff pathology is present with the subluxing biceps tendon, use an anterosuperior approach, beginning the incision just lateral to the](https://pubmed.ncbi.nlm.nih.gov/?term=TECHNIQUE%2046-33%0A%0A%E2%80%A2%20In%20the%20rare%20instance%20when%20no%20pathological%20condition%20exists%20in%20the%20rotator%20cuff%2C%20use%20an%20anterior%20approach%20through%20the%20deltopectoral%20interval.%20Identify%20the%20long%20head%20of%20the%20biceps%20tendon%2C%20and%20make%20an%20incision%20through%20the%20transverse%20humeral%20ligament%2C%20extending%20down%20through%20the%20proximal%20third%20of%20the%20pectoralis%20major%20tendon.%20Rarely%2C%20the%20biceps%20tendon%20can%20be%20placed%20back%20in%20the%20groove%2C%20and%20the%20transverse%20humeral%20ligament%20can%20be%20repaired%20using%20interrupted%20sutures.%20More%20commonly%2C%20tenodesis%20should%20be%20performed.%0A%0A%E2%80%A2%20If%20rotator%20cuff%20pathology%20is%20present%20with%20the%20subluxing%20biceps%20tendon%2C%20use%20an%20anterosuperior%20approach%2C%20beginning%20the%20incision%20just%20lateral%20to%20the)
