Cerebral Palsy: Comprehensive Diagnosis, Prognostic Evaluation, and Gait Analysis
Key Takeaway
The diagnosis of cerebral palsy relies primarily on a meticulous clinical history and physical examination, focusing on motor developmental milestones and the persistence of primitive reflexes. Quantitative gait analysis and the Gross Motor Function Classification System (GMFCS) are critical adjuncts. Together with examination under anesthesia, these diagnostic modalities guide orthopedic surgeons in formulating precise, multi-level surgical interventions to optimize ambulation and correct musculoskeletal deformities in the pediatric patient.
DIAGNOSIS AND CLINICAL EVALUATION OF CEREBRAL PALSY
Cerebral palsy (CP) represents a heterogeneous group of non-progressive, permanent disorders of movement and posture caused by a static lesion or developmental anomaly in the immature brain. While the neurological lesion is static, the musculoskeletal pathology is relentlessly progressive. Consequently, the orthopaedic surgeon’s role is to manage the evolving lever-arm dysfunctions, muscle contractures, and joint subluxations that arise from altered muscle tone and impaired motor control.
History and physical examination remain the paramount diagnostic tools. A meticulous history must encompass a thorough investigation of the prenatal, perinatal, and postnatal periods. Key factors include prematurity, low birth weight, anoxic brain injury, intraventricular hemorrhage, and periventricular leukomalacia. With the exception of several rare conditions—such as familial spastic paraparesis and congenital ataxia—there is no known genetic component to cerebral palsy.
Ancillary studies, including radiographs, hematological studies, chromosomal analysis, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET), are rarely required to establish the primary diagnosis. However, they are highly valuable in determining the anatomical extent of the brain injury (e.g., identifying periventricular leukomalacia in spastic diplegia) and ruling out progressive neurodegenerative disorders.
Clinical Pearl: Diagnosis of cerebral palsy before the age of 2 years is notoriously difficult and fraught with diagnostic pitfalls. Nelson and Ellenberg demonstrated that 55% of children diagnosed with cerebral palsy by 1 year of age did not meet the diagnostic criteria by age 7.
Differential Diagnosis and Diagnostic Pitfalls
When evaluating an infant for abnormal tone, the orthopaedic surgeon must consider physiological and ethnic variations, as well as transient conditions:
* Transient Dystonia of Prematurity: This condition is characterized by increased tone in the lower extremities between 4 and 14 months of age. It is frequently confused with spastic diplegic cerebral palsy. However, transient dystonia is a self-limiting condition that resolves spontaneously without surgical or medical intervention.
* Ethnic Variations in Muscle Tone: African American children statistically tend to exhibit higher baseline muscle tone compared to other ethnic groups during infancy. Failure to recognize this normal physiological variant can lead to an erroneous diagnosis of cerebral palsy.
MOTOR DEVELOPMENT AND PRIMITIVE REFLEXES
A profound understanding of normal motor developmental milestones and primitive reflexes is essential for identifying children with delayed motor maturation. Normal motor development proceeds in a strict cephalad-to-caudal pattern. It begins with bulbar functions (swallowing and sucking) present at birth, progresses to head control, and ultimately culminates in sphincter control between 24 and 36 months of age.
Early Motor Developmental Milestones
The following milestones serve as a baseline for evaluating developmental delay. Failure to achieve these milestones within the 95th percentile age range warrants rigorous neurological and orthopaedic evaluation.
- Head Control: Average Age: 3 months | 95th Percentile: 6 months
- Independent Sitting: Average Age: 6 months | 95th Percentile: 9 months
- Crawling: Average Age: 8 months | 95th Percentile: Variable (some normal children bypass crawling)
- Pull to Stand: Average Age: 8 months | 95th Percentile: 12 months
- Independent Walking: Average Age: 12 months | 95th Percentile: 17 months
The Role of Primitive Reflexes
Primitive reflex patterns are brainstem-mediated motor activities present in early infancy. In normal maturation, these reflexes are suppressed by the developing cerebral cortex. In children with cerebral palsy, the cortical inhibition is impaired, causing these primitive reflexes to persist longer than normal—and in severe cases, permanently.
Conversely, higher-level postural reactions (such as the parachute reaction and equilibrium responses), which are absolute prerequisites for normal independent ambulation, may be significantly delayed or may never manifest.
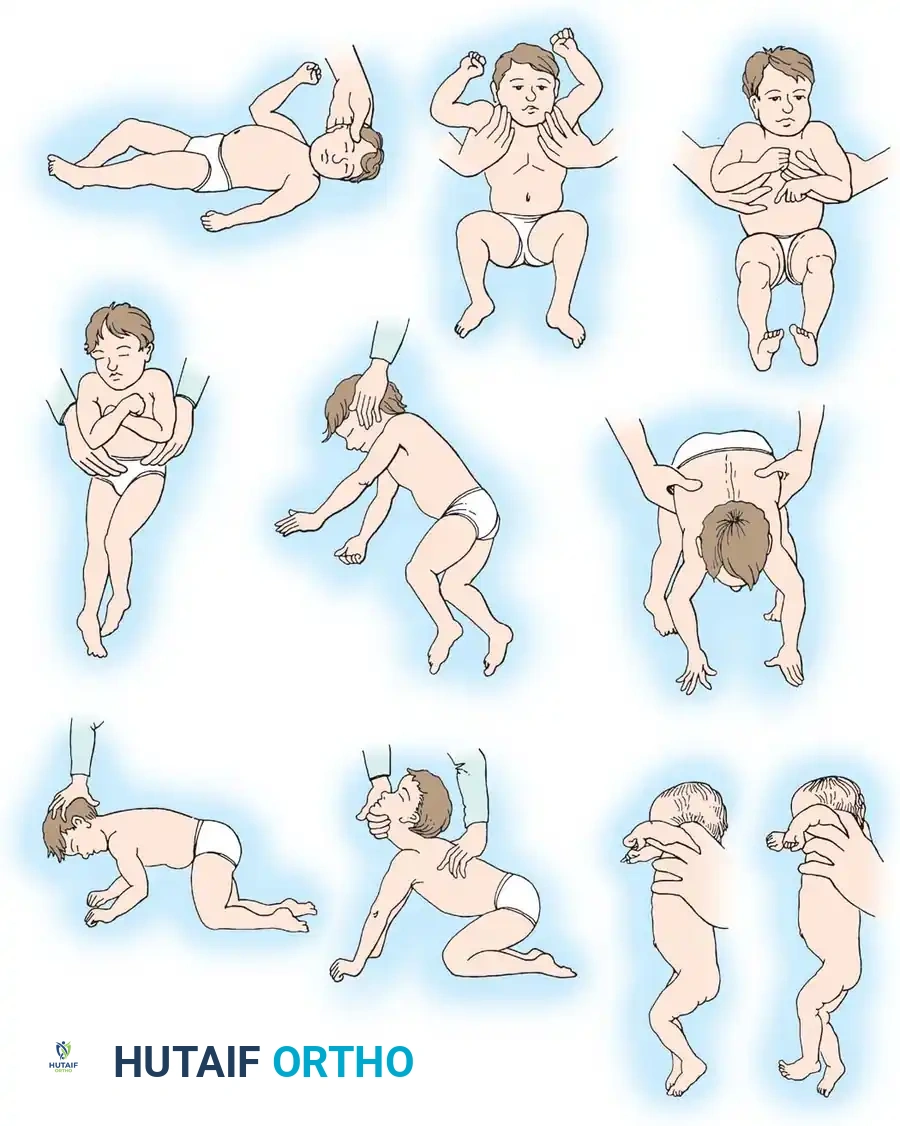
Figure 30-3: Pathological Persistence of Primitive Reflexes
* A. Asymmetrical Tonic Neck Reflex (ATNR): As the head is turned to one side, the ipsilateral arm and leg extend, while the contralateral arm and knee flex (the "fencer's posture"). An obligate ATNR prevents independent sitting and bimanual activities.
* B. Moro Reflex: Sudden neck extension causes the upper limbs to extend and abduct, followed by an embracing pattern of flexion and adduction.
* C. Extensor Thrust Reflex: When the infant is held upright under the armpits, the lower extremities stiffen into rigid extension.
* D. Neck-Righting Reflex: As the head is turned, the shoulders, trunk, pelvis, and lower extremities log-roll to follow the turned head.
* E. Parachute Reaction: A mature protective response. As the infant is suspended at the waist and suddenly lowered forward, the arms and hands extend to protect the head. Absence of this reflex after 11 months is a poor prognostic sign for ambulation.
* F. Symmetrical Tonic Neck Reflex (STNR): As the neck is flexed, the arms flex and the legs extend. As the neck is extended, the arms extend and the legs flex.
* G. Foot Placement Reaction: When the dorsum of the foot is stroked against the underside of a table, the infant automatically steps up and places the foot flat on the surface.
Surgical Warning: The persistence of primitive reflexes not only indicates severe neurological impairment but actively contributes to the development of musculoskeletal deformities. For example, a persistent ATNR can lead to unilateral hip subluxation or dislocation on the flexed (contralateral) side due to unopposed adductor and flexor spasticity.
By systematically determining which reflexes are present or absent, the clinician can calculate the child’s Neurological Age. Comparing the neurological age with the chronological age yields a Neurological Quotient, a vital metric for determining long-term prognosis and formulating a surgical treatment algorithm.
GROSS MOTOR FUNCTION CLASSIFICATION SYSTEM (GMFCS)
The GMFCS is an internationally validated, age-specific observational system that classifies the gross motor function of children with cerebral palsy. It is the gold standard for standardizing communication among orthopaedic surgeons, neurologists, and physical therapists.
- Level I: Walks without limitations; performs advanced gross motor skills (running, jumping) but with slightly decreased speed, balance, and coordination.
- Level II: Walks independently without assistive devices but has limitations walking outdoors and in the community; struggles with running and jumping.
- Level III: Walks using hand-held mobility devices (crutches, walkers) in most indoor settings; utilizes a wheelchair for long community distances.
- Level IV: Self-mobility is severely limited. Has the ability to stand for transfers but relies on wheeled mobility (often motorized or pushed by a caregiver) in most settings.
- Level V: Lacks antigravity head and trunk control. Cannot sit independently. Totally dependent on caregivers for all aspects of mobility and daily care.
PROGNOSTIC FACTORS FOR AMBULATION
Predicting a child's ultimate ambulatory potential is one of the most critical aspects of early orthopaedic evaluation, as it directly dictates the aggressiveness and timing of surgical interventions. Extensive research has identified reliable prognostic indicators.
Historical and Clinical Predictors
- Paine's Observations: Paine noted that the presence of obligate tonic neck reflexes is fundamentally incompatible with independent standing balance and the reciprocal lower extremity movements required for walking. He established that independent sitting by age 2 is a strong predictor of future ambulation. Approximately 50% of children who sit independently between ages 2 and 4 will eventually walk. If a child cannot sit independently by age 4, independent ambulation is highly unlikely. Furthermore, if a child has not achieved walking by age 8 (assuming they are not limited by severe, correctable contractures), they will likely never walk.
- Molnar and Gordon: Their research refined Paine's criteria, suggesting that while sitting before age 2 is not a guaranteed predictor of walking, the inability to sit independently by age 4 is a definitive predictor of non-ambulation.
Bleck’s Scoring System
Bleck developed a highly reliable prognostic scoring system based on the presence of primitive reflexes and the absence of mature postural reactions.
* Scoring: The child receives 1 point for any abnormal primitive reflex that persists, and 1 point for any mature protective reflex (like the parachute reaction) that is absent.
* Prognosis:
* Score of 0 = Good prognosis for walking.
* Score of 1 = Guarded prognosis.
* Score of ≥ 2 = Poor prognosis for walking.
Bleck identified five specific Poor Prognostic Signs for ambulation:
1. An imposable Asymmetrical Tonic Neck Reflex (ATNR).
2. A persistent Moro reflex.
3. A strong extensor thrust on vertical suspension.
4. A persistent neck-righting reflex.
5. Absence of a normal parachute reaction after 11 months of age.
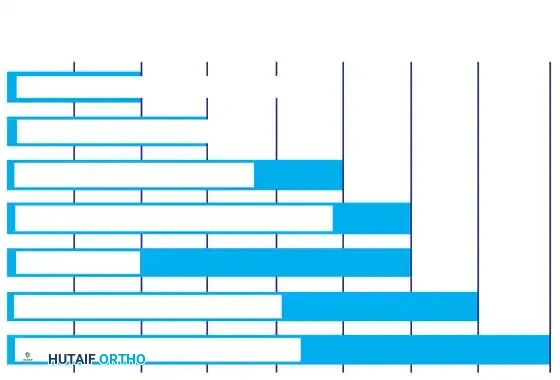
Figure 30-4: Incidence of Pathological Reflexes in Non-Ambulatory Children
This chart illustrates the prevalence of various pathological reflexes in children with cerebral palsy who have failed to ambulate by 8 years of age. The persistence of these specific primitive reflexes correlates directly with extensive cerebral damage and a uniformly poor prognosis for independent ambulation, self-care, and activities of daily living (ADLs).
GAIT ANALYSIS IN SURGICAL PLANNING
The orthopaedic management of the ambulatory child with cerebral palsy (GMFCS Levels I-III) relies heavily on accurate gait analysis. The goal of surgery is to improve the biomechanics of gait, reduce energy expenditure, and prevent joint degeneration.
Observational Gait Analysis (OGA)
Before the advent of computerized laboratories, careful clinical observation was the sole method of diagnosing gait deviations. It remains an essential, foundational skill. OGA requires repeatedly observing the child walking from the coronal (front/back) and sagittal (sides) planes. The surgeon must systematically evaluate the pelvis, hip, knee, ankle, and foot, noting stride length, cadence, rotational alignment, trunk sway, and side-to-side asymmetries.
Pitfall: Krebs et al. demonstrated that while intraobserver reliability in OGA is acceptable, interobserver reliability is poor. The human eye cannot accurately process the simultaneous, multi-planar, high-speed events occurring across multiple joints during the gait cycle.
Quantitative Gait Analysis (QGA)
Modern computerized gait analysis provides objective, three-dimensional data that is critical for planning Single-Event Multilevel Surgery (SEMLS). QGA consists of four primary components:
1. Kinematics: High-speed motion capture cameras track retroreflective markers placed on specific skeletal landmarks. This generates waveforms representing the exact joint angles in three dimensions throughout the gait cycle.
2. Kinetics: Force platforms embedded in the floor measure ground reaction forces. Combined with kinematic data, this calculates joint moments and powers (identifying where the patient is generating or absorbing energy).
3. Dynamic Electromyography (EMG): Surface or fine-wire electrodes document the precise timing of muscle activation. This differentiates between muscles firing in a normal physiological pattern versus those firing out of phase (e.g., continuous rectus femoris firing during swing phase, causing a stiff-knee gait).
4. Pedobarography and Energetics: Foot pressure mapping identifies abnormal weight-bearing patterns (e.g., equinovarus foot strike). Oxygen consumption measurements quantify the physiological cost index (energy efficiency) of the child's gait.
Impact of QGA on Surgical Decision Making
The integration of QGA into orthopaedic practice has revolutionized surgical planning.
* DeLuca et al. reviewed 91 patients with CP. When experienced surgeons were provided with QGA data after making initial recommendations based solely on clinical exams, their surgical plans changed 52% of the time. QGA led to more recommendations for gastrocnemius-soleus lengthening and rectus femoris transfers, and fewer recommendations for hamstring lengthenings, psoas lengthenings, adductor tenotomies, and osteotomies.
* Skaggs et al. noted that while QGA data is objective, its interpretation remains subjective, with significant institutional variations in treatment recommendations.
* Lee et al. demonstrated that patients whose surgical procedures aligned with QGA recommendations had significantly better postoperative outcomes compared to those who underwent surgery based on clinical examination alone.
* Kay et al. showed that postoperative QGA altered ongoing patient care in 84% of cases, guiding bracing (AFO) modifications and targeted physical therapy protocols.
TRANSLATING DIAGNOSIS TO SURGICAL INTERVENTION
To optimize outcomes, Davids et al. proposed a rigorous Five-Step Paradigm for clinical decision-making:
1. Clinical History
2. Physical Examination
3. Diagnostic Imaging
4. Quantitative Gait Analysis
5. Examination Under Anesthesia (EUA)
Examination Under Anesthesia (EUA)
EUA is the critical bridge between diagnosis and surgical execution. In the awake patient, it is often impossible to differentiate between dynamic spasticity and fixed myostatic contracture. Under general anesthesia, spasticity is abolished. Any residual limitation in joint range of motion represents a true, fixed contracture requiring surgical lengthening.
Common Surgical Approaches Based on Diagnostic Findings
1. Equinus Gait (Ankle Plantarflexion)
* Indication: True contracture of the gastroc-soleus complex confirmed by the Silfverskiöld test under anesthesia.
* Biomechanics: Premature heel rise, knee hyperextension (recurvatum) in stance phase.
* Surgical Approach: If the contracture is isolated to the gastrocnemius (ankle dorsiflexes with knee flexed but not extended), a Gastrocnemius Recession (Baumann or Strayer procedure) is performed. If both the gastrocnemius and soleus are contracted, a Tendo-Achilles Lengthening (TAL) is indicated.
* Positioning: Supine or prone depending on concurrent procedures.
2. Stiff-Knee Gait
* Indication: Decreased peak knee flexion during swing phase, causing foot drag or circumduction. Confirmed by continuous rectus femoris firing on dynamic EMG.
* Surgical Approach: Rectus Femoris Transfer. The distal tendon of the rectus femoris is detached from the patella and transferred posteriorly to the semitendinosus or sartorius. This converts the rectus from a knee extensor that impedes swing phase into a knee flexor.
3. Crouch Gait
* Indication: Excessive hip and knee flexion with ankle dorsiflexion during stance. Often iatrogenic from previous over-lengthening of the Achilles tendon combined with unaddressed hamstring/psoas contractures.
* Biomechanics: Massive increase in patellofemoral joint reaction forces and severe energy inefficiency.
* Surgical Approach: Requires complex SEMLS. May include hamstring lengthening, distal femoral extension osteotomy (DFEO), and patellar tendon advancement (PTA) to restore the extensor mechanism lever arm.
Postoperative Protocol
Following multi-level orthopaedic surgery for cerebral palsy, patients are typically immobilized in short-leg or long-leg casts for 3 to 6 weeks, depending on the inclusion of osteotomies. Upon cast removal, patients transition immediately into custom-molded Ankle-Foot Orthoses (AFOs) to protect the surgical lengthenings and prevent recurrence of deformity. Intensive, daily physical therapy is mandatory to retrain motor patterns, rebuild strength, and maximize the functional gains achieved through surgical intervention.
You Might Also Like