Comprehensive Introduction and Patho-Epidemiology
The management of diabetic foot complications represents one of the most challenging, multifaceted, and resource-intensive domains within modern orthopedic surgery. Care for diabetic foot ulcers and their associated sequelae, including deep space infections and lower extremity amputations, is estimated to cost the United States healthcare system well over 10 billion dollars annually. Beyond the staggering economic burden, diabetic foot ulcers exert a profound, devastating impact on patient quality of life. Clinical outcome scores for patients with unhealed ulcers are significantly lower than those with healed ulcers, and both cohorts score substantially lower than the age-matched general population. The presence of a diabetic foot ulcer must be viewed as a critical sentinel event; it is not merely a localized cutaneous wound but a glaring marker of end-stage systemic disease severity. Epidemiological data demonstrates that the development of a diabetic foot ulcer carries a five-year mortality rate approaching 50%, a figure that eclipses the mortality rates of several aggressive malignancies, including breast, prostate, and colon cancer.
The pathophysiological cascade leading to diabetic foot ulceration is rarely the result of a single isolated pathology. Rather, it is the devastating culmination of a triad of peripheral neuropathy, biomechanical deformity, and peripheral arterial disease (PAD). Neuropathy in the diabetic patient is insidious and affects the sensory, motor, and autonomic nervous systems in a progressive, length-dependent manner. Sensory neuropathy results in the loss of protective sensation (LOPS). Because these patients are unable to perceive repetitive microtrauma, thermal injury, or undue focal pressure, the skin is placed at severe risk of mechanical breakdown. Motor neuropathy leads to the denervation of the intrinsic foot musculature, creating an "intrinsic-minus" foot. This muscular imbalance results in the classic claw toe and hammer toe deformities, driving the metatarsal heads plantarly and rendering them, along with the dorsal proximal interphalangeal (PIP) joints, highly vulnerable to pressure necrosis.

Fixed flexion deformities of the interphalangeal joint of the hallux and proximal interphalangeal joint of the second toe. The rigid nature of these deformities exponentially increases focal plantar pressures.
Autonomic neuropathy further exacerbates the vulnerability of the diabetic foot. The loss of sympathetic tone leads to an autosympathectomy, resulting in dry, anhidrotic skin that is highly prone to hyperkeratosis and fissuring. These fissures provide a direct portal of entry for opportunistic bacterial pathogens. Furthermore, autonomic dysfunction causes arteriovenous shunting, which bypasses the nutrient capillary beds and deprives the dermis and epidermis of essential oxygen and metabolites, even in the presence of palpable pedal pulses.
Compounding these neurological deficits is the high prevalence of peripheral vascular disease and altered cellular healing mechanisms. Diabetic PAD typically affects the infrapopliteal vessels (the anterior tibial, posterior tibial, and peroneal arteries) while paradoxically sparing the pedal vessels (dorsalis pedis and plantar arteries). This specific pattern of distal ischemia is distinct from the proximal atherosclerotic disease seen in non-diabetic cohorts. Additionally, diabetic patients suffer from profoundly altered immune function and delayed bone healing. Hyperglycemia induces defects in leukocyte chemotaxis, adherence, phagocytosis, and intracellular bactericidal killing, leaving these patients highly susceptible to rapidly spreading infections. Diabetics face an 80% increased risk of cellulitis, a fourfold increased risk of osteomyelitis, and double the risk of systemic sepsis compared to normoglycemic individuals.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the altered surgical anatomy and biomechanics of the diabetic foot is essential for both prophylactic intervention and definitive reconstruction. The foot is a complex biomechanical structure designed to absorb shock during heel strike and act as a rigid lever during the propulsive push-off phase of gait. In the diabetic foot, this delicate balance is destroyed. The denervation of the lumbricals and interossei muscles leads to the overpowering of the intrinsic musculature by the extrinsic flexors and extensors. The extensor digitorum longus hyperextends the metatarsophalangeal (MTP) joints, while the flexor digitorum longus and brevis flex the PIP and distal interphalangeal (DIP) joints. This intrinsic-minus posture forces the metatarsal heads to bear a disproportionate amount of weight during the stance phase, leading to the formation of dense, hypertrophic calluses that eventually break down into deep cavitary ulcers.
Equinus contracture is arguably the most critical biomechanical fault in the diabetic foot. A tight Achilles tendon or gastrocnemius complex severely limits ankle dorsiflexion. During the midstance and terminal stance phases of gait, the inability of the tibia to translate anteriorly over the talus forces the foot to compensate by prematurely lifting the heel, thereby exponentially increasing peak plantar pressures across the forefoot. Furthermore, chronic hyperglycemia induces structural, microscopic changes within the Achilles tendon itself. Non-enzymatic glycosylation of Type I collagen leads to the disorganization of tendon fibrils, the formation of advanced glycation end-product (AGE) cross-linking, and intratendinous calcification. These histologic changes, which are highly prevalent in older diabetic patients, explain the profound stiffness and loss of viscoelasticity in the gastrocsoleus complex.

Evaluating protective sensation with the 5.07 Semmes-Weinstein monofilament. The filament should be applied perpendicular to the skin until it buckles.
Vascular anatomy in the diabetic foot must be evaluated through the lens of the angiosome concept, which divides the foot and ankle into distinct three-dimensional blocks of tissue fed by specific source arteries. The posterior tibial artery supplies the plantar heel, the plantar midfoot, and the plantar forefoot via its calcaneal, medial plantar, and lateral plantar branches. The anterior tibial artery (continuing as the dorsalis pedis) supplies the anterior ankle and the dorsum of the foot. The peroneal artery supplies the lateral heel and lateral ankle. In the setting of diabetic microvascular and macrovascular disease, the choke vessels (collaterals) between these angiosomes frequently fail. Therefore, when planning surgical incisions or amputations, the surgeon must acutely aware of which angiosome is compromised and tailor the approach to preserve the most robust vascular supply.
Because medial arterial calcification (Mönckeberg's sclerosis) renders the tibial arteries incompressible, standard Ankle-Brachial Index (ABI) measurements are frequently falsely elevated (>1.3) and clinically misleading. Therefore, Toe-Brachial Index (TBI) and toe systolic pressures using photoplethysmography (PPG) are mandatory for accurate assessment. The digital arteries are typically spared from medial calcinosis. A toe pressure greater than 40 mm Hg is generally required for predictable wound healing following a minor amputation or debridement, while pressures below 30 mm Hg indicate severe ischemia requiring urgent vascular surgery consultation for revascularization prior to any definitive orthopedic reconstruction.
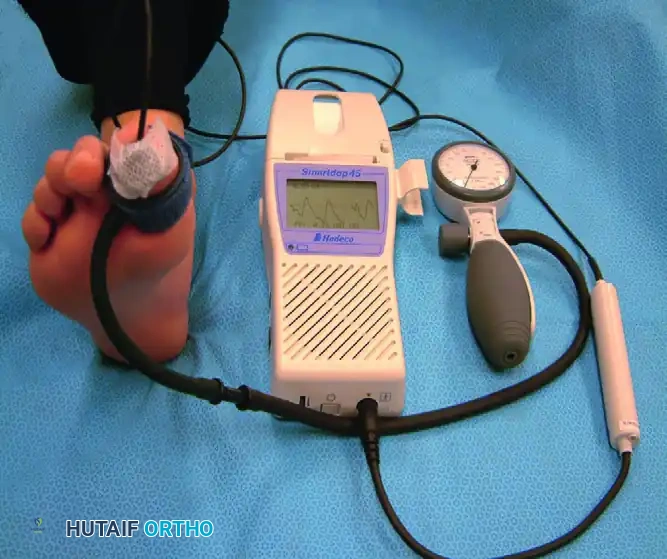
Measurement of toe systolic pressure with a manual PPG unit. A toe pressure >40 mm Hg is generally required for predictable wound healing.
Exhaustive Indications and Contraindications
The decision-making process regarding conservative offloading versus surgical intervention in the diabetic foot is highly nuanced. Accurate classification of the ulcer guides treatment and establishes a reliable prognosis. The Wagner Classification system remains a foundational tool in orthopedic practice, grading ulcers from Grade 0 (pre-ulcerative lesion) to Grade 5 (extensive gangrene involving the entire foot). However, the University of Texas (UT) San Antonio classification system is an excellent and necessary adjunct, as it incorporates ischemia and infection into a matrix grid, correlating more closely with prolonged healing times and the ultimate risk of major limb amputation.

Superficial (Wagner Grade 1) ulcer. The dermis is breached, but deep structures are not exposed.
Surgical indications are broadly categorized into urgent/emergent interventions for acute infection, and elective/prophylactic procedures for deformity correction and ulcer prevention. Urgent surgical indications include the presence of necrotizing fasciitis, gas gangrene, deep space abscesses, and wet gangrene. In these scenarios, the phrase "time is tissue" is highly applicable; delayed debridement exponentially increases the risk of systemic sepsis and major proximal limb amputation. Elective indications include rigid deformities causing recurrent ulceration despite maximal pedorthic offloading, chronic osteomyelitis that has failed culture-directed suppressive antibiotic therapy, and severe equinus contractures driving forefoot ulceration.

Deep (Wagner Grade 2) ulcer with exposed tendon and joint capsule. Immediate offloading and infection surveillance are required.
Contraindications to surgical intervention are equally critical to recognize. Operating on an ischemic limb without prior vascular optimization is an absolute contraindication, as surgical incisions will inevitably fail to heal, converting a stable, dry eschar into an active, limb-threatening infection. Similarly, elective prophylactic surgery should be deferred in patients with profound malnutrition (albumin < 3.0 g/dL), uncontrolled severe hyperglycemia (HbA1c > 10%), or untreated medical comorbidities that preclude safe anesthesia.

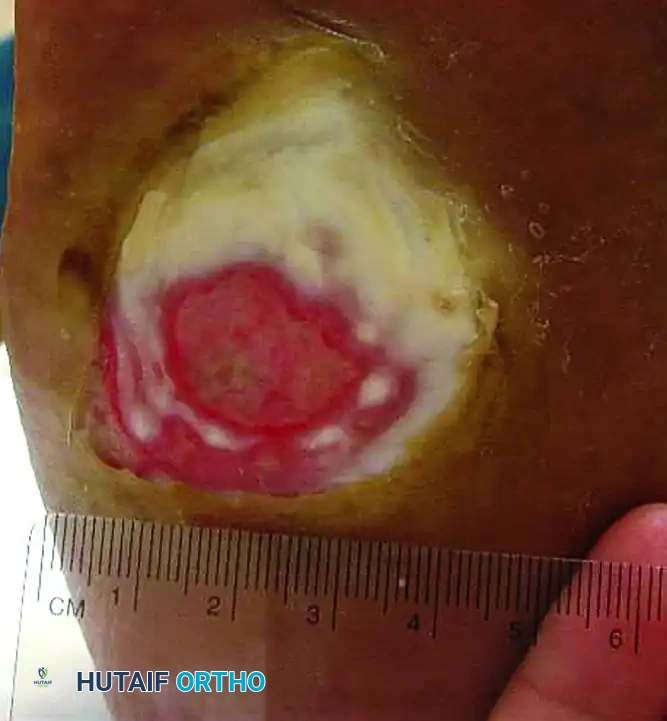
Wagner Grade 3 ulcer with underlying osteomyelitis. Note the deep tissue destruction and purulent exudate.
| Surgical Intervention | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Emergent I&D / Radical Debridement | Necrotizing fasciitis, deep space abscess, wet gangrene, systemic sepsis secondary to foot infection. | None (Life-saving procedure). | Unstable hemodynamics requiring resuscitation prior to OR. |
| Transmetatarsal Amputation (TMA) | Forefoot gangrene, multiple ray osteomyelitis, unstageable forefoot necrosis with viable midfoot soft tissue. | Inadequate plantar flap perfusion, uncorrectable proximal ischemia, midfoot/hindfoot infection. | Severe malnutrition, active systemic bacteremia (delay until cleared). |
| Achilles Tendon Lengthening (TAL) | Recalcitrant forefoot ulceration, severe equinus contracture (>10 deg plantarflexion), prophylactic offloading. | Active posterior heel ulceration, severe midfoot Charcot neuroarthropathy (risk of rocker-bottom collapse). | Patient inability to comply with post-operative casting. |
| Partial Calcanectomy | Chronic calcaneal osteomyelitis, posterior heel ulceration failing conservative care. | Complete calcaneal destruction, inadequate dorsal/plantar soft tissue coverage, severe PAD. | Non-ambulatory status (consider primary BKA if comfort is the goal). |
| Major Amputation (BKA / AKA) | Unreconstructable vascular disease, overwhelming sepsis, non-salvageable foot, chronic intractable pain. | Patient refusal, viable and functional limb salvage options remain. | Severe contralateral limb disease (requires careful prosthetic planning). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the bedrock of successful diabetic foot surgery. The initial phase of planning must involve a multidisciplinary team, typically including an orthopedic surgeon, vascular surgeon, endocrinologist, infectious disease specialist, and a certified pedorthotist. Optimization of the host is paramount. Glycemic control must be aggressively managed, targeting perioperative blood glucose levels between 140 and 180 mg/dL. Strict glycemic control has been shown to improve leukocyte function, enhance collagen synthesis, and significantly reduce the rates of post-operative surgical site infections. Nutritional status must be quantified via serum albumin, prealbumin, and total lymphocyte counts; deficiencies must be corrected with enteral or parenteral supplementation to provide the metabolic substrates required for wound healing.
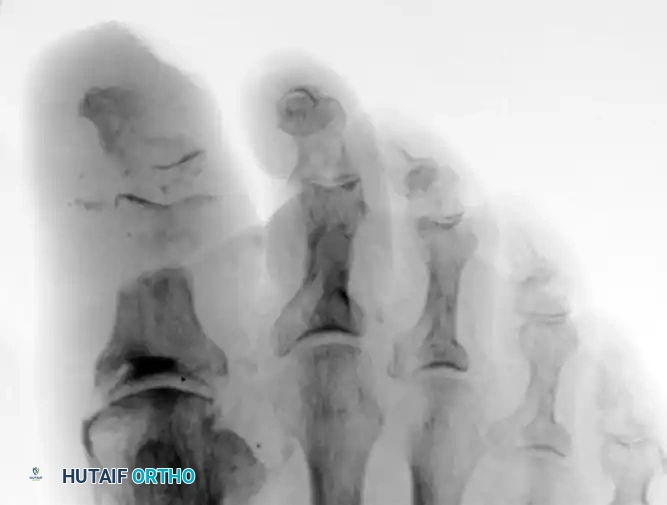
Advanced imaging is crucial for defining the extent of bony and soft tissue involvement. While standard weight-bearing radiographs are the initial modality of choice to assess for gross deformity, gas in the soft tissues, and advanced osteomyelitis, they lack sensitivity for early bone infection. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the gold standard for diagnosing osteomyelitis, delineating deep space abscesses, and evaluating the integrity of the tendinous structures. The surgeon must meticulously review the MRI to template the level of bone resection, ensuring that all infected osseous margins are excised while preserving the maximal functional length of the foot.

Radiograph demonstrating severe osteomyelitis and bone destruction of the metatarsophalangeal joints, necessitating surgical resection.
Patient positioning and operating room setup require careful consideration of the patient's compromised integument and vascular status. The patient is typically positioned supine on a radiolucent operating table to facilitate intraoperative fluoroscopy. All bony prominences, particularly the contralateral heel and sacrum, must be meticulously padded to prevent iatrogenic pressure ulcers during prolonged procedures. The use of a pneumatic tourniquet is highly controversial in the diabetic population with concurrent PAD. If a tourniquet is deemed absolutely necessary for visualization during a complex reconstruction, it should be applied over generous padding, inflated to the lowest effective pressure (typically 100 mm Hg above systolic pressure), and utilized for the shortest duration possible to minimize ischemic-reperfusion injury to already compromised tissues. In cases of severe PAD or calcified vessels, tourniquet use is strictly contraindicated, and hemostasis must be achieved via precise electrocautery and topical hemostatic agents.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention in the diabetic foot ranges from percutaneous prophylactic releases to radical amputations. Regardless of the procedure, tissue handling must be exceptionally atraumatic. Forceps should be used sparingly on skin edges, and self-retaining retractors must be placed with caution to avoid ischemic necrosis of the wound margins.
Transmetatarsal Amputation (TMA)
The transmetatarsal amputation is a workhorse procedure for extensive forefoot osteomyelitis or gangrene. The goal is to create a durable, balanced, and sensate stump utilizing a robust plantar flap.
1. Incision and Flap Design: A fish-mouth incision is utilized. The dorsal incision is made straight across the metatarsals at the planned level of bone resection. The plantar incision extends distally to the metatarsal necks, creating a long, thick plantar flap that will fold dorsally to cover the distal bony stump.
2. Dissection: The dorsal incision is carried down through the extensor tendons, which are placed under tension and sharply transected to allow them to retract proximally. The plantar flap is elevated full-thickness, staying extra-periosteal to preserve the critical blood supply from the medial and lateral plantar arteries.
3. Bone Resection: An oscillating saw is used to transect the metatarsals. The cuts must be made with a 10 to 15-degree plantar declination to prevent prominent distal bony spikes from impinging on the plantar flap during weight-bearing. The metatarsals should be cut in a gentle cascade, with the first metatarsal being the longest and the fifth being the shortest, mimicking the natural parabola of the foot. A rongeur and rasp are used to meticulously smooth all bony edges.
4. Nerve Handling: The digital nerves are identified, placed under gentle traction, and transected sharply so they retract deep into the proximal soft tissue, minimizing the risk of painful terminal neuroma formation.
5. Closure: The wound is copiously irrigated with sterile saline. The thick plantar flap is rotated dorsally. Closure must be entirely tension-free. If tension is present, further bony shortening is mandatory. Deep tissues are approximated with absorbable suture, and the skin is closed with non-absorbable monofilament using a vertical mattress technique to evert the edges and preserve dermal perfusion.
Achilles Tendon Lengthening (TAL)
For recalcitrant forefoot ulcers driven by equinus contracture, a percutaneous Achilles tendon lengthening is a highly effective, minimally invasive adjunct.
1. Positioning and Prep: The patient can be positioned prone or supine with the leg externally rotated. The procedure is often performed under local anesthesia.
2. The Hoke Triple Hemisection Technique: Three percutaneous stab incisions are made over the Achilles tendon. The first is placed medially, approximately 1-2 cm proximal to the calcaneal insertion. The second is placed laterally, 2-3 cm proximal to the first. The third is placed medially, 2-3 cm proximal to the second.
3. Tendon Release: A #11 blade is inserted blindly but carefully into the center of the tendon at each level. The blade is turned to transect the medial half of the tendon at the distal and proximal incisions, and the lateral half at the middle incision.
4. Lengthening: The ankle is then forcibly dorsiflexed by the surgeon. The remaining intact tendon fibers will slide and lengthen, yielding a palpable "give." The goal is to achieve 5 to 10 degrees of ankle dorsiflexion past neutral.
5. Post-Operative Care: The incisions are closed with single sutures or steri-strips, and the patient is immediately placed in a rigid cast or CAM boot locked at 90 degrees to allow the tendon to heal in its newly lengthened position.
Metatarsal Head Resection
Isolated metatarsal head resection is indicated for chronic plantar ulcers underlying a specific prominent metatarsal head, often complicated by localized osteomyelitis.
1. Approach: A dorsal longitudinal incision is made centered over the affected metatarsophalangeal joint. The extensor tendon is retracted or Z-lengthened.
2. Capsulotomy and Resection: A dorsal capsulotomy is performed, exposing the metatarsal head. Collateral ligaments are released. An oscillating saw is used to resect the metatarsal head at the surgical neck, angling the cut dorsal-distal to plantar-proximal to ensure no plantar prominence remains.
3. Debridement: The underlying ulcer is aggressively debrided from the inside out (via the dorsal incision) to remove all fibrotic and infected tissue, creating a clean soft-tissue envelope.
4. Closure: The wound is flushed, and the dorsal incision is closed. The plantar ulcer is typically left open to heal by secondary intention or managed with negative pressure wound therapy.
Complications, Incidence Rates, and Salvage Management
Surgical intervention in the diabetic foot is fraught with potential complications. The compromised host biology, poor microvascular perfusion, and profound immunosuppression create an environment where wound healing is unpredictable and infection recurrence is common. Surgeons must counsel patients extensively pre-operatively regarding the high likelihood of complications, the potential need for multiple staged procedures, and the ever-present risk of major proximal amputation.
Wound dehiscence and failure of surgical flaps are among the most frequent complications, occurring in 20% to 30% of cases, particularly following transmetatarsal or midfoot amputations. This is typically the result of unrecognized proximal ischemia, excessive tension on the suture line, or premature weight-bearing by a non-compliant, neuropathic patient. If dehiscence occurs, immediate cessation of weight-bearing is required. The wound must be assessed for deep infection; if clean, it can often be salvaged with aggressive Negative Pressure Wound Therapy (NPWT) and eventual split-thickness skin grafting. If necrotic tissue is present, return to the operating room for further proximal bone resection is necessary.
Recurrence of osteomyelitis or deep space infection occurs in approximately 15% to 20% of cases. This is often due to retained microscopic foci of infected bone, inadequate duration of post-operative antibiotic therapy, or the development of a new adjacent ulcer due to altered post-operative biomechanics (transfer lesions). Salvage management requires a multidisciplinary approach: repeat MRI to map the extent of recurrence, aggressive re-debridement (often requiring conversion to a higher-level amputation, such as a ray resection to a TMA, or a TMA to a Syme amputation), and prolonged course (6 weeks) of culture-directed intravenous antibiotics managed by an infectious disease specialist.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management & Prevention |
|---|---|---|---|
| Wound Dehiscence / Flap Necrosis | 20% - 30% | Undiagnosed PAD, closure under tension, premature weight-bearing, hematoma formation. | NPWT, strict offloading, hyperbaric oxygen therapy (HBOT). Prevent via meticulous vascular workup and tension-free closures. |
| Recurrent Osteomyelitis | 15% - 20% | Retained infected bone, inadequate antibiotic duration, transfer ulceration. | Repeat surgical debridement, proximal amputation revision, 6-week IV antibiotics. Prevent via clean bone margins (pathology confirmed). |
| Transfer Ulceration | 30% - 40% | Altered biomechanics post-amputation (e.g., adjacent metatarsal overload after ray resection). | Custom orthotics, rocker-bottom shoes, prophylactic tendon balancing (TAL). Prevent via biomechanically sound reconstructive planning. |
| Charcot Neuroarthropathy Triggering | 5% - 10% | Surgical trauma and hyperemia in a severely neuropathic foot triggering the acute inflammatory phase. | Immediate immobilization in Total Contact Cast (TCC), prolonged non-weight-bearing. Prevent via gentle tissue handling and post-op surveillance. |
| Progression to Major Amputation (BKA/AKA) | 10% - 15% | Overwhelming sepsis, uncorrectable vascular failure, progressive gangrene. | Formal proximal amputation optimizing the stump for prosthetic fitting. Ensure multidisciplinary optimization prior to initial limb salvage attempts. |
Phased Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical to the ultimate success of limb salvage as the surgical intervention itself. A technically perfect operation will rapidly fail if the post-operative offloading and mobilization protocols are inadequate. Because diabetic wound healing is significantly delayed, timelines for immobilization are substantially longer than those for non-diabetic orthopedic procedures.
Phase I: Immediate Post-Operative (Weeks 0-4)
Following debridement, partial amputation, or structural reconstruction, the foot is typically placed in a bulky, non-compressive Jones dressing with a posterior plaster splint to lock the ankle in neutral. If the wound is left open or closed with high risk of dehiscence, a Negative Pressure Wound Therapy (NPWT) device is applied in the operating room. Strict, absolute non-weight-bearing (NWB) is enforced. Patients are instructed on the use of crutches, walkers, or knee-scooters. Deep venous thrombosis (DVT) prophylaxis is initiated, and glycemic control is tightly monitored. Sutures are left in place for a minimum of 3 to 4 weeks, as premature removal frequently leads to catastrophic wound dehiscence.
Phase II: Transition to Offloading (Weeks 4-10)
Once the soft tissue envelope is stable, the surgical incisions are fully epithelialized, and sutures are removed, the patient is transitioned to aggressive mechanical offloading. Total contact casting (TCC) remains the absolute gold standard for offloading plantar wounds and protecting recent surgical sites. TCC works by rigidly locking the ankle, eliminating the propulsive push-off phase of gait, and transferring ground reaction forces from the plantar surface of the foot directly to the conical shape of the lower leg (shank).
Application of a total contact cast. Meticulous padding of bony prominences is essential to prevent iatrogenic ulceration.
For patients who cannot maintain strict non-weight-bearing status, modifications to the TCC can be made. The addition of a metal stirrup extending beyond the foot-plate transmits ground reaction forces directly to the cast walls, bypassing the plantar surface entirely.
Total contact cast modified with a metal stirrup to further offload the plantar surface in ambulatory patients.
If TCC is contraindicated (e.g., highly exudative wounds requiring daily dressing changes, severe PAD, or active infection), Removable Cast Walkers (CAM boots) are utilized. While biomechanically effective, clinical success with CAM boots is heavily dependent on patient adherence. Wrapping the boot with cohesive bandages or fiberglass (rendering it an "irremovable" cast walker) significantly improves healing rates by enforcing compliance.

Removable diabetic boot. While effective for offloading, clinical success is heavily dependent on patient adherence.

A plantar ulcer successfully healed after 2 months of strict total contact casting.
Phase III: Long-Term Pedorthic Management (Lifelong)
Once the foot is fully healed and stable, the patient enters the lifelong maintenance phase. The patient is transitioned to a Charcot Restraint Orthotic Walker (CROW) boot or definitive custom diabetic footwear. Patients must be fitted by a certified pedorthotist with custom-molded, multi-density plastazote orthotics to accommodate residual deformities and distribute plantar pressures evenly. Extra-depth shoes with rigid rocker-bottom soles are mandatory. The rocker-bottom sole simulates ankle dorsiflexion and MTP extension, effectively bypassing the foot's intrinsic joints and drastically reducing plantar peak pressures during the terminal stance phase of gait. Routine surveillance by the orthopedic and podiatric team every 3 to 6 months is required indefinitely.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of the diabetic foot is heavily guided by evidence-based medicine and consensus guidelines generated by international expert panels. Familiarity with this landmark literature is essential for the practicing orthopedic surgeon.
The International Working Group on the Diabetic Foot (IWGDF) publishes regularly updated, comprehensive guidelines that serve as the global standard of care. Their guidelines emphasize the absolute necessity of non-invasive vascular testing for all diabetic foot ulcers, the superiority of Total Contact Casting for plantar forefoot ulcers, and the requirement for deep tissue cultures (rather than superficial swabs) to direct antibiotic therapy for osteomyelitis. The IWGDF strictly recommends against the routine use of topical antimicrobials for uninfected ulcers, emphasizing mechanical offloading and sharp debridement as the primary drivers of healing.
Landmark literature regarding offloading is dominated by the work of Armstrong and Lavery. Their randomized controlled trials definitively established that irremovable offloading devices (TCC or instant total contact casts) yield significantly higher healing rates (nearly 90% at 12 weeks) compared to standard removable cast walkers (approximately 65%), primarily due to the enforcement of patient compliance. Their studies underscore the concept that "it's not what you put on the wound, it's what you take off of it."
The management of diabetic foot infections is governed by the guidelines of the Infectious Diseases Society of America (IDSA). The IDSA guidelines stratify infections into mild, moderate, and severe categories, dictating the route (oral vs. intravenous) and spectrum of empiric antibiotic therapy. A critical tenet of the IDSA guidelines is that osteomyelitis in the diabetic foot does not always require radical amputation; selected cases of forefoot osteomyelitis without systemic toxicity or severe ischemia can be successfully managed with conservative surgical debridement (e.g., isolated bone resection) combined with a 6-week course of culture-directed antibiotics.
Finally, the Eurodiale study, a massive prospective cohort study across multiple European centers, highlighted the profound impact of multidisciplinary
