Masterclass: Surgical Management of Thumb Metacarpophalangeal Joint Volar Instability and Dislocations
Key Takeaway
Join our masterclass on thumb MP joint volar instability and dislocations. Learn comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution for open reduction and volar plate advancement. We cover critical pearls, pitfalls, and essential postoperative rehabilitation, guiding you through every micro-step to ensure optimal outcomes for challenging thumb injuries.
Comprehensive Introduction and Patho-Epidemiology
The thumb metacarpophalangeal (MP) joint represents a critical anatomical fulcrum, serving as the foundational cornerstone for nearly every prehensile function of the human hand. While the trapeziometacarpal (basal) joint affords the thumb its sweeping circumduction and opposition, it is the rigid stability of the MP joint that allows for the transmission of powerful pinch and grip forces. When we encounter thumb metacarpophalangeal joint volar instability and dislocations, we are faced with a pathology that profoundly disrupts the entire kinetic chain of the hand. The inherent stability of this joint is paramount; without it, the ability to effectively oppose the other digits is lost, rendering fine motor tasks clumsy and power grips critically weakened.

The epidemiology of thumb MP joint dislocations dictates that dorsal dislocations are overwhelmingly more common than their volar counterparts. The classic mechanism of injury for a dorsal dislocation involves a sudden, violent hyperextension force applied to the proximal phalanx, often encountered in contact sports, falls on an outstretched hand, or direct axial loading. This abrupt vector forces the proximal phalanx dorsally, sequentially rupturing the volar plate from its membranous proximal attachment on the metacarpal neck, and occasionally tearing the collateral ligaments. In contrast, true volar dislocations are exceedingly rare anomalies in the orthopedic literature. They typically result from a complex, combined mechanism of forced hyperflexion coupled with a torsional or shearing stress, leading to the rupture of the dorsal capsule, the extensor mechanism, and frequently the collateral ligaments.
The pathogenesis of chronic volar instability, distinct from acute dislocation, often stems from unrecognized or inadequately treated acute hyperextension injuries. When the restraining structures on the volar surface of the joint—specifically the stout fibrocartilaginous volar plate and its associated sesamoid complex—are disrupted and fail to heal in anatomic tension, it leads to excessive joint excursion and abnormal hyperextension. This is not merely a cosmetic deformity; it is a profoundly painful condition that causes significant functional deficits. Furthermore, we must recognize that a subset of patients presenting with multidirectional instability may suffer from generalized ligamentous laxity, such as Ehlers-Danlos syndrome or benign joint hypermobility syndrome. In these cohorts, the surgical approach must be carefully modulated, as their native collagen is inherently flawed.

The natural history of untreated or neglected thumb MP joint instability is a predictable progression toward debilitating dysfunction. Post-traumatic instability left unaddressed will invariably lead to persistent weakness of pinch and grip, chronic pain, and an altered mechanical axis. Over time, the abnormal kinematics and shear forces across the articular cartilage will precipitate premature degenerative joint disease (arthrosis). This underscores the absolute necessity for the orthopedic surgeon to maintain a high index of suspicion, perform a meticulous clinical evaluation, and execute precise surgical intervention when indicated to restore the delicate biomechanical balance of the thumb.
Detailed Surgical Anatomy and Biomechanics
Osteology and Joint Characteristics
The thumb MP joint exhibits a fascinating and highly variable blend of biomechanics, possessing features of both a ginglymus (hinge) joint and a diarthrodial condyloid joint. While it primarily functions in a flexion-extension arc, much like a true hinge, there are subtle but biomechanically vital elements of rotation and abduction-adduction in the healthy joint. This is largely dictated by the inherent spectrum of metacarpal head geometry observed across the population. The metacarpal head is asymmetric, being broader volarly than dorsally, which creates a "cam effect."

The specific morphology of the metacarpal head significantly influences the available range of motion. Patients with more spherical, rounded metacarpal heads exhibit greater flexion, extension, and rotational freedom. Conversely, individuals with flatter, more rectangular metacarpal heads inherently possess a much more restricted arc of motion. This anatomical variability is crucial to appreciate when assessing stability, as a "normal" degree of laxity in a spherical joint may represent pathologic instability in a flattened joint. The articular congruity is further stabilized by the proximal phalanx, which presents a shallow, concave articular surface that relies heavily on soft tissue constraints to prevent subluxation.

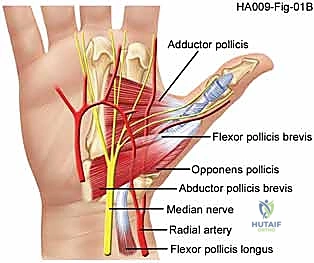
Volar Stabilizers and the Sesamoid Complex
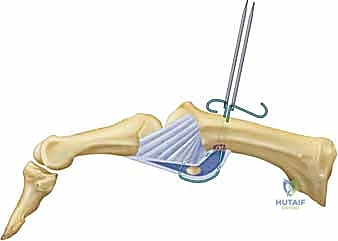
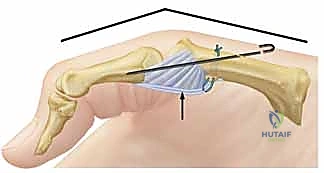
The volar plate is the paramount stabilizing structure against hyperextension forces, serving as the robust, fibrocartilaginous floor of the MP joint. Distally, it has a thick, rigid attachment to the volar base of the proximal phalanx. Proximally, it thins into a membranous, compliant tissue that attaches to the metacarpal neck, allowing it to glide proximally during joint flexion. The integrity of this structure is absolutely essential for volar stability; its rupture is the sine qua non of dorsal dislocations and chronic hyperextension instability.

Adding crucial dynamic and static volar support is the sesamoid complex and the insertions of the thenar intrinsic muscles. The adductor pollicis inserts into the ulnar sesamoid, while the flexor pollicis brevis and abductor pollicis brevis insert into the radial sesamoid. These sesamoids are intimately embedded within the substance of the volar plate, acting as mechanical fulcrums that enhance the mechanical advantage of the intrinsic flexors. The intersesamoid ligament bridges these two ossicles, creating a fibro-osseous tunnel through which the flexor pollicis longus (FPL) tendon glides. Disruption of this complex not only causes instability but can lead to complex dislocations where the metacarpal head buttonholes through the intrinsic musculature.

Collateral Ligaments and Dorsal Structures
The collateral ligaments provide the primary restraint against valgus and varus stresses, contributing significantly to mediolateral stability. The proper collateral ligaments (PCL) originate from the dorsal-lateral condyles of the metacarpal and pass obliquely to insert on the palmar-proximal aspect of the proximal phalanx. Due to the cam effect of the metacarpal head, the PCLs are maximally taut in flexion. The accessory collateral ligaments (ACL) originate more volarly and proximally, fanning out to insert onto the volar plate and the sesamoids. The ACLs are taut in extension, effectively suspending the volar plate against the metacarpal head.

Dorsally, the stability is augmented by the extensor mechanism. The extensor pollicis brevis (EPB) inserts onto the dorsal base of the proximal phalanx, while the extensor pollicis longus (EPL) traverses the joint to insert at the base of the distal phalanx. The adductor and abductor aponeuroses contribute transverse fibers to the extensor hood, providing a modicum of dynamic lateral stability. The dorsal capsule itself is relatively thin and redundant to allow for full flexion, making it highly susceptible to rupture during the rare volar dislocation events.

Neurovascular Anatomy and Surgical Perils
During any volar or mid-lateral approach to the thumb MP joint, the digital neurovascular bundles are at paramount risk and demand meticulous identification. On both the radial and ulnar aspects of the thumb, these bundles course longitudinally, intimately associated with the flexor tendon sheath and the A1 pulley. The radial digital nerve is particularly vulnerable as it crosses obliquely over the flexor sheath near the level of the MP joint.

The arterial supply to the MP joint is derived from branches of the princeps pollicis artery, which bifurcates into the radial and ulnar digital arteries. These vessels are typically found just volar to the collateral ligaments, deep to the skin and subcutaneous fat. Meticulous blunt dissection, the use of loupe magnification, and gentle retraction with vessel loops are non-negotiable tenets of this surgery to prevent catastrophic iatrogenic injury, neuroma formation, or devascularization of the digit.
Exhaustive Indications and Contraindications
The decision-making paradigm for surgical intervention in thumb MP joint instability and dislocations requires a nuanced understanding of the injury chronicity, the specific structures involved, and the patient's functional demands. Acute dislocations are broadly categorized into simple (reducible via closed means) and complex (irreducible). Complex dislocations mandate emergent or urgent open reduction. Volar dislocations are almost universally complex due to the interposition of the dorsal capsule, the EPB, or the EPL into the joint space, acting as a mechanical block to closed reduction.

For chronic volar instability, the indications for surgery are driven by persistent pain, weakness in pinch grip, and a demonstrable hyperextension deformity that fails conservative management (such as figure-of-eight splinting or extension-block orthoses). If a patient exhibits a symptomatic hyperextension laxity of greater than 20 to 30 degrees compared to the contralateral normal thumb, surgical reconstruction of the volar plate (capsulodesis) or advancement is highly indicated to prevent the inevitable progression to arthrosis.

Contraindications must be rigorously respected to avoid catastrophic outcomes. Active local or systemic infection is an absolute contraindication to any elective joint reconstruction or open reduction with internal fixation. Severe, pre-existing degenerative joint disease (osteoarthritis) of the MP joint renders soft tissue reconstruction futile; in such cases, primary MP joint arthrodesis is the procedure of choice. Relative contraindications include severe medical comorbidities precluding anesthesia, profound patient non-compliance, and heavy tobacco use, which significantly impairs soft tissue healing and microvascular perfusion.
| Category | Indications for Surgical Management | Contraindications for Surgical Management |
|---|---|---|
| Acute Injuries | Irreducible (complex) dorsal or volar dislocations; Open dislocations; Associated unstable intra-articular fractures; Concomitant neurovascular compromise. | Reducible (simple) dislocations with a stable post-reduction arc of motion; Medical instability precluding safe anesthesia. |
| Chronic Injuries | Symptomatic hyperextension instability failing conservative care; Painful pinch/grip weakness; Volar plate incompetence >20-30 degrees vs. contralateral side. | Advanced MP joint arthrosis (requires arthrodesis instead); Active local soft tissue infection; Severe generalized ligamentous laxity without functional deficit. |
| Patient Factors | High-demand manual laborers; Athletes requiring stable pinch; Patients committed to rigorous post-operative rehabilitation. | Uncontrolled psychiatric disorders; Severe non-compliance; Active heavy smoking (relative contraindication due to healing risk). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Advanced Diagnostics
Our surgical journey begins long before the first incision, anchored in an exhaustive preoperative clinical and radiographic evaluation. The history must meticulously detail the mechanism of injury. In acute settings, understanding the vector of force—whether pure hyperextension, hyperflexion, or combined rotational shear—provides invaluable clues regarding the disrupted structures. The surgeon must inquire about previous attempts at closed reduction, as forceful, repeated attempts by untrained personnel often convert a simple dislocation into a complex one by driving the metacarpal head through the volar structures.

Physical examination begins with observation of the resting posture. A complex dorsal dislocation presents with the proximal phalanx resting in hyperextension, with a prominent volar metacarpal head palpable in the thenar eminence. A pathognomonic sign of a complex dorsal dislocation is a slight dimpling of the volar skin, caused by the metacarpal head buttonholing through the volar plate and intrinsic muscles, placing the skin under immense tension. Range of motion assessment of the interphalangeal (IP) joint is critical; limited or absent IP joint flexion strongly suggests entrapment of the flexor pollicis longus (FPL) tendon around the metacarpal neck, an absolute indication for open reduction.

Radiographic Analysis
Plain radiography remains the cornerstone of our imaging evaluation. Standard anteroposterior (AP), true lateral, and Robert's (pronated AP) views are mandatory. In acute dislocations, the lateral view will clearly delineate the direction of the displacement. The surgeon must scrutinize the films for associated avulsion fractures, particularly at the volar base of the proximal phalanx, which indicate a bony avulsion of the volar plate.
A critical radiographic finding in complex dorsal dislocations is the presence of a sesamoid bone within the widened joint space on the AP or lateral radiograph. This "sesamoid sign" implies that the volar plate, which houses the sesamoids, has been completely avulsed and interposed between the articular surfaces, rendering closed reduction impossible. In chronic instability cases, stress radiographs (performed under local anesthesia if necessary) can quantify the degree of hyperextension laxity compared to the contralateral digit. Advanced imaging, such as a non-contrast MRI, is rarely needed for acute dislocations but can be invaluable in chronic cases to assess the viability of the volar plate tissue, the presence of occult osteochondral defects, or concomitant collateral ligament pathology.
Patient Positioning and Surgical Preparation
Optimal patient positioning and meticulous preparation of the surgical field are essential for a seamless operation. The patient is positioned supine on the operating table with the affected upper extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is absolutely critical for the safe identification of the delicate digital neurovascular bundles.

Anesthesia can be achieved via a regional brachial plexus block (supraclavicular or axillary) or general anesthesia, depending on patient preference and comorbidities. A wide sterile prep and drape are performed, exposing the hand and forearm. A sterile C-arm fluoroscopy unit must be positioned perpendicular to the hand table, readily available to confirm joint reduction, assess hardware placement, and perform dynamic stress testing intraoperatively. The surgeon should sit comfortably at the axilla, utilizing loupe magnification (minimum 2.5x to 3.5x) and a dedicated hand surgery instrument set equipped with fine skin hooks, tenotomy scissors, and miniature retractors.
Step-by-Step Surgical Approach and Fixation Technique
The Volar Approach for Dorsal Dislocations and Volar Plate Repair
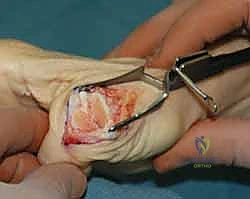
For complex dorsal dislocations and chronic volar plate instability, the volar approach is the gold standard, providing direct access to the pathology. A volar zigzag (Bruner) incision or a mid-lateral incision is utilized. The Bruner incision is centered over the MP joint, with the apices of the flaps carefully planned to avoid crossing the flexion creases at right angles, thereby preventing post-operative scar contracture.

Upon incising the skin and subcutaneous tissue, the superficial fascia is bluntly dissected. The absolute first priority is the identification and protection of the radial and ulnar digital neurovascular bundles. The radial digital nerve is particularly superficial and crosses the operative field obliquely; it must be mobilized gently with vessel loops and retracted laterally. Once the neurovascular structures are secured, the A1 pulley of the flexor tendon sheath is exposed. In complex dislocations, the metacarpal head is often found protruding through a rent in the joint capsule, trapped between the flexor pollicis brevis, the lumbrical, and the FPL tendon.

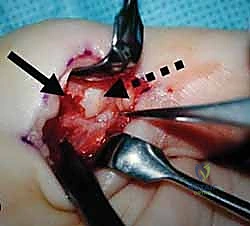
Joint Decompression and Reduction
The crux of the open reduction is relieving the tension on the structures that are strangulating the metacarpal head. The A1 pulley is longitudinally incised to mobilize the FPL tendon. The surgeon will typically find the avulsed volar plate interposed dorsally between the proximal phalanx and the metacarpal head. Under direct vision, a blunt Freer elevator or a small retractor is used to meticulously extract the volar plate from the joint space.
Once the interposed tissue is cleared, longitudinal traction is applied to the thumb, coupled with volar translation of the proximal phalanx and flexion of the MP joint. The joint should reduce with a palpable and visible "clunk." It is imperative to avoid forceful leverage during reduction to prevent iatrogenic osteochondral fractures of the metacarpal head. Following reduction, the joint is taken through a full arc of motion to ensure stability and confirm that the FPL tendon is gliding freely without entrapment.

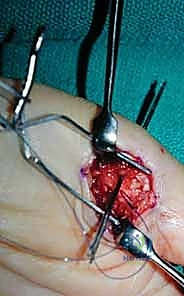
Volar Plate Reconstruction and Fixation
With the joint reduced, attention turns to the definitive repair of the volar plate. In acute avulsions from the base of the proximal phalanx, direct repair is indicated. The bony footprint on the volar base of the proximal phalanx is debrided of fibrous tissue to a bleeding cancellous bed using a small curette or a rongeur. Fixation is most robustly achieved utilizing modern micro-suture anchors (1.3mm to 1.5mm) loaded with high-strength non-absorbable suture.

The anchors are placed into the volar-proximal aspect of the phalanx. The sutures are then passed through the robust distal edge of the volar plate using a horizontal mattress or Krackow configuration. The joint is held in approximately 20 to 30 degrees of flexion to remove tension from the repair, and the sutures are securely tied. In cases of chronic instability where the volar plate is attenuated, a formal capsulodesis may be required. This involves advancing the volar plate distally and securing it into a bony trough created at the base of the phalanx. If the tissue is entirely unviable, a tendon graft (such as the palmaris longus) can be utilized to reconstruct the volar restraints, weaving the graft through drill holes in the metacarpal neck and proximal phalanx.

The Dorsal Approach for Volar Dislocations
In the rare event of a complex volar dislocation, a dorsal approach is typically necessitated, as the pathology involves the interposition of dorsal structures. A longitudinal or curvilinear dorsal incision is made over the MP joint. The extensor hood is identified, and a longitudinal split is made between the EPB and EPL tendons.

The surgeon will typically encounter the ruptured dorsal capsule and the extensor mechanism interposed into the joint, blocking reduction. These structures are carefully extricated using a blunt hook or elevator. Once cleared, the joint is reduced via longitudinal traction and dorsal translation. The dorsal capsule and the extensor hood are then meticulously repaired with absorbable sutures. Regardless of the approach (volar or dorsal), if the joint remains grossly unstable post-reduction and soft-tissue repair, temporary transarticular stabilization utilizing a 0.045-inch Kirschner wire (K-wire) driven obliquely across the MP joint in a functional position (20 degrees of flexion) may be employed for 3 to 4 weeks.
Complications, Incidence Rates, and Salvage Management
The surgical management of the thumb MP joint, while highly successful in restoring stability, is fraught with potential complications that the surgeon must anticipate and mitigate. The most ubiquitous complication following both acute dislocation management and chronic instability reconstruction is post-operative stiffness. The MP joint is notoriously unforgiving to prolonged immobilization. Loss of terminal flexion and extension occurs in up to 30-40% of patients, primarily due to capsular scarring, adherence of the extensor mechanism, or over-tensioning of a capsulodesis.

Recurrent instability is a devastating complication, occurring in approximately 5-10% of cases. This typically results from technical errors during surgery, such as inadequate fixation of the volar plate, failure to recognize concomitant collateral ligament ruptures, or patient non-compliance with post-operative immobilization protocols. If a patient presents with recurrent hyperextension instability, a thorough re-evaluation with stress radiography and MRI is required. Revision soft tissue reconstruction is technically demanding and carries a higher failure rate, often necessitating the use of autologous tendon grafts to augment the attenuated tissues.

Neurovascular complications, particularly injury to the radial digital nerve, are a significant risk during the volar approach. Neurapraxia due to aggressive retraction is common and usually resolves within weeks to months. However, iatrogenic transection of the nerve requires immediate microsurgical epineural repair and can result in permanent sensory deficits and painful neuroma formation. Deep surgical site infection and hardware failure (anchor pullout or K-wire migration) are rare (<2%) but mandate prompt intervention, including debridement, hardware removal, and targeted antibiotic therapy.

When soft tissue reconstruction fails unequivocally, or when chronic instability has precipitated severe, painful post-traumatic arthrosis, salvage procedures must be employed. Arthroplasty (joint replacement) of the thumb MP joint yields unpredictable results and is generally avoided in young, high-demand patients. The definitive, gold-standard salvage procedure is MP joint arthrodesis. Fusion of the joint in approximately 15 to 20 degrees of flexion, 10 degrees of abduction, and slight pronation provides a stable, pain-free pillar for pinch and grip, with high patient satisfaction rates despite the loss of motion.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Joint Stiffness | 30 - 40% | Prevention: Limit immobilization to 3-4 weeks; early protected ROM. Salvage: Aggressive hand therapy, dynamic splinting |
Clinical & Radiographic Imaging Archive