Disorders of Tendons and Fascia: Posterior Tibial Tendon Insufficiency
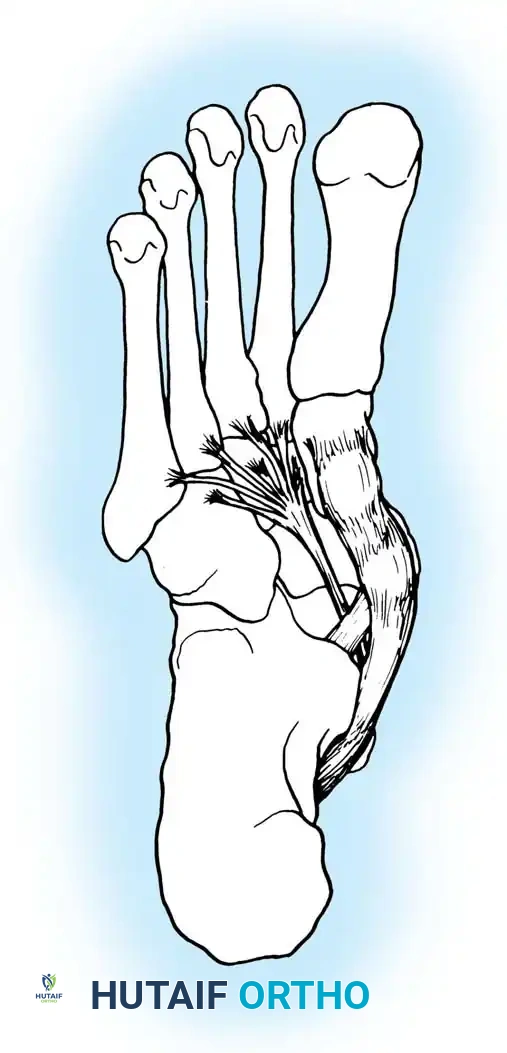
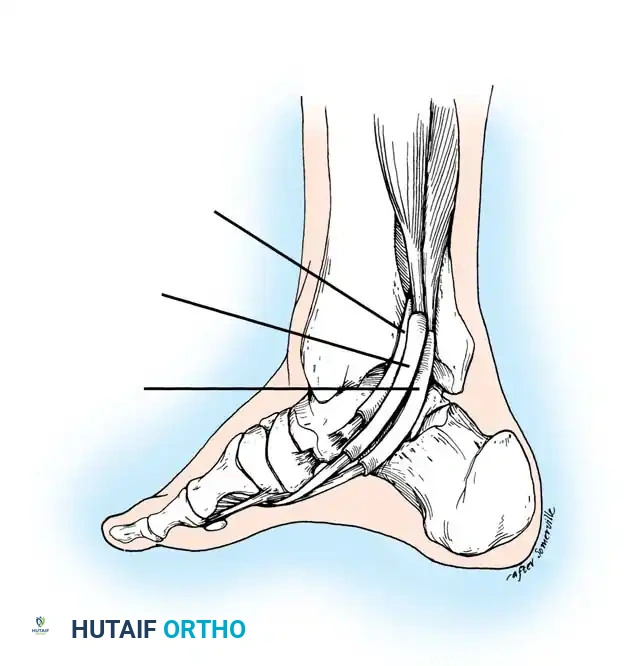
Chronic tenosynovitis (whether traumatic, degenerative, or secondary to inflammatory arthropathies), loss of tendon continuity, and the disruption of normal anatomical relationships at the tendon's insertion (such as the accessory navicular or prehallux syndrome) frequently render the posterior tibial tendon (PTT) insufficient. When the PTT fails to perform its critical biomechanical tasks—plantar flexion, hindfoot inversion, and dynamic stabilization of the medial longitudinal arch—the resulting clinical cascade is termed Posterior Tibial Tendon Insufficiency (PTTI).
Other than the rupture of the Achilles tendon, no single muscle-tendon unit distal to the knee can precipitate as profound a functional deficit as the loss of the posterior tibial tendon. Any pathological state that diminishes the effective excursion of this tendon produces a hallmark clinical deformity: the asymmetrical adult acquired flatfoot.
Biomechanics and Pathoanatomy of the Asymmetrical Flatfoot
The components of the PTTI deformity are triplanar:
* Hindfoot Valgus: Driven by the unopposed pull of the peroneus brevis.
* Midfoot Abduction: Occurring primarily at the midtarsal (transverse tarsal) joint.
* Forefoot Pronation (Supination relative to the hindfoot): A compensatory mechanism to keep the medial column on the ground despite hindfoot valgus.
This description applies most accurately to the weight-bearing posture of the foot. The severity of each component varies based on the magnitude of PTT dysfunction, the specific location of bony collapse within the medial longitudinal arch, the chronicity of the insufficiency, the rigidity of the deformity, and the baseline configuration of the patient's arch prior to the onset of disease.
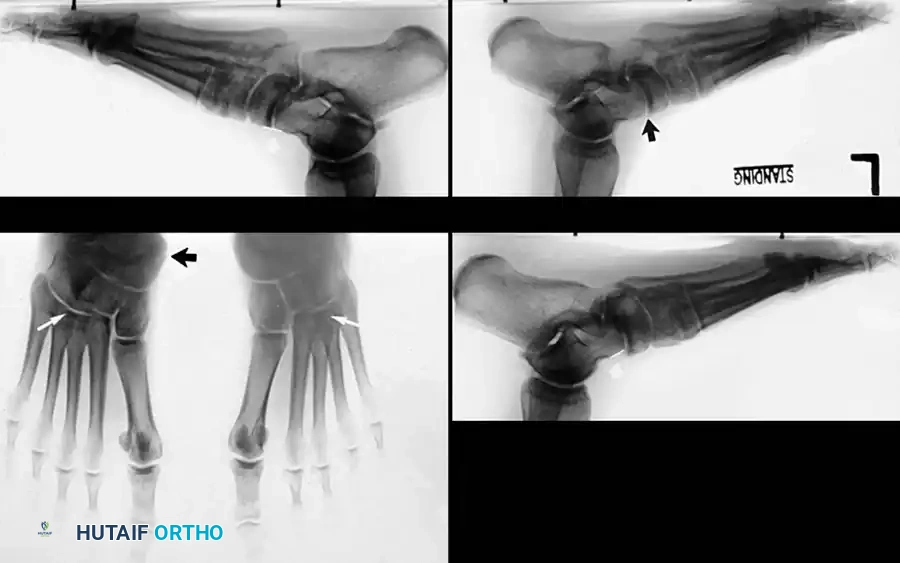
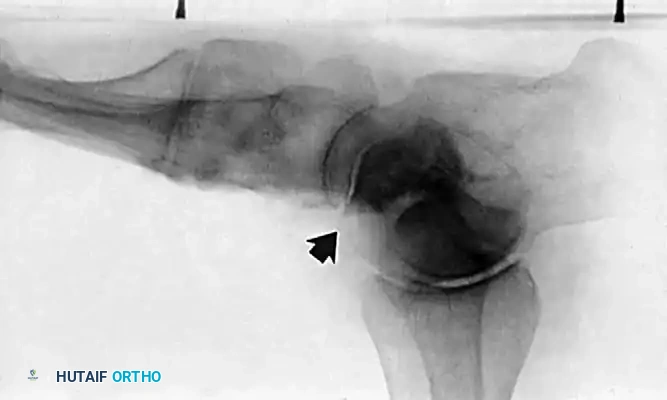
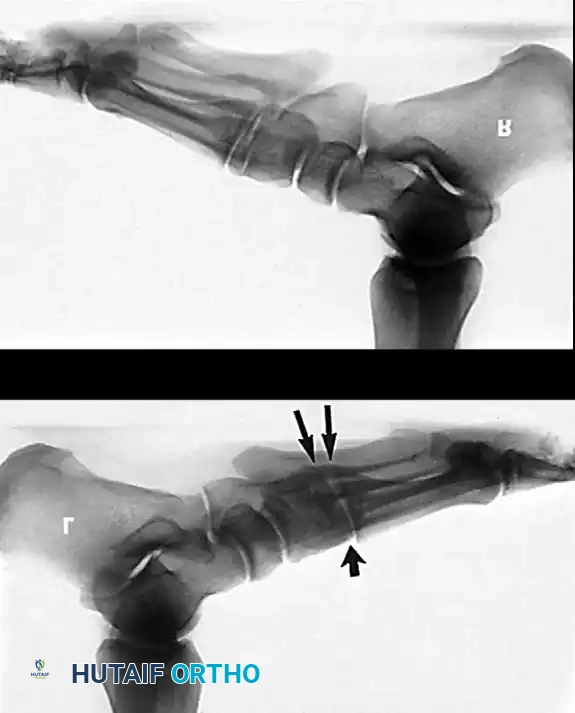
Clinical Pearl: The loss of the medial longitudinal arch can occur at the talonavicular, navicular-cuneiform, or cuneiform-metatarsal articulations. A weight-bearing lateral radiograph may initially show no bony collapse, appearing identical to the asymptomatic contralateral foot, even in the presence of obvious clinical pes planus.
Secondary Ligamentous Failure
Recognizing the secondary soft-tissue changes that accompany long-standing PTTI is paramount for surgical planning. As the hindfoot drifts into valgus and the midfoot abducts, immense strain is placed on the static ligamentous supporting structures of the medial arch.
- Spring Ligament Complex: The plantar calcaneonavicular (spring) ligament undergoes significant stretching and attenuation, gradually losing its ability to support the talar head.
- Talocalcaneal Interosseous Ligament: Frequently becomes incompetent, exacerbating subtalar instability.
- Plantar Fascia and Medial Column Ligaments: Ligaments supporting the navicular-cuneiform and cuneiform–first metatarsal joints elongate under chronic strain.
- Deltoid Ligament: In severe, end-stage cases, the superficial deltoid ligament (specifically the anterior or tibionavicular portion) elongates. This represents a critical transition into medial ankle instability and tibiotalar tilt.



Clinical Evaluation and Diagnosis
The clinical presentation of PTTI varies heavily depending on the etiology and chronicity of the insufficiency.
Symptomatology
If recurrent tenosynovitis is the primary driver, medial ankle and hindfoot pain will predominate. If unchecked, the inflammatory process leads to edema and mechanical blockage beneath the flexor retinaculum (laciniate ligament). Patients often "decommission" the muscle-tendon unit involuntarily because contraction elicits severe pain.
Patients frequently report:
* Foot and ankle fatigue after limited weight-bearing activity.
* A sensation of the foot "rolling out" or lacking support.
* Difficulty fitting into standard footwear.
* Pain Shift: Initially, pain is localized medially along the PTT sheath. However, with long-standing pronation and hindfoot valgus, the pain shifts laterally. This lateral pain is caused by subfibular impingement, where the anterior surface of the lateral process of the talus impinges against the floor of the sinus tarsi or the calcaneus impinges against the fibula.
Physical Examination
A meticulous physical examination is the cornerstone of diagnosing PTTI.
1. Weight-Bearing Assessment:
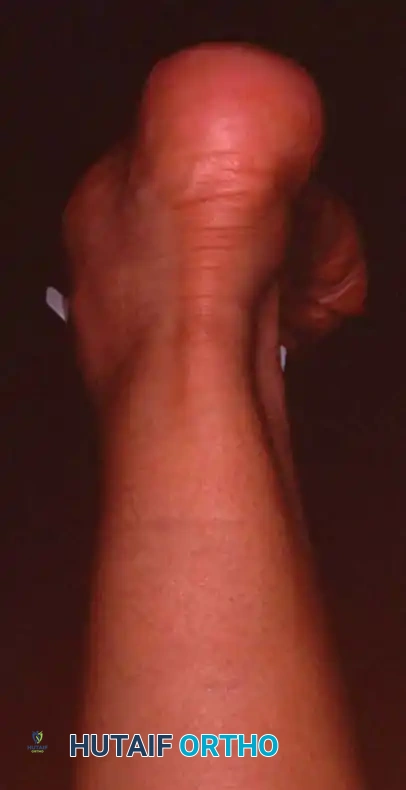
Observe the patient from the anterior and posterior aspects while standing. Look for the classic "too many toes" sign from behind, indicative of severe midfoot abduction.


2. The Single-Leg Heel Rise Test:
This is the most critical functional test for PTT integrity.
* Normal Biomechanics: When a patient rises on one toe, the intact PTT inverts the calcaneus. This inversion locks the transverse tarsal joint (talonavicular and calcaneocuboid joints), converting the midfoot into a rigid lever arm for push-off.
* Pathological Finding: In PTTI, the patient cannot invert the heel. The heel remains in valgus, the transverse tarsal joint remains unlocked, and the patient either cannot lift the heel off the ground or does so with profound weakness and pain.
Surgical Warning: Do not be fooled by patients with supple deformities who "throw" their hindfoot into a locked position by gaining momentary support from an examining table and using the gastrocnemius-soleus complex to cheat the movement. True, unassisted single-leg heel inversion is virtually impossible with a ruptured PTT.
3. Gait Analysis:
In a normal gait cycle, the stance phase begins with the hindfoot in slight inversion, moves to valgus during midstance, and returns to inversion at terminal stance (toe-off). In PTTI, the hindfoot remains locked in valgus throughout the entire stance phase, resulting in an apropulsive, flat-footed gait.





Staging of Posterior Tibial Tendon Insufficiency
The classification system originally developed by Johnson and Strom (1989), and later modified by Myerson, dictates the surgical algorithm.
Stage I Disease
- Pathology: Tenosynovitis with tendon continuity.
- Clinical Findings: Swelling, pain, and inflammation along the PTT sheath. Mild weakness may be present due to pain, but there is no deformity.
- Function: The patient can successfully perform a single-leg toe raise and actively invert the foot.
Stage II Disease
- Pathology: Elongation or partial/complete rupture of the PTT.
- Clinical Findings: Loss of PTT function resulting in a flexible flatfoot deformity (hindfoot valgus, midfoot abduction). Mild lateral sinus tarsi pain may begin to manifest.
- Function: Inability to perform a single-leg toe raise. The anterior tibial muscle often attempts to compensate as an accessory inverter.
Stage III Disease
- Pathology: Chronic PTT rupture with secondary joint contractures.
- Clinical Findings: A fixed, rigid hindfoot valgus and midfoot abduction deformity. Significant lateral sinus tarsi impingement pain is the primary complaint.
- Radiography: Degenerative arthritic changes are visible in the subtalar and/or talonavicular joints.
Stage IV Disease (Myerson Modification)
- Pathology: Deltoid ligament failure in addition to Stage III findings.
- Clinical Findings: Valgus tilt of the talus within the ankle mortise. The deformity involves not just the hindfoot, but the tibiotalar joint itself.



Surgical Management and Operative Techniques
Surgical intervention is dictated strictly by the stage of the disease, the flexibility of the deformity, and the presence of degenerative joint changes.
Stage I: Tenosynovectomy and Debridement
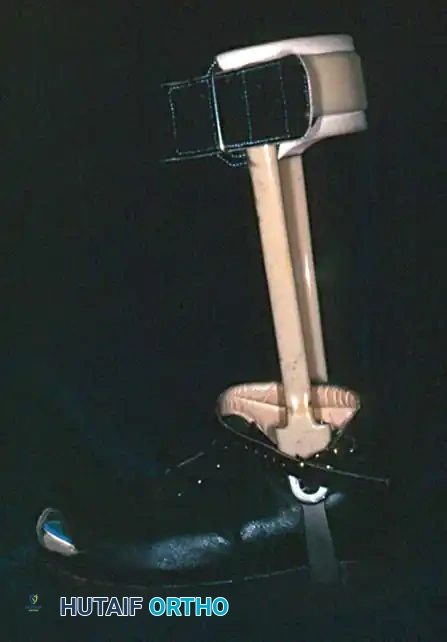
When conservative management (immobilization, NSAIDs, orthotics) fails after 3 to 6 months, surgical debridement is indicated.
Surgical Technique:
1. Incision: A longitudinal incision is made 1 cm posterior to the medial malleolus, extending distally to the navicular insertion.
2. Exposure: The flexor retinaculum is incised. The PTT is elevated and inspected 360 degrees.
3. Debridement: Hypertrophic synovium is aggressively excised. If longitudinal splits or partial tears are identified within the tendon substance, they are debrided and tubularized using 5-0 non-absorbable suture.
4. Closure: The retinaculum is left partially open to prevent stenosis, and the skin is closed in layers.


Stage II: Joint-Sparing Reconstruction
Stage II disease requires a combination of soft-tissue reconstruction (to restore the motor unit) and bony osteotomies (to correct the biomechanical axis and protect the tendon transfer).
1. Flexor Digitorum Longus (FDL) Transfer:
The FDL is the ideal transfer candidate due to its in-phase firing pattern, proximity, and adequate strength.
* The PTT is excised if severely degenerated, or left in situ if viable.
* The FDL is identified posterior to the PTT, harvested distally at the master knot of Henry, and transected.
* A drill hole is created dorsal-to-plantar through the navicular.
* The FDL is passed through the navicular and sutured to itself or secured with a bio-tenodesis screw under maximal tension with the foot held in plantarflexion and inversion.
2. Medial Displacement Calcaneal Osteotomy (MDCO):
To correct hindfoot valgus and shift the mechanical axis medially, reducing strain on the FDL transfer.
* An oblique lateral incision is made posterior to the sural nerve.
* An osteotomy is performed posterior to the posterior facet of the subtalar joint, angled 45 degrees to the plantar surface.
* The posterior tuberosity is translated medially by 10 to 15 mm.
* Fixation is achieved with one or two large-fragment (6.5 mm or 7.3 mm) cannulated screws.
3. Lateral Column Lengthening (Evans Osteotomy):
Indicated if severe midfoot abduction is present (uncovering of the talar head > 40%).
* An osteotomy is made 1.5 cm proximal to the calcaneocuboid joint.
* A tricortical iliac crest allograft or autograft (usually 8-10 mm) is impacted into the osteotomy site to lengthen the lateral column, swinging the midfoot out of abduction.



Stage III: Arthrodesis
Once the deformity becomes rigid or degenerative arthritic changes are present in the hindfoot, joint-sparing procedures are contraindicated. Arthrodesis is required to correct the deformity and eliminate pain.
Triple Arthrodesis:
The gold standard for rigid Stage III PTTI. It involves the fusion of the subtalar, talonavicular, and calcaneocuboid joints.
* Approach: A dual-incision technique is standard. A lateral incision over the sinus tarsi exposes the subtalar and calcaneocuboid joints. A medial incision exposes the talonavicular joint.
* Preparation: All articular cartilage is meticulously denuded down to bleeding subchondral bone using curettes and osteotomes.
* Correction: The deformity is corrected by manipulating the joints. The hindfoot must be fused in 0 to 5 degrees of valgus. Never fuse the hindfoot in varus.
* Fixation: Large cannulated screws are used for the subtalar joint (calcaneus to talus). The talonavicular and calcaneocuboid joints are fixed with screws or specialized locking plates.
Pitfall: Failure to adequately prepare the talonavicular joint is the most common cause of nonunion in a triple arthrodesis. Ensure aggressive decortication and rigid compression.





Stage IV: Tibiotalocalcaneal (TTC) Arthrodesis
In Stage IV disease, the deltoid ligament has failed, leading to talar tilt and ankle joint arthropathy. Fusing the hindfoot alone will not correct the ankle instability.
Surgical Technique:
* A transfibular or anterior approach is utilized to expose the tibiotalar and subtalar joints.
* The articular surfaces of the ankle and subtalar joints are prepared.
* The talus is centralized beneath the tibia.
* Fixation is typically achieved using a retrograde intramedullary TTC nail inserted through the plantar aspect of the calcaneus, traversing the talus, and locking into the tibial diaphysis. Supplemental compression screws may be
Associated Surgical & Radiographic Imaging