Disorders of the Patella: Diagnosis and Surgical Management
Key Takeaway
Disorders of the patella encompass a spectrum of pathologies including osteochondritis dissecans, dorsal defects, bipartite patella, and chondromalacia. Effective management requires a profound understanding of patellofemoral biomechanics and precise radiographic evaluation. This comprehensive guide details evidence-based diagnostic protocols, conservative management strategies, and advanced surgical techniques—such as the Ogata subperiosteal release—to optimize functional outcomes and restore extensor mechanism integrity in the orthopedic patient.
Comprehensive Introduction and Patho-Epidemiology
The Spectrum of Patellar Pathology
The patella, representing the largest sesamoid bone in the human body, is an indispensable biomechanical component of the extensor mechanism of the knee. By displacing the quadriceps tendon anteriorly away from the femorotibial axis, it significantly increases the moment arm of the extensor apparatus, thereby enhancing the mechanical advantage of the quadriceps muscle group by up to 30% to 50% throughout the arc of motion. However, this unique anatomical arrangement subjects the patellofemoral joint to immense compressive and shear forces, predisposing it to a distinct spectrum of developmental, osteochondral, and degenerative disorders. The orthopedic surgeon must possess a profound understanding of these pathologies, which range from incidental developmental variants to debilitating osteochondral defects, to prevent unwarranted interventions and optimize patient outcomes.
Pathophysiology of Osteochondritis Dissecans and Dorsal Defects
Osteochondritis dissecans (OCD) of the patella is a relatively rare entity compared to its counterpart in the femoral condyles, and it typically carries a more guarded prognosis due to the extreme shear forces experienced by the patellar facets. The condition is characterized by the focal separation of an osteochondral fragment from the underlying subchondral bone, secondary to localized ischemia, repetitive microtrauma, or a combination of both. OCD of the patella predominantly manifests in the second and third decades of life. Topographically, lesions are most frequently localized to the lower half of the patella, particularly along the median ridge and paramedial areas. Notably, bilateral involvement is observed in up to one-third of patients, necessitating a thorough evaluation of the contralateral knee even in unilateral presentations.
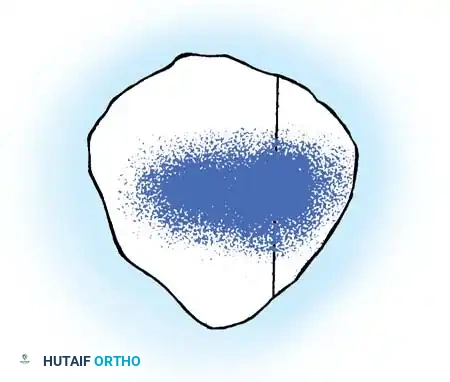
In stark contrast to OCD, a dorsal defect of the patella is a benign, circular, well-circumscribed radiolucent lesion, typically measuring approximately 1 cm in diameter. First described by Caffey, it invariably abuts the articular cartilage and is characteristically located in the superolateral quadrant of the patella. The exact etiology remains debated, though the prevailing consensus identifies it as a variant of normal ossification. Van Holsbeeck et al. proposed a traction injury hypothesis, noting a strong association between bipartite patella and dorsal defects. They postulated that repetitive traction at the insertion of the vastus lateralis muscle during the critical phases of patellar ossification leads to this localized defect. Misdiagnosis of a dorsal defect as an active OCD lesion can lead to unwarranted surgical intervention in a self-limiting condition.
Chondromalacia Patellae and Basal Degeneration
Introduced by Aleman in 1928, the term chondromalacia patellae specifically denotes the pathological softening, fibrillation, and degeneration of the articular cartilage of the patella. It is imperative to distinguish this strict pathological and arthroscopic diagnosis from the broader clinical syndrome of "anterior knee pain." The fundamental pathophysiology of chondromalacia differs drastically from primary osteoarthritis. While osteoarthritis initiates at the superficial articular surface with the loss of transverse collagen fibers, chondromalacia begins as basal degeneration—a disorder originating in the deep layers of the cartilage.
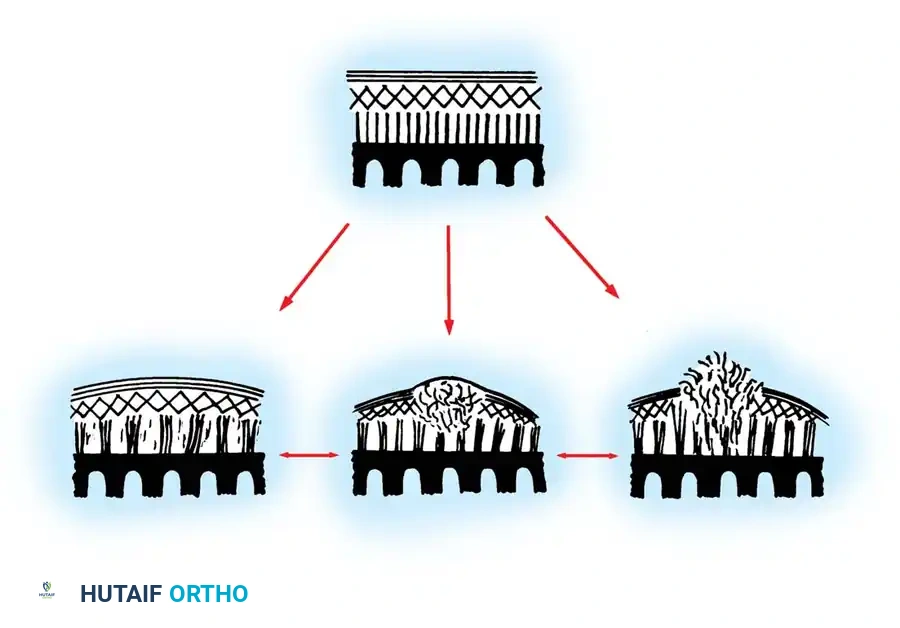
The initial lesion involves a biochemical degradation of the ground substance, specifically a marked decrease in sulfated mucopolysaccharides. Histologically, this is demonstrated by a loss of basophilia on hematoxylin and eosin (H&E) staining. During this early phase, the superficial articular surface remains macroscopically smooth and intact, though the cartilage feels softened or "boggy" to arthroscopic probing. Topographically, Goodfellow et al. mapped these lesions and found they predominantly occur in specific non-contact areas astride the median ridge and straddling the inferior portion of the central ridge. Extreme ranges of knee flexion bring these softened areas into direct articulation with the femoral trochlea, leading to macroscopic fibrillation, blistering, and eventual full-thickness cartilage loss.
Detailed Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
The patella is structurally designed to withstand high compressive loads, featuring the thickest articular cartilage in the human body, which can reach up to 6 to 7 millimeters in depth. The articular surface is divided by a prominent vertical median ridge into a larger lateral facet and a smaller medial facet. A secondary, less prominent vertical ridge further divides the medial facet to create the "odd facet" at the extreme medial border of the patella. The Wiberg classification system categorizes patellar morphology based on the relative sizes of these facets: Type I presents with symmetrical facets, Type II features a smaller medial facet, and Type III demonstrates a dysplastic, markedly hypoplastic medial facet with a dominant lateral facet. Type III morphology is highly associated with lateral patellar instability and abnormal tracking mechanics.
The Extensor Mechanism and Soft Tissue Constraints
The stability of the patellofemoral joint relies on a complex interplay of static and dynamic soft tissue constraints. The dynamic stabilizers comprise the quadriceps musculature, specifically the vastus medialis obliquus (VMO), which provides a dynamic medializing vector to counteract the lateral pull of the vastus lateralis. The static stabilizers are divided into medial and lateral retinacular complexes. The medial patellofemoral ligament (MPFL) is the primary restraint to lateral patellar translation, contributing 50% to 60% of the restraining force from 0 to 30 degrees of knee flexion. The lateral retinaculum, comprising the superficial oblique and deep transverse layers, provides a tethering effect that, when pathologically contracted, can lead to excessive lateral tilt and localized articular overload.
Patellofemoral Kinematics and Joint Reaction Forces
Patellofemoral kinematics are dictated by the engagement of the patella within the femoral trochlea. In full extension, the patella rests superior to the trochlear groove, relying entirely on soft tissue restraints for stability. As the knee flexes to 20-30 degrees, the patella engages the trochlea, shifting the primary stabilizing role to the osseous geometry. The joint reaction forces (JRF) across the patellofemoral articulation are profoundly influenced by the degree of knee flexion. During level walking, the JRF is approximately 0.5 times body weight. However, during stair climbing, this force increases to 3.3 times body weight, and during deep squatting, it can escalate to a staggering 7 to 8 times body weight. Any disruption in the kinematic chain—such as patella alta, excessive tibial tubercle-trochlear groove (TT-TG) distance, or trochlear dysplasia—exponentially amplifies these forces, precipitating premature chondral failure and the clinical manifestation of patellar disorders.
Exhaustive Indications and Contraindications
Surgical Decision Making in Patellar Disorders
The decision to proceed with surgical intervention for patellar disorders must be rigorously evidence-based, as inappropriate surgery can exacerbate patellofemoral pain and lead to iatrogenic instability. For osteochondritis dissecans, conservative management is indicated for stable lesions with intact articular cartilage, particularly in skeletally immature patients. Surgical intervention is strictly reserved for unstable lesions, detached fragments, or failure of prolonged conservative therapy (typically greater than 6 months). For bipartite patella, operative intervention is indicated only for refractory cases where localized pain persists despite activity modification, NSAIDs, and targeted physical therapy, or in the rare event of an acute, displaced traumatic separation of the synchondrosis.
Parameters for Extensor Mechanism Realignment
Extensor mechanism realignment, specifically tibial tubercle osteotomy (TTO), is indicated for patients with severe, symptomatic, full-thickness chondromalacia or localized patellofemoral osteoarthritis that has failed exhaustive conservative measures. Biomechanical offloading is indicated when the pathology is localized to the distal and lateral facets. A TT-TG distance exceeding 20 millimeters, as measured on axial computed tomography (CT) or magnetic resonance imaging (MRI), is a definitive indication for medialization of the tibial tubercle. Anteriorization (the Maquet or Fulkerson principle) is indicated to increase the moment arm and decrease overall patellofemoral contact stresses.
Contraindications to Patellar Surgery
Absolute contraindications to patellofemoral surgical intervention include active local or systemic infection, severe complex regional pain syndrome (CRPS), and the presence of asymptomatic incidental findings (such as an asymptomatic dorsal defect or bipartite patella). Relative contraindications include diffuse, unicompartmental, or bicompartmental tibiofemoral osteoarthritis, as isolated patellofemoral realignment will not address the primary source of global knee pain. Furthermore, a TTO is contraindicated in patients with profound medial facet chondromalacia, as medialization of the tubercle will paradoxically increase contact stresses on the already compromised medial articular surface.
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| OCD Fragment Fixation | Unstable but salvageable fragment; >15mm diameter; Failed conservative care | Active infection; Completely macerated/unsalvageable fragment | Skeletally immature with stable MRI findings |
| Bipartite Excision / Release | Refractory localized pain >6 months; Acute traumatic separation | Asymptomatic incidental finding; Generalized anterior knee pain | Poor quadriceps tone; Non-compliant patient |
| Tibial Tubercle Osteotomy (TTO) | TT-TG > 20mm; Distal/Lateral facet advanced chondromalacia | Diffuse tibiofemoral OA; Medial facet advanced chondromalacia | Active smoking; Poor soft tissue envelope |
| Autologous Chondrocyte Implantation (ACI) | Focal, full-thickness unipolar defect >2cm²; Intact subchondral bone | Kissing lesions; Uncorrected malalignment | Age > 50; BMI > 35 |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Radiographic Measurements
Thorough preoperative planning relies on a comprehensive imaging battery. Standard anteroposterior (AP) and lateral radiographs are mandatory, but the true lateral radiograph must be meticulously evaluated for patellar height using the Caton-Deschamps or Insall-Salvati ratios. The axial ("skyline") or Merchant view is the definitive projection to assess patellar tilt, subluxation, and the topographic location of osteochondral defects. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the integrity of the articular cartilage, assessing the stability of OCD fragments (indicated by high T2 signal fluid interposition behind the fragment), and identifying subchondral bone marrow edema associated with symptomatic bipartite patellae.
Surgical Templating for Osteotomies
When planning a tibial tubercle osteotomy, precise templating is critical to achieve the desired biomechanical vectors without compromising the structural integrity of the proximal tibia. Axial CT scans are utilized to calculate the TT-TG distance by superimposing the deepest point of the trochlear groove onto the center of the tibial tubercle. The degree of medialization is calculated to restore the TT-TG distance to a physiologic norm of 10 to 12 millimeters. For anteriorization (Fulkerson osteotomy), the slope of the osteotomy cut dictates the ratio of anteriorization to medialization. A steeper cut (e.g., 60 degrees to the coronal plane) provides more medialization with less anteriorization, whereas a shallower cut (e.g., 30 degrees) maximizes anteriorization to offload severe distal chondromalacia.
Operating Room Setup and Patient Positioning
The patient is positioned supine on a standard radiolucent operating table. A proximal thigh tourniquet is applied but typically inflated only if visualization is compromised, as tourniquet-induced quadriceps tethering can artificially alter patellofemoral tracking dynamics during intraoperative assessment. A lateral thigh post or a specialized leg holder is utilized to allow stable positioning at 90 degrees of flexion for arthroscopic evaluation, while permitting full extension for extensor mechanism realignment. The contralateral leg is secured in a well-padded gynecological stirrup or placed flat on the table to allow unhindered access for the C-arm fluoroscopy unit, which is draped and positioned on the non-operative side for orthogonal intraoperative imaging.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Assessment and Cartilage Restoration
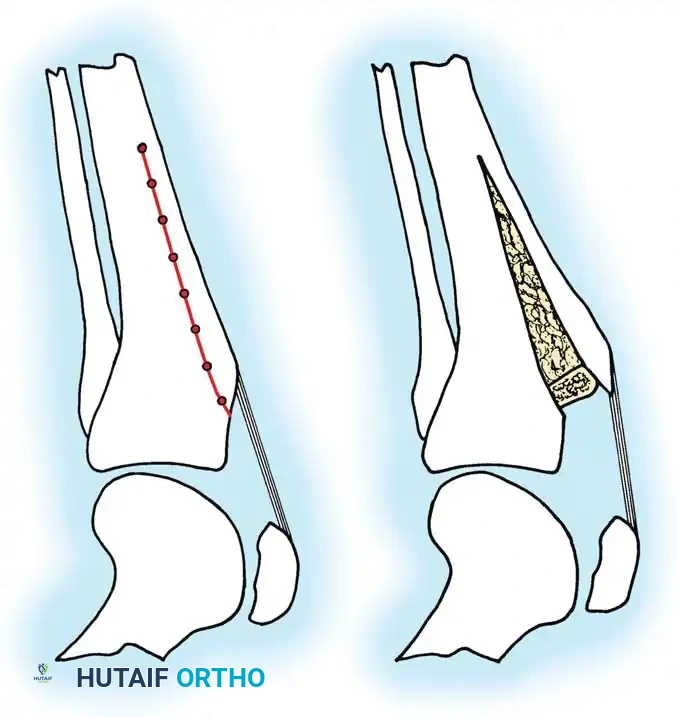
Every surgical intervention for patellar disorders should commence with a diagnostic arthroscopy to directly visualize the articular surfaces, assess patellar tracking dynamically, and address concomitant intra-articular pathology. The patellofemoral joint is evaluated from both standard anterolateral/anteromedial portals and superomedial/superolateral portals to ensure a comprehensive view of the facets. For unsalvageable OCD fragments, arthroscopic excision followed by curettage and marrow stimulation (microfracture or drilling) of the crater is performed. For salvageable fragments, the crater is debrided of fibrous tissue, the subchondral bone is prepared, and the fragment is reduced and stabilized using retrograde or antegrade bioabsorbable pins or Herbert screws, ensuring the hardware is countersunk below the articular surface.
The Ogata Subperiosteal Release for Bipartite Patella
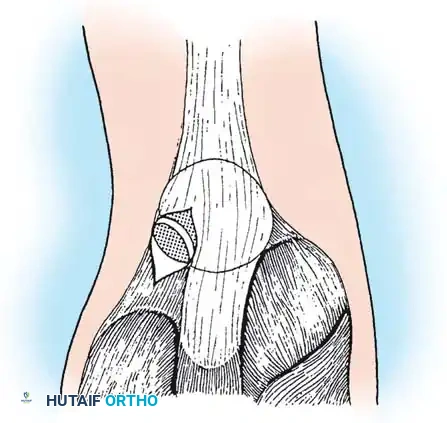
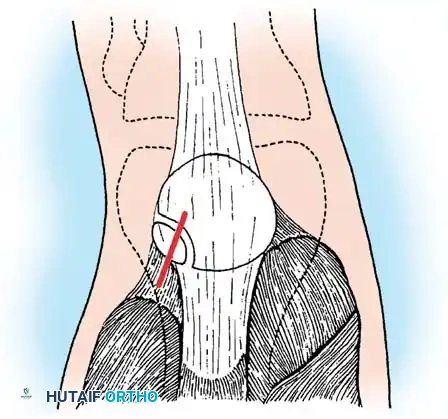
For symptomatic bipartite patella, particularly Saupe Type III lesions, the Ogata subperiosteal release of the lateral quadriceps mechanism is a highly effective, tissue-sparing technique. This procedure detaches the vastus lateralis insertion from the painful fragment while preserving the continuity of the tendon-periosteum complex to the main patella, relieving muscle traction without inducing a mediolateral tracking imbalance.
Following diagnostic arthroscopy, an oblique skin incision is made over the distal portion of the vastus lateralis tendon, extending just distal to the midportion of the separated bipartite area.
The vastus lateralis tendon, which is frequently hypertrophied in these patients, is identified. The tendon is split longitudinally along its middle fibers to expose the underlying bipartite fragment and synchondrosis.
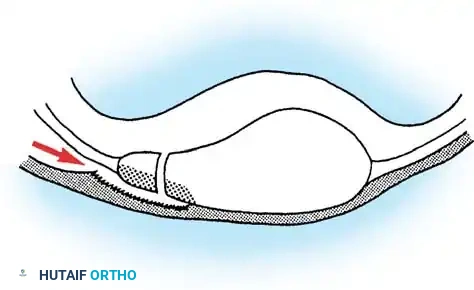
The tendinous insertion to the painful bipartite fragment is carefully detached in a subperiosteal plane. It is critical to preserve the continuity of the tendinous expansion to the main mass of the patella. The tendon-periosteum complex is dissected, and the smaller fragment is sharply denuded completely, relieving it from the traction forces of the vastus lateralis.
Stability of the denuded fragment is assessed by applying bending stress. If the synchondrosis widens significantly, the fragment is grossly unstable and excised. If it demonstrates minimal mobility, it is left in situ, as the traction relief will promote spontaneous union. The longitudinal split in the vastus lateralis is then repaired with absorbable sutures.
Tibial Tubercle Osteotomy (Fulkerson Procedure)
For advanced distal and lateral facet chondromalacia associated with malalignment, the Fulkerson anteromedialization (AMZ) osteotomy is performed. A longitudinal incision is made just lateral to the tibial crest. The anterior compartment musculature is elevated off the lateral tibia. Retractors are placed subperiosteally to protect the neurovascular bundle posteriorly.
Using an oscillating saw, an oblique osteotomy is created from medial to lateral, originating proximal to the patellar tendon insertion and exiting distally along the tibial crest. The angle of the cut is dictated by the preoperative templating (typically 45 to 60 degrees).
The osteotomized tubercle pedicle, with the patellar tendon securely attached, is mobilized and translated anteromedially along the osteotomy plane. The pedicle is temporarily provisioned with Kirschner wires, and patellar tracking is dynamically assessed through a full range of motion. Once optimal tracking and offloading are confirmed, the osteotomy is rigidly fixed using two or three 4.5mm fully threaded cortical lag screws placed from anterior to posterior, ensuring bicortical purchase.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
Surgical management of patellar disorders is fraught with potential complications that demand meticulous surgical technique to avoid. Intraoperative fracture of the tibial tubercle pedicle or propagation of the osteotomy into the proximal tibial articular surface is a catastrophic complication associated with TTO, occurring in 1% to 3% of cases. This is mitigated by ensuring the proximal cut is tapered smoothly and avoiding excessive levering of the bone fragment. Early postoperative complications include deep vein thrombosis (DVT), superficial wound infections, and arthrofibrosis. The patellofemoral joint is particularly susceptible to postoperative stiffness; therefore, prolonged immobilization must be strictly avoided unless dictated by fragile internal fixation.
Late Complications and Hardware Issues
Late complications frequently revolve around hardware irritation and failure of biological healing. Symptomatic hardware following TTO is common, with up to 30% to 40% of patients requiring elective screw removal once radiographic union is achieved, typically 6 to 12 months postoperatively. Nonunion or delayed union of the osteotomy site occurs in less than 2% of cases but requires aggressive intervention with bone grafting and revision fixation if symptomatic. In cartilage restoration procedures or OCD fixation, failure of fragment integration or progressive chondral delamination can occur, leading to recurrent mechanical symptoms and the need for revision debridement or autologous chondrocyte implantation (ACI).
Salvage Procedures and Arthroplasty
When joint-preserving procedures fail, or when patellofemoral osteoarthritis progresses to an end-stage, bone-on-bone state, salvage procedures are indicated. Historically, complete patellectomy was the procedure of choice; however, this drastically reduces the moment arm of the extensor mechanism, resulting in a 30% to 50% loss of quadriceps power and severe functional impairment. Today, patellectomy is universally considered an absolute last resort. Contemporary salvage involves patellofemoral arthroplasty (PFA) for isolated, strictly unicompartmental disease, or total knee arthroplasty (TKA) if there is concomitant tibiofemoral degeneration. PFA offers excellent pain relief and functional restoration, provided the extensor mechanism is properly aligned prior to or during the arthroplasty.
| Complication | Estimated Incidence | Prevention and Salvage Management Strategy |
|---|---|---|
| Symptomatic Hardware (TTO) | 30% - 40% | Countersink screw heads; Elective hardware removal after radiographic union (6-12 months). |
| Proximal Tibia Fracture | 1% - 3% | Taper proximal osteotomy cut; Avoid over-levering; Salvage with rigid plate fixation. |
| Arthrofibrosis | 5% - 10% | Early aggressive ROM protocols; Avoid prolonged extension casting; Arthroscopic lysis of adhesions. |
| Nonunion of Osteotomy | < 2% | Rigid bicortical lag screw fixation; Smoking cessation; Salvage with bone grafting and revision ORIF. |
| Recurrent Instability / Maltracking | 3% - 8% | Dynamic intraoperative assessment of tracking before final fixation; Revision realignment or MPFL reconstruction. |
Phased Post-Operative Rehabilitation Protocols
Phase I: Immediate Postoperative Protection and Tissue Healing
The initial postoperative phase (Weeks 0 to 2) prioritizes the protection of surgical fixation, mitigation of joint effusion, and re-establishment of basic quadriceps activation. For soft tissue procedures and arthroscopic debridements, weight-bearing is typically tolerated immediately. However, for osteotomies (TTO) and OCD internal fixation, patients are restricted to touch-down weight-bearing (TDWB) with the limb locked in full extension using a hinged knee brace. Cryotherapy and elevation are critical for edema control. Isometric quadriceps sets and straight leg raises (SLR) in the brace are initiated on postoperative day one to prevent profound VMO atrophy. Range of motion (ROM) is carefully introduced, typically limited to 0 to 30 degrees initially, to prevent excessive tension on the osteotomy or fixation site.
Phase II: Restoration of Kinematics and Strengthening
As biological healing progresses (Weeks 3 to 6), the focus shifts to restoring full, symmetric range of motion and progressive load-bearing. For TTO patients, weight-bearing is incrementally advanced to full weight-bearing by week 6, contingent upon radiographic evidence of early callus formation. The hinged brace is gradually unlocked to allow progressive flexion, targeting 90 degrees by week 4 and full flexion by week 6. Physical therapy emphasizes closed kinetic chain (CKC) exercises, such as mini-squats and leg presses within a pain-free arc, to stimulate VMO hypertrophy while minimizing patellofemoral joint reaction forces. Open kinetic chain (OKC) extension exercises are strictly avoided during this phase to prevent deleterious shear stresses on the healing articular cartilage.
Phase III: Advanced Functional Return and Maintenance
The final phase of rehabilitation (Weeks 7 to 16+) bridges the gap between basic functional recovery and return to high-demand athletic or occupational activities. Once full, painless ROM is achieved and radiographic union is definitively confirmed, advanced strengthening, proprioceptive training, and plyometrics are introduced. Eccentric quadriceps control is emphasized to ensure the extensor mechanism can adequately decelerate the body during dynamic tasks. Return to competitive sports is permitted only when the patient demonstrates functional symmetry, typically defined as a Limb Symmetry Index (LSI) greater than 90% on single-leg hop testing, isokinetic dynamometry, and complete resolution of patellofemoral pain during sport-specific drills.
Summary of Landmark Literature and Clinical Guidelines
Historical Perspectives on Patellofemoral Surgery
The evolution of patellofemoral surgery is deeply rooted in the pioneering observations of early 20th-century surgeons. Aleman's introduction of the term chondromalacia patellae in 1928 laid the groundwork for understanding basal cartilage degeneration. Subsequently, Caffey's definitive description of the dorsal defect in 1972 and Saupe's morphological classification of the bipartite patella provided the orthopedic community with the necessary frameworks to differentiate benign developmental variants from true pathological entities. Historically, the surgical management of severe patellar disorders leaned heavily toward radical excision, culminating in the widespread use of patellectomy. However, biomechanical studies in the late 20th century unequivocally demonstrated the catastrophic loss of extensor power following patellectomy, driving a paradigm shift toward joint preservation.
Evidence-Based Guidelines for Cartilage Restoration
Contemporary clinical guidelines heavily emphasize biological preservation and targeted biomechanical realignment. Arandes-Renu et al. provided landmark evidence supporting the efficacy of arthroscopic excision and marrow stimulation for unsalvageable OCD lesions, demonstrating excellent long-term functional scores with minimal activity restriction at 4-year follow-ups. For salvageable lesions, Marandola and Prietto established the biomechanical superiority of rigid internal fixation using countersunk screws or bioabsorbable pins, a technique now considered the gold standard for large, unstable OCD fragments in young patients. Furthermore, the management of symptomatic bipartite patellae was revolutionized by Mori, Adachi, and Ogata, whose collective work validated the subperiosteal release of the vastus lateralis as a definitive, tissue-sparing alternative to fragment excision.
Contemporary Outcomes of Realignment Procedures
The surgical management of advanced patellofemoral malalignment and chondromalacia is dominated by the principles established by Maquet and subsequently refined by Fulkerson. Fulkerson's introduction of the anteromedialization (AMZ) osteotomy provided a powerful tool to simultaneously correct lateral maltracking and offload the distal-lateral articular facets. Long-term outcome studies of the Fulkerson osteotomy consistently report good to excellent results in over 80% of patients, with significant delays in the progression to end-stage osteoarthritis. Current consensus guidelines mandate that such realignment procedures be meticulously templated using modern CT or MRI parameters, specifically targeting a postoperative TT-TG distance of 10 to 12 millimeters, to ensure optimal kinematic restoration and long-term joint survivorship.
