DEFINITION
Pronator and anterior interosseous syndromes are compression neuropathies of the median nerve and its main branch, the anterior interosseous nerve (AIN), at the elbow, and proximal forearm.
ANATOMY
The median nerve passes in the distal upper arm between the brachialis and the medial intermuscular septum, with the brachial artery sitting lateral to it.A rare supracondylar process may arise from the distal aspect of the humerus, giving origin to a fibrous band extending to the medial epicondyle. This is the ligament of Struthers.If a ligament of Struthers is present, the median nerve passes underneath it.At the elbow, the median nerve sits underneath the lacertus fibrosus and then typically passes between the superficial (humeral) head and the deep (ulnar) head of the pronator teres.In 20% of individuals, the deep head is absent or consists of a small fibrous band.Motor branches to the palmaris longus, flexor carpi radialis, flexor digitorum superficialis, and flexor digitorum profundus typically branch from the median nerve in an ulnar direction proximal to the pronator teres.Under the pronator teres, the AIN branches in a radial direction from the median nerve, and both pass underneath the fibrous arcade of the flexor digitorum superficialis.The surgeon should be cognizant of the cutaneous nerves passing over the antecubital and proximal forearm region. Damage to these nerves can result in numbness and paresthesia as well as symptomatic neuromas in the forearm.Anomalous muscles and nerve branches may be present, the most common of which is the so-called Martin-Gruber anastomosis.The surgeon should also be aware of more proximal or distal branching of the AIN from the median nerve.The Martin-Gruber anastomosis, which occurs in about 15% of the population, consists of branches from either the median nerve or AIN to the ulnar nerve.
PATHOGENESIS
Compression of the median nerve in the proximal forearm is rare compared with carpal tunnel syndrome.Median nerve compression in the proximal forearm has been labeled as eitherpronator syndromeoranterior interosseous syndrome.The true incidence of median nerve compression in the proximal forearm is difficult to ascertain, as is the relative contribution of the various potential impinging structures.Numerous studies have shown that the most common causes of median nerve compression in the region of the elbow and proximal forearm seem to be fascial bands and muscular anomalies of the pronator teres andthe fibrous arcade of the flexor digitorum superficialis.3,6Less common sites of nerve compression include the lacertus fibrosus and the ligament of Struthers (in cases with an existing supracondylar process).A large number of additional structures have been identified as potential sources of compression of themedian nerve. These include an accessory bicipital aponeurosis8 and a variety of anomalous muscles, the most frequently cited of which is the accessory head of the flexor pollicis longus muscle, orGantzer muscle.A persistent median artery penetrating the median nerve also has been described.4Space-occupying lesions such as lipomas or scarring from trauma can result in nerve compression.Anterior interosseous syndrome caused by nerve compression must be differentiated from Parsonage-Turner syndrome or mononeuritis.
NATURAL HISTORY
Compression of the median nerve in the forearm often is transient due to excessive physical activity or swelling from injury.Recovery from Parsonage-Turner syndrome can be prolonged, but the prognosis usually is good without surgical decompression.The natural history and prognosis of pronator syndrome is not well understood.
PATIENT HISTORY AND PHYSICAL FINDINGS
Classically, pronator syndrome presents as paresthesia in the median nerve distribution with minimal or no weakness. The patient also may complain of pain localized to the proximal forearm that is increased with activities. There may be a focal area of increased pain localizing to the specific area of compression.In severe cases, weakness of the anterior interosseous innervated muscles—the flexor pollicis longus, the index and long flexor digitorum profundus, and the pronator quadratus—might be seen as well as select thenar muscles.P.863Theoretically, patients may have paresthesia in the distribution of the palmar cutaneous branch of the median nerve, in contrast to carpal tunnel syndrome.AIN syndrome presents as diminished motor function of the index (and long) flexor digitorum profundus, flexor pollicis longus, and pronator quadratus without injury or specific known cause.The patient typically complains of spontaneous loss of dexterity and voices specific complaints related to flexion of the thumb interphalangeal (IP) joint and/or index distal interphalangeal (DIP) joint.Decreased sensation is not a common presenting symptom.In cases of space-occupying lesions or scarring from trauma compressing the nerve, one would expect to see sensory symptoms as well as motor abnormalities.Patients suffering from Parsonage-Turner syndrome often will experience a prodromal viral-type illness together with significant pain for several days or weeks before the onset of weakness.Physical examinations to perform include the following:Pronator compression test. Paresthesia in the median nerve distribution within 30 seconds is considered a positive test. The test is nonspecific and can be seen with carpal tunnel syndrome.Resisted proximal interphalangeal (PIP) joint flexion of long finger. Paresthesia in the median nerve distribution and pain in the forearm are considered a positive test. The test is thought to be consistent with compression of the median nerve at the fibrous arcade of the flexor digitorum superficialis.Resisted pronation test. Paresthesia in the median nerve distribution and pain are considered a positive test. A positive finding is consistent with compression of the median nerve by the pronator teres.Elbow flexion test. Paresthesia and pain are considered a positive test. A positive test is thought to be consistent with lacertus fibrosus compression of the median nerve.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Electrodiagnostic studies are often not helpful in pronator syndrome. Numerous studies have shown that symptoms and outcome of surgery do not correlate well with electrodiagnostic studies.In anterior interosseous syndrome, electrodiagnostic studies will confirm denervation of the anterior interosseous muscles.Electrodiagnostic studies are most valuable in the diagnosis of proximal median nerve compression for ruling out carpal tunnel syndrome.Ultrasonography and magnetic resonance imaging (MRI) are valuable tests for identifying space-occupying lesions such as lipomas or ganglions.MRI can be a useful investigation to evaluate anterior interosseous syndrome showing edema within the pronator quadratus.1Plain radiographs of the proximal forearm and elbow may reveal a supracondylar process or anatomic variation.
DIFFERENTIAL DIAGNOSIS
Carpal tunnel syndromeMononeuritis or Parsonage-Turner syndrome Other form of neuritis
NONOPERATIVE MANAGEMENT
In the acute phase, rest, immobilization, and avoidance of aggravating activities, such as repetitive pronation and heavy gripping, should be recommended.Forearm stretching exercises can be tried in chronic cases.Modalities such as ultrasound and electrostimulation have been advocated, although there is limited validation of their usefulness.Nerve gliding and nerve mobilization remain controversial.Spontaneous recovery does appear to occur in the majority of patients with anterior interosseous syndrome, although recovery can take up to 12 months.7,10
SURGICAL MANAGEMENT
APPROACH
The greatest variation in surgical technique concerns the skin incision.For decompression of both pronator and anterior interosseous syndromes, extensile exposures using a modification of Henry approach allows for safe and thorough exposure of the median nerve and decompression of all sites of potential compression.This incision sometimes is associated with unsightly scarring and injuries to the cutaneous nerves.Lesser incisions have been described, therefore; these include a lazy S-shape incision in the proximal volar forearm as well as two longitudinal,2 oblique,6,11 and transverse9 incisions.Limited incisions require significant retraction to ensure decompression both proximally and distally.Endoscopic decompression has been recently described.5 Whether the advantages of an endoscopic release outweigh the increased cost and risks remains unknown.The surgeon's experience and comfort level may be the determining factors in deciding on the type of incision.P.864
TECHNIQUES
EXTENSILE APPROACH
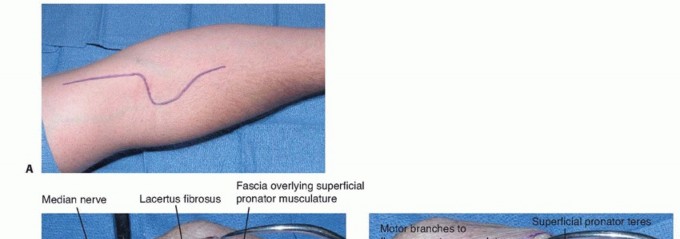


TECH FIG 1 • Extensile exposure. A. Skin incision. B. Incision with demonstrated lacertus fibrosus. C. Retracted but not released superficial pronator teres and intact flexor digitorum superficialis arch.(continued)


TECH FIG 1 •(continued)D. Retracted pronator and released superficial arch. E. Z-lengthened superficial pronator teres tendon.


TECH FIG 2 • Oblique limited exposure. A. Skin incision. B. Retracted pronator teres with exposed superficialis arch.




TECH FIG 3 • Endoscopic technique. A. Hoffman endoscope sheath (Karl Storz GmbH & Co., Tuttlingen, Germany). B. Skin incision. C. Median nerve prior to insertion of the endoscope. D. Median nerve viewed through the endoscope. The endoscope is first inserted proximally, lifting the soft tissues above the median nerve.Scissors are then used to release the proximal extension of the bicipital aponeurosis under endoscopic view.The endoscope is then directed distally, and the tendinous or fibrous band associated with the pronator teres muscle is identified.The fibrous portion of the pronator teres as well as the ulnar and humeral head can be released at this point by a technique combining spreading and cutting.The fibrous arch of the flexor digitorum superficialis is then identified and released using scissors.P.867
PEARLS AND PITFALLS
Anatomy ▪ Tendinous portions of the pronator teres and the fibrous portions of the arcade of the flexor digitorum superficialis are the most common causes of compression.1. Motor branches that go from the median nerve to the muscles originating from the medial epicondyle branch from the ulnar side of the nerve.2. The AIN originates from the radial side of the median nerve and under the pronator teres.3. Considerable variation occurs within the pronator teres. Tendinous portions of the pronator impinging on the median nerve should be released, with preservation of the muscle fibers when possible.4. The humeral or superficial head of the pronator teres is the largest portion of the muscle. The ulnar head or deep head is far smaller, sometimes absent, and most commonly is deep to the median nerve. Both heads, however, have tendinous insertion sites, which may be sources of impingement. In addition, fascial connections between the heads may be present, impinging on the median nerve.Surgical technique4. The fibrous portion of the superficialis arcade can be released with preservation of the muscle.5. Palpation and visualization proximally and distally can be obtained by appropriate retraction.6. Extensile exposures result in easier surgery but at the expense of potential unsightly scarring and dysesthesia from cutaneous nerve injury.7. Judicious release of the pronator teres limits the postoperative morbidity and decreases the recovery time.Relation to carpal tunnel syndrome8. Patients often may have both carpal tunnel syndrome and a more proximal compression, resulting in the so-called double crush phenomenon.9. Some authors have implied that failed carpal tunnel syndrome is due to a misdiagnosis in which the more proximal compression of the median nerve in the forearm was not identified.10. In cases, however, where electrodiagnostic studies clearly show carpal tunnel syndrome even when proximal forearm symptoms are present, it is wise to merely decompress the carpal canal because the carpal tunnel procedure has a more predictable outcome with less morbidity than proximal forearm median nerve decompression.
POSTOPERATIVE CARE
Splinting or casting is avoided.Early elbow range of motion is encouraged.If the pronator tendon has been released, lifting and forearm rotation are restricted for 4 weeks.
OUTCOMES
Outcome following surgical treatment of proximal forearm median nerve compression has been inconsistent compared to the more uniformly good outcomes associated with carpal tunnel release.Many, if not most, patients continue to be at least somewhat symptomatic after surgical decompression. This may reflect persistent compression due to inadequate release or scarring from the surgery itself. It is more likely, however, that it reflects the difficulty in making the diagnosis due to the lack ofobjective criteria.Few studies have evaluated outcome following median nerve decompression in the forearm. Most such studies report results of decompression for pronator syndrome.Olehnik et al6 and Hartz et al3 both reported results for decompression of pronator syndrome.Olehnik et al6 showed surgery to be of benefit in 30 of 37 extremities, but 9 of 39 were unchanged and 20 had only partial relief.Hartz et al3 showed 28 good or excellent results in 36 operations, but a majority of patients still had symptoms.Lee et al5 showed that 13 patients improved symptomatically as measured by Disability of the Arm, Shoulder, and Hand (DASH) scoring after endoscopically assisted decompression.
COMPLICATIONS
Persistent symptoms due to incorrect diagnosisDamage to cutaneous nerve branches with subsequent dysesthesiasDamage to or scarring of motor branches of median nerve or interosseous nerve Scarring of pronator teres and forearm musculature
REFERENCES
- Dunn AJ, Salonen DC, Anastakis DJ. MR imaging findings of anterior interosseous nerve lesions. Skeletal Radiol 2007;36:1155-1162.
- Gainor BJ. Modified exposure for pronator syndrome decompression: a preliminary experience. Orthopedics 1993;1612:1329-1331.
- Hartz CR, Linscheid RL, Gramse RR, et al. The pronator teres syndrome: compressive neuropathy of the median nerve. J Bone Joint Surg Am 1981;63(6):885-890.
- Jones NF, Ming NL. Persistent median artery as a cause of pronator syndrome. J Hand Surg Am 1988;13:728-732.
- Lee AK, Khorsandi M, Nurbhai N, et al. Endoscopically assisted decompression for pronator syndrome. J Hand Surg Am 2012;37(6): 1173-1179.
- Olehnik WK, Manske PR, Szerzinski J. Median nerve compression in the proximal forearm. J Hand Surg Am 1994;19:121-126.
- Seki M, Nakamura H, Kono H. Neurolysis is not required for young patients with a spontaneous palsy of the anterior interosseous nerve. J Bone Joint Surg Br 2006;88(12):1606-1609.
- Spinner RJ, Carmichael SW, Spinner M. Partial median nerve entrapment in the distal arm because of an accessory bicipital aponeurosis. J Hand Surg Am 1991;16:236-244.
- Tsai TM, Syed SA. A transverse skin incision approach for decompression of pronator teres syndrome. J Hand Surg Br 1994;19:40-42.
- Ulrich D, Piatkowski A, Pallua N. Anterior interosseous nerve syndrome: retrospective analysis of 14 patients. Arch Orthop Trauma Surg 2011;131:1561-1565.
- Zancolli ER III, Zancolli EP IV, Perrotto CJ. New mini-invasive decompression for pronator teres syndrome. J Hand Surg Am 2012; 37(8):1706-1710.
