DEGENERATIVE SPONDYLOLISTHESIS AND SCOLIOSIS: A CONTINUUM OF UNSTABLE STENOSIS
Junghanns first described degenerative spondylolisthesis in 1930, meticulously separating the pathology from isthmic spondylolisthesis. He originally classified this entity as “pseudospondylolisthesis,” a term later refined by Newman to degenerative spondylolisthesis due to the ubiquitous arthritic changes noted on radiographs. Degenerative spondylolisthesis is inextricably linked with spinal stenosis, which is typically the primary catalyst for symptom exacerbation and must be the focal point of clinical consideration.
Hanley elegantly conceptualized this pathology as “unstable stenosis,” which manifests in two distinct but related forms:
* Unisegmental Unstable Stenosis: Manifested primarily by degenerative spondylolisthesis.
* Multisegmental Unstable Stenosis: Represented by degenerative lumbar scoliosis.
The treatment of either of these entities exists along a therapeutic continuum, necessitating a unified approach to decompression, stabilization, and deformity correction.
Incidence and Epidemiology
Degenerative spondylolisthesis is a pathology of the aging spine, occurring almost exclusively in patients older than 40 years. It is characterized by the anterior translation (forward slip) of one vertebra over another, typically measuring less than 33% of the vertebral body width (Meyerding Grade I or II).
- Anatomical Predilection: Deformity occurs at the L4-L5 level six times more frequently than at other lumbar levels, and four times more often above a sacralized L5 transitional vertebra. When other levels are involved, L3-L4 is affected more frequently than L5-S1.
- Demographics: Autopsy studies identify this disorder in approximately 4% of specimens, rising to 10% in women older than 60 years. Women are disproportionately affected, presenting four to six times more often than men.
- Hormonal and Systemic Factors: The female predominance is hypothesized to stem from inherent ligamentous laxity and distinct facet morphology. Furthermore, systemic factors play a role; diabetes is highly prevalent in this cohort. Imada et al. demonstrated that patients who underwent an oophorectomy had a threefold greater rate of degenerative spondylolisthesis. Immunohistochemical analyses reveal an upregulation of estrogen receptors in the facet cartilage of patients with degenerative instability, though the exact pathophysiological role of estrogen depletion remains a subject of ongoing research.
Degenerative scoliosis similarly develops in patients with previously straight spines after the age of 40. It typically affects the lumbar spine, presenting with associated lumbar hypolordosis, lateral olisthesis, and multisegmental spinal stenosis. Unlike idiopathic adolescent scoliosis, degenerative scoliosis affects men and women more equally (though women still comprise 60% to 70% of cases) and involves fewer spinal segments (typically two to five segments, compared to seven to eleven in idiopathic curves).
Clinical Pearl: Symptoms of spinal stenosis in degenerative scoliosis occur most frequently at the apex of the curve (both convexity and concavity). This is likely because severe, localized degenerative changes precede and drive the development of the scoliotic deformity.
ANATOMY AND BIOMECHANICS
The hallmark differentiator between degenerative and isthmic spondylolisthesis is the presence of an intact pars interarticularis in the degenerative form. Because the neural arch remains intact and translates anteriorly with the vertebral body, the spinal canal is progressively narrowed between the posterior aspect of the vertebral body below and the intact lamina/ligamentum flavum of the slipped vertebra above.
The true deformity in degenerative spondylolisthesis is rarely pure sagittal translation; it is a complex rotary deformity that distorts the thecal sac and exacerbates the clinical presentation of stenosis.
Pathoanatomical Theories of Instability
Two primary theories explain the genesis of degenerative spondylolisthesis:
1. The Sagittal Facet Theory: This theory posits a primary anatomical predisposition. Facets that are oriented more sagittally fail to resist anterior shear forces. Over time, this mechanical disadvantage leads to anterior translation. Boden et al. demonstrated that sagittal facet angles exceeding 45 degrees at L4-L5 predicted a 25-fold greater likelihood of developing degenerative spondylolisthesis.
2. The Disc Degeneration Theory: This theory suggests that the intervertebral disc narrows first. The loss of disc height leads to secondary overloading of the facet joints, resulting in accelerated osteoarthritis, capsular laxity, remodeling, and subsequent anterolisthesis.
Current consensus suggests a continuum where disc space narrowing increases facet loading, driving secondary arthritic changes. Regardless of the inciting event, the resulting cascade—facet arthritis, disc degeneration, and ligamentum flavum hypertrophy—culminates in symptomatic neurogenic claudication.
Biomechanics of Degenerative Scoliosis
In degenerative scoliosis, mechanical insufficiency of the lumbar spine leads to a progressive loss of lumbar lordosis (flatback syndrome). Curves are typically less than 60 degrees, but 81% of patients develop lateral olisthesis (rotary subluxation).
Osteoporosis is a critical biomechanical consideration. While not a direct cause of degenerative scoliosis, the older demographic is highly predisposed to diminished bone mineral density. This complicates surgical intervention, increasing the risk of compression fractures, pedicle screw pullout, and proximal junctional kyphosis (PJK).
NATURAL HISTORY
The natural history of degenerative spondylolisthesis is variable but often features a phenomenon known as "autostabilization." Matsunaga et al. followed 145 patients for a minimum of 10 years:
* Progressive slippage occurred in 34% of patients.
* In patients without further slip, progressive disc space narrowing was observed.
* Interestingly, low back pain often improved as the disc space collapsed, implying that osteophyte formation and disc desiccation eventually stabilize the hypermobile segment.
* While 76% of patients remained free of severe neurological deficits, 83% of those who developed neurological symptoms (claudication, vesicorectal dysfunction) deteriorated significantly, indicating a poor prognosis without surgical intervention.
For degenerative scoliosis, curves can progress at a rate of 1 to 6 degrees per year. Observation and nonoperative management (physical therapy, NSAIDs, epidural steroid injections) are warranted initially. However, operative intervention becomes necessary when patients develop progressive neurological deficits or intractable pain that fails conservative measures.
CLINICAL EVALUATION
A meticulous clinical evaluation is paramount to differentiate spinal pathology from peripheral vascular or neuropathic conditions.
- Symptomatology: Patients typically present with mechanical back pain, neurogenic claudication (68%), and radiculopathy (32%). Cauda equina syndrome is rare (3%).
- Degenerative Scoliosis Presentation: Neurogenic claudication is present in 71% to 90% of these patients. Unlike typical central stenosis, patients with degenerative scoliosis often do not obtain relief simply by bending forward. They frequently require upper extremity support (leaning heavily on a shopping cart or walker) or must assume a supine position to alleviate symptoms.
- Physical Examination: Motion is usually preserved, but patients actively guard against hyperextension, which exacerbates canal narrowing. Neurological deficits (motor weakness, sensory loss, reflex asymmetry) must be carefully documented.
- Vascular Assessment: Evaluation of distal pulses (dorsalis pedis, posterior tibial) is mandatory to rule out vascular claudication. Bilateral absence of Achilles reflexes may indicate underlying diabetic peripheral neuropathy.
Surgical Warning: Overlap of neurogenic and vascular claudication is common in the elderly. If pedal pulses are diminished, Ankle-Brachial Index (ABI) testing and vascular surgery consultation are required prior to any elective spine intervention.
DIAGNOSTIC IMAGING
Radiography
Standard radiographic imaging is the cornerstone of diagnosis.
* Standing AP and Lateral Views: Essential for evaluating the true extent of the deformity. Up to 15% of deformities spontaneously reduce when the patient is supine.

Preoperative standing lateral radiograph demonstrating a Grade I degenerative anterolisthesis of L4 on L5 with associated disc space collapse.
- Flexion-Extension Lateral Views: Utilized to assess dynamic instability. Instability is generally defined as >4 to 5 mm of dynamic translation or >10 to 15 degrees of angular change between flexion and extension.
- Coronal Assessment: The AP view will reveal degenerative scoliosis, lateral olisthesis, and the status of the transverse processes.

Preoperative AP radiograph illustrating a degenerative lumbar scoliosis with lateral olisthesis and asymmetric disc space collapse.
- Ferguson View: A 30-degree cephalad-angled AP view of the lumbosacral junction is critical for visualizing L5-S1 degenerative changes and assessing the size of the L5 transverse processes. Hypoplastic transverse processes should prompt the surgeon to consider interbody fusion, as the posterolateral bone mass will be insufficient for a robust fusion mass.
Advanced Imaging: MRI and CT Myelography
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating neural compression, assessing disc hydration (T2-weighted sequences), and identifying facet synovial cysts. Synovial cysts are a hallmark of microinstability and often necessitate a more aggressive foraminal decompression and concomitant fusion.
When MRI is contraindicated or obscured by severe deformity, CT Myelography is invaluable. It provides unparalleled visualization of bony anatomy, lateral recess stenosis caused by ligamentum flavum hypertrophy, and peduncular kinking of the nerve roots on the concavity of a scoliotic curve.
Clinical Pearl: Desiccation of the L5-S1 disc on MRI in a patient requiring an L4-L5 fusion should prompt careful consideration. Stopping a fusion construct adjacent to a severely degenerated disc significantly increases the risk of adjacent segment disease (ASD). Extension of the fusion to the sacrum may be warranted.
SURGICAL MANAGEMENT: STEP-BY-STEP MASTERCLASS
The primary goal of surgery is the adequate decompression of neural elements. However, decompression alone in the setting of degenerative spondylolisthesis or scoliosis often leads to progressive instability and iatrogenic deformity. Therefore, decompression with instrumented fusion is the gold standard for unstable stenosis.
Indications for Surgery
- Intractable neurogenic claudication or radiculopathy failing >3-6 months of conservative care.
- Progressive motor deficit or cauda equina syndrome (absolute indication).
- Documented dynamic instability on flexion-extension radiographs with correlating mechanical back pain.
- Progressive scoliotic deformity with coronal/sagittal imbalance.
Preoperative Planning and Positioning
- Anesthesia: General endotracheal anesthesia with neuromonitoring (SSEP and MEP) is highly recommended, especially during deformity correction.
- Positioning: The patient is placed prone on a radiolucent Jackson spinal table. The abdomen must hang completely free to decrease intra-abdominal pressure, thereby reducing epidural venous engorgement and intraoperative bleeding.
- Lordosis Preservation: The hips and knees are extended to maximize lumbar lordosis during instrumentation.
Surgical Approach and Decompression
- Incision and Exposure: A standard midline longitudinal incision is made. Subperiosteal dissection of the paraspinal musculature is performed laterally to the tips of the transverse processes at the levels to be fused.
- Crucial Step: Meticulous care must be taken to preserve the facet joint capsules at the adjacent, non-fused levels to prevent adjacent segment instability.
- Laminectomy and Facetectomy: A wide bilateral laminectomy is performed. The ligamentum flavum is excised using Kerrison rongeurs. A medial facetectomy is performed to decompress the lateral recess and traversing nerve roots.
- Foraminotomy: The neural foramina are decompressed along the course of the exiting nerve roots. In degenerative scoliosis, the concavity of the curve often requires aggressive foraminal decompression due to pedicle kinking.
Interbody Fusion (TLIF/PLIF)
To maximize fusion rates, restore disc height, and indirectly decompress the foramina, a Transforaminal Lumbar Interbody Fusion (TLIF) or Posterior Lumbar Interbody Fusion (PLIF) is frequently employed.
- Disc Preparation: The facet joint is completely resected on the more symptomatic side (TLIF approach). The annulus is incised, and a thorough complete discectomy is performed using pituitary rongeurs, curettes, and rasps. The cartilaginous endplates are meticulously prepped to bleeding subchondral bone.
- Grafting and Cage Insertion: The anterior third of the disc space is packed with autograft (local bone from the laminectomy) or allograft/biologics. An interbody cage of appropriate size and lordosis is then impacted into the disc space.
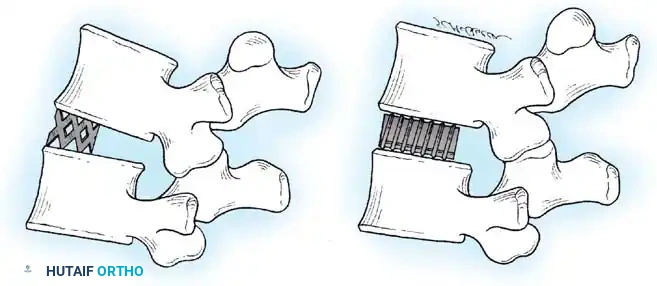
Schematic representation of an interbody fusion cage inserted into the prepared disc space, restoring foraminal height and providing anterior column support.
Instrumentation and Deformity Correction
- Pedicle Screw Placement: Under fluoroscopic or stereotactic navigation guidance, pedicle screws are inserted bilaterally. The entry point is the intersection of the pars interarticularis, the superior articular facet, and the transverse process.

Intraoperative/Postoperative lateral radiograph demonstrating the trajectory of pedicle screws stabilizing the spondylolisthesis.
- Rod Contouring and Reduction: Titanium or Cobalt-Chrome rods are contoured to the desired lumbar lordosis. In cases of spondylolisthesis, reduction of the slip can be achieved via the instrumentation, though partial reduction is often sufficient and safer for the nerve roots. In degenerative scoliosis, compression on the convexity and distraction on the concavity aids in coronal correction.
- Posterolateral Fusion: The transverse processes and lateral gutters are decorticated with a high-speed burr. Bone graft is meticulously laid over the decorticated surfaces to ensure a robust posterolateral fusion mass.
Postoperative Radiographic Assessment
Immediate postoperative radiographs are obtained to confirm the restoration of alignment, adequate decompression (indirectly via disc height restoration), and optimal hardware placement.

Postoperative lateral radiograph showing successful reduction of the anterolisthesis, restoration of disc height with an interbody cage, and solid posterior pedicle screw fixation.

Postoperative AP radiograph demonstrating the posterior construct, including pedicle screws and a cross-link (if utilized), ensuring rigid stabilization of the scoliotic and translated segments.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Rehabilitation
- Mobilization: Patients are mobilized on postoperative day 1 with physical therapy. Early ambulation is critical to prevent deep vein thrombosis (DVT) and pulmonary complications.
- Bracing: The use of a rigid Thoracolumbosacral Orthosis (TLSO) is surgeon-dependent but is often utilized in patients with poor bone quality or extensive multisegmental deformity corrections for 6 to 12 weeks.
- Restrictions: Bending, lifting (greater than 10 lbs), and twisting are restricted for the first 3 months until early fusion mass consolidation is visible on radiographs.
Complications
- Dural Tears: The dura in degenerative stenosis is often thin and adherent to the hypertrophied ligamentum flavum. Incidental durotomies must be repaired primarily with 4-0 or 5-0 non-absorbable suture and augmented with a dural sealant.
- Adjacent Segment Disease (ASD): A long-term complication where the segments adjacent to the fusion construct undergo accelerated degeneration due to altered biomechanical stress.
- Pseudarthrosis: Failure of fusion, more common in smokers, diabetics, and patients with osteoporosis. Meticulous endplate preparation and robust bone grafting techniques are the best prevention.
- Hardware Failure: Screw pullout or rod breakage, often secondary to pseudarthrosis or severe osteoporosis.
In conclusion, the surgical management of degenerative spondylolisthesis and scoliosis requires a profound understanding of spinal biomechanics, meticulous preoperative planning, and precise surgical execution. By adhering to these evidence-based principles, orthopedic surgeons can reliably decompress neural elements, restore spinal stability, and significantly improve the patient's quality of life.
📚 Medical References
- degenerative spondylolisthesis, Spine 29:1885, 2004.
- van Rens TJG, van Horn JR: Long-term results in lumbosacral interbody fusion for spondylolisthesis, Acta Orthop Scand 53:383, 1982.
- Vazquez-Seoane P, Yoo J, Zou D, et al: Interference screw fi xation of cervical grafts: a combined in vitro biomechanical and in vivo animal study, Spine 18:946, 1993.
- Wang JC, McDonough PW, Endow KK, et al: A comparison of fusion rates between single-level cervical corpectomy and twolevel discectomy and fusion, J Spinal Disord 14:222, 2001.
- Wang JC, McDonough PW, Kanim LE, et al: Increased fusion rates with cervical plating for two-level anterior cervical discectomy and fusion, Spine 25:41, 2000.
- Watkins MB: Posterolateral fusion in pseudarthrosis and posterior element defects of the lumbosacral spine, Clin Orthop Relat Res 35:80, 1964.
- White AA III, Hirsch C: An experimental study of the immediate load bearing capacity of some commonly used iliac bone grafts, Acta Orthop Scand 42:482, 1971.
- White AA III, Jupiter J, Southwick WO, et al: An experimental study of the immediate load bearing capacity of three surgical constructions for anterior spine fusions, Clin Orthop Relat Res 91:21, 1973.
- Whitecloud TS III, LaRocca H: Fibular strut graft in reconstructive surgery of the cervical spine, Spine 1:33, 1976.
- Whitehill R, Sirna EC, Young DC, et al: Late esophageal perforation from an autogenous bone graft: report of a case, J Bone Joint Surg 67A:644, 1985.
- Williams JL, Allen MB Jr, Harkess JW: Late results of cervical discectomy and interbody fusion: some factors infl uencing the results, J Bone Joint Surg 50A:277, 1968.
- Wiltse LL: Spondylolisthesis in children, Clin Orthop 21:156, 1961.
- Wiltse LL, Bateman JG, Hutchinson RH, et al: The paraspinal sacrospinalis-splitting approach to the lumbar spine, J Bone Joint Surg 50A:919, 1968.
- Wing KJ, Fisher CG, O’Connell JX, et al: Stopping nicotine exposure before surgery: the effect on spinal fusion in a rabbit model, Spine 25:30, 2000.
- Wozney JM, Rosen U, Celeste AJ, et al: Novel regulators of bone formation: molecular clones and activities, Science 242:1528, 1988.
- Young WF, Rosenwasser RH: An early comparative analysis of the use of fi bular allograft versus autologous iliac crest graft for interbody fusion after anterior cervical discectomy, Spine 18:1123, 1993.
- Zdeblick TA: A prospective randomized study of lumbar fusion: preliminary results, Spine 18:983, 1993.
- Zdeblick TA, Cooke ME, Wilson D, et al: Anterior cervical discectomy, fusion, and plating: a comparative animal study, Spine 18:1974, 1993.
- Zdeblick TA, Ducker TB: The use of freeze-dried allograft bone for anterior cervical fusions, Spine 16:726, 1991.
- Zdeblick TA, Hughes SS, Riew D, et al: Failed anterior cervical discectomy and arthrodesis, J Bone Joint Surg 79A:523, 1997.
- Zdeblick TA, Wilson D, Cooke ME, et al: Anterior cervical discectomy and fusion: a comparison of techniques in an animal model, Spine 17:S418, 1992.
- Zeller RD, Ghanem I, Miladi L, et al: Posterior spinal fusion in
