PATHOPHYSIOLOGY AND BIOMECHANICS OF EPICONDYLITIS
Epicondylitis, despite its nomenclature, is fundamentally a degenerative tendinosis rather than an acute inflammatory condition. Histological analysis consistently demonstrates angiofibroblastic hyperplasia—characterized by disorganized, immature collagen formation, fibroblastic proliferation, and non-functional vascularity—without a significant presence of acute inflammatory cells (macrophages, neutrophils).
In lateral epicondylitis (tennis elbow), the primary site of pathology is the origin of the extensor carpi radialis brevis (ECRB). The ECRB is uniquely susceptible to microtrauma due to its anatomical position; it undergoes significant shearing forces against the lateral epicondyle and capitellum during combined elbow extension and forearm pronation.
In medial epicondylitis (golfer's elbow), the pathology localizes to the flexor-pronator mass, specifically the origins of the pronator teres (PT) and the flexor carpi radialis (FCR). This condition is frequently driven by repetitive valgus stress and wrist flexion, commonly seen in overhead throwing athletes and racket sports players.
Surgical intervention is indicated only after exhaustive nonoperative management—including structured physical therapy emphasizing eccentric strengthening, nonsteroidal anti-inflammatory drugs (NSAIDs), counterforce bracing, and judicious corticosteroid or biologic injections—has failed to provide relief after 6 to 12 months.
CORRECTION OF LATERAL EPICONDYLITIS (TENNIS ELBOW)
The modified Nirschl technique remains the gold standard for the open surgical management of recalcitrant lateral epicondylitis. The primary objective is the meticulous identification and excision of the angiofibroblastic tissue within the ECRB, decortication of the lateral epicondyle to stimulate a healing response, and secure reattachment of the healthy tendon.
Surgical Anatomy and Preoperative Planning
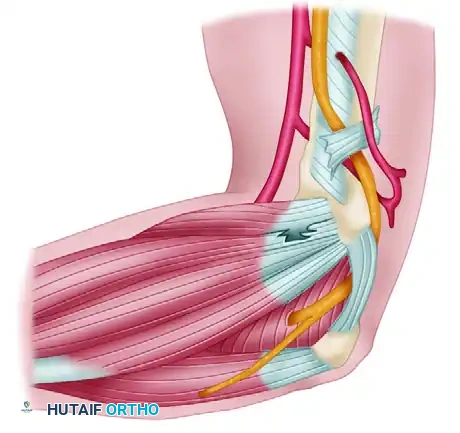
The common extensor origin comprises the extensor carpi radialis brevis (ECRB), extensor digitorum communis (EDC), extensor digiti minimi (EDM), and extensor carpi ulnaris (ECU). The extensor carpi radialis longus (ECRL) originates more proximally on the lateral supracondylar ridge. The pathological ECRB tissue is typically situated deep to the ECRL and anterior to the EDC.
Surgical Warning: The lateral ulnar collateral ligament (LUCL) lies immediately deep and posterior to the ECRB origin. Overzealous excision or deep dissection at the posterior aspect of the lateral epicondyle can compromise the LUCL, leading to iatrogenic posterolateral rotatory instability (PLRI) of the elbow.
Surgical Technique: Modified Nirschl Procedure
1. Positioning and Incision
* Place the patient supine with the operative arm draped free on a hand table. A sterile tourniquet is applied to the proximal arm.
* Make a gently curved incision, approximately 5 cm in length, centered directly over the lateral epicondyle.
* Incise the deep fascia in line with the skin incision and retract the fascial flaps to expose the underlying musculature.
2. Interval Identification
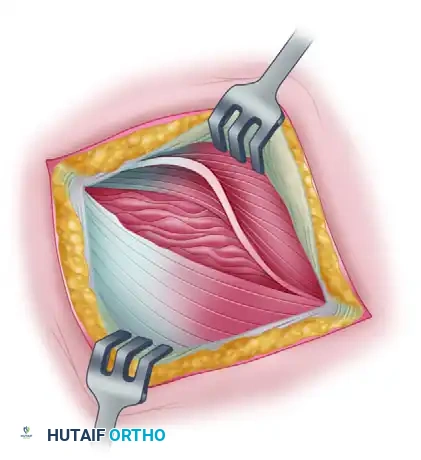
* Identify the extensor carpi radialis longus (ECRL) and the origin of the extensor digitorum communis (EDC). The EDC partially obscures the deeper origin of the ECRB.
* Develop the interval between the ECRL and the EDC. Retract the ECRL anteriorly to expose the underlying ECRB origin.
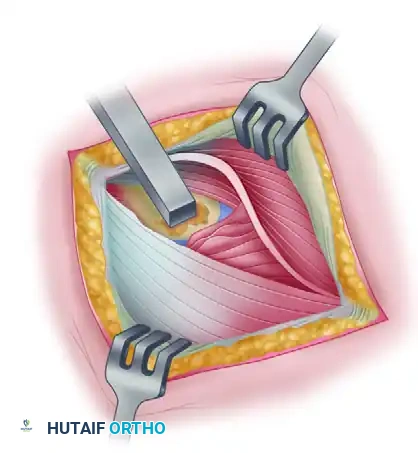
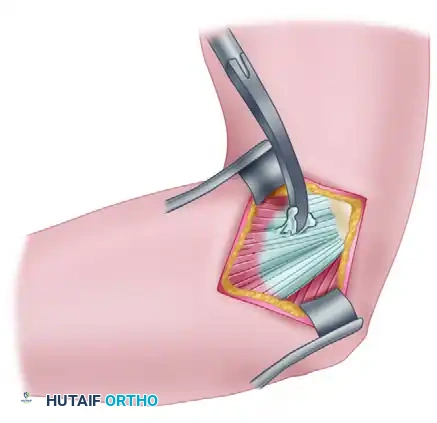
3. Excision of Pathological Tissue
* Elevate the brevis portion of the conjoined tendon at the midportion of the lateral epicondyle, reflecting it toward the elbow joint.
* Carefully differentiate between normal Sharpey fibers and the diseased tendon. The pathological angiofibroblastic tissue typically appears gray, friable, fibrillated, and discolored. It may also contain focal calcium deposits.
* Excise the abnormal ECRB tendon entirely. If the disease process extends into the anterior portion of the EDC origin, this involved tissue must also be excised.
* Note: The elbow joint capsule should not be violated unless preoperative imaging or clinical evaluation indicates an intra-articular pathology (e.g., loose bodies, synovial plica, or advanced radiocapitellar degenerative joint disease).
4. Epicondylar Decortication
* Once the diseased tissue is removed, decorticate a small, localized area of the anterior lateral epicondyle using a rongeur, curette, or a small osteotome.
* This step exposes a bleeding cancellous bone bed, which provides mesenchymal stem cells and growth factors necessary to facilitate robust tendon-to-bone healing.
Clinical Pearl: When decorticating the lateral epicondyle, direct the osteotome or rongeur carefully to avoid penetrating the joint capsule and damaging the delicate articular cartilage of the capitellum.
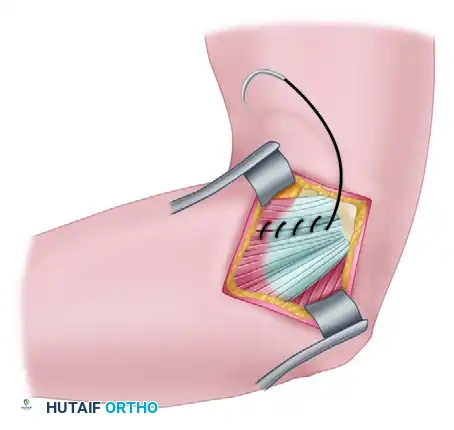
5. Tendon Repair and Closure
* Suture the remaining healthy ECRB tendon to the adjacent intact fascia or periosteum. Alternatively, it can be attached directly to the decorticated epicondyle using nonabsorbable sutures passed through transosseous drill holes. While suture anchors are frequently utilized and highly successful, transosseous tunnels remain a biomechanically sound and cost-effective alternative.
* Close the ECRL and EDC interval meticulously with absorbable sutures. This closure should completely cover the knots of the ECRB repair.
* Close the subcutaneous tissue and skin with absorbable 4-0 sutures and apply adhesive strips.
CORRECTION OF MEDIAL EPICONDYLITIS (GOLFER'S ELBOW)
Medial epicondylitis is significantly less common than its lateral counterpart but is notoriously more difficult to treat. The pathology primarily involves the origins of the pronator teres and the flexor carpi radialis, and less frequently, the flexor digitorum superficialis and flexor carpi ulnaris.
Diagnostic Considerations
Medial epicondylitis must be carefully differentiated from ulnar neuropathy (cubital tunnel syndrome) and medial ulnar collateral ligament (MUCL) insufficiency. Physical examination reveals maximal tenderness approximately 5 mm distal and anterior to the midpoint of the medial epicondyle. Pain is exacerbated by resisted forearm pronation and wrist flexion. Radiographs may reveal medial ulnar traction spurs or MUCL calcifications, indicative of chronic valgus overload.
Surgical Technique: Nirschl Medial Approach
If conservative treatment fails, open debridement and reattachment of the flexor-pronator origin is indicated. The Nirschl technique emphasizes the excision of pathological tissue while preserving the surrounding normal tendinous structures.
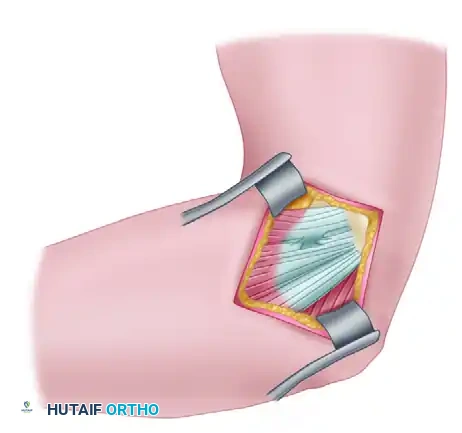
1. Exposure and Nerve Protection
* Make a longitudinal incision centered over the medial epicondyle.
* Identify and protect the medial antebrachial cutaneous nerve branches.
Surgical Warning: The ulnar nerve lies immediately posterior to the medial epicondyle in the cubital tunnel. If the patient exhibits preoperative ulnar nerve symptoms (e.g., paresthesias in the ring and small fingers, positive Tinel's sign), an ulnar nerve decompression and anterior transposition must be performed concomitantly.
2. Longitudinal Exposure of the Flexor-Pronator Mass
* Perform a longitudinal incision through the common flexor tendon to expose the underlying pathological tissue.
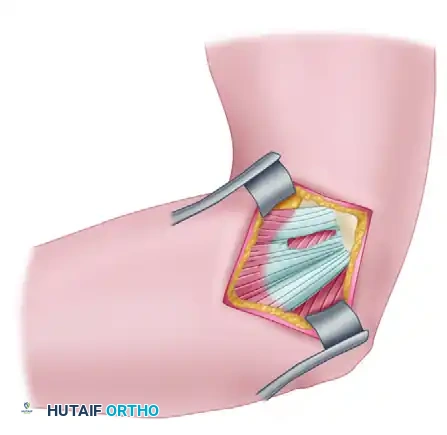
3. Excision of Pathological Tissue
* Identify the angiofibroblastic tissue within the pronator teres and flexor carpi radialis origins.
* Excise the frayed, degenerated tissue down to bleeding bone.
4. Preservation of Normal Tissue
* Ensure that the normal, healthy tissue of the pronator origin and the surrounding flexor mass is left intact to maintain structural integrity and facilitate repair.
5. Epicondylectomy and Closure
* A partial medial epicondylectomy may be performed to enhance the healing bed; however, strictly limit resection to no more than 20% to 25% of the epicondyle to prevent iatrogenic MUCL compromise.
* Close the defect in the flexor-pronator origin securely using heavy absorbable or nonabsorbable sutures, anchoring the healthy tendon back to the prepared bony bed.
POSTOPERATIVE REHABILITATION PROTOCOL
Rehabilitation following epicondylar debridement is goal-dependent rather than strictly time-dependent. Patients must meet specific clinical milestones before advancing to the next phase.
Phase 1: Acute Phase (Weeks 0–2)
Goals: Reduce inflammation, promote tissue healing, and retard muscular atrophy.
* Immobilization: The postoperative splint is removed within the first 5 to 7 days.
* Modalities: Cryotherapy, high-voltage galvanic stimulation, and whirlpool therapy.
* Range of Motion (ROM): Initiate gentle, passive, and active-assisted wrist extension/flexion, elbow extension/flexion, and forearm supination/pronation.
* Restrictions: Strict avoidance of painful movements, particularly forceful gripping or lifting.
Phase 2: Subacute Phase (Weeks 2–6)
Goals: Improve flexibility, increase muscular strength and endurance, and initiate functional activities.
* Strengthening: Emphasize concentric and eccentric strengthening of the involved muscle groups (wrist extensors for lateral; wrist flexors/pronators for medial).
* Proximal Stabilization: Initiate shoulder and scapular strengthening to correct any kinetic chain deficiencies.
* Support: A counterforce brace may be utilized during activities.
* Progression: Gradually reintroduce previously painful movements in a controlled environment.
Phase 3: Chronic Phase (Weeks 6–12+)
Goals: Maximize muscular strength, maintain flexibility, and return to high-level sports or occupational activities.
* Advanced Strengthening: Continue heavy eccentric loading protocols.
* Sport-Specific Training: Initiate a gradual return to sport activity (e.g., interval throwing programs or modified racket use).
* Equipment Modification: Recommend adjustments such as increasing racket grip size, lowering string tension, or altering the playing surface to reduce shock transmission.
* Outcomes: Strenuous activity can typically be resumed within the limits of pain by 8 to 10 weeks, with full power and maximal medical improvement expected at approximately 3 to 6 months.
SURGICAL MANAGEMENT OF ELBOW CONTRACTURES
Elbow stiffness is a debilitating complication following trauma, prolonged immobilization, or chronic inflammatory conditions. The functional arc of elbow motion required for most activities of daily living (ADLs) is 30 to 130 degrees of flexion, with 50 degrees of both pronation and supination.
Surgical intervention is strongly considered for patients who fail nonoperative management (splinting, physical therapy) and present with an arc of motion less than 100 degrees, or a severe flexion contracture exceeding 45 degrees.
Classification of Contractures
Understanding the etiology of the contracture is paramount for surgical planning:
1. Extrinsic Causes: Pathology lies outside the articular cartilage. This includes contractures of the joint capsule, collateral ligament shortening, extra-articular malunions, and heterotopic ossification (HO).
2. Intrinsic Causes: Pathology involves the articular surfaces. This includes intra-articular step-off fractures, advanced cartilage degradation, osteochondral defects, and dense intra-articular adhesions.
Clinical Pearl: Extrinsic capsular contractures are almost universally present when intrinsic articular causes are the primary pathology. Therefore, any intrinsic joint reconstruction must be accompanied by a comprehensive capsular release.
Preoperative Evaluation
A meticulous history and physical examination are required. Plain radiographs evaluate joint congruity and the presence of osteophytes or heterotopic ossification. Advanced imaging, including MRI and CT with three-dimensional (3D) reconstruction, is highly recommended to precisely map bony impingements (e.g., osteophytes in the olecranon or coronoid fossae) and guide the surgical approach.
Surgical Approaches for Contracture Release
If the joint surfaces are preserved and the contracture is purely extrinsic, an arthroscopic or open capsular release is highly effective. However, if intrinsic destruction is present, complex distraction arthroplasty or fascial interposition may be required.
The Lateral Column Procedure
For post-traumatic flexion contractures, a modified lateral approach—often termed the "column procedure"—is highly advantageous.
* Exposure: This technique utilizes an extensile modification of the Nirschl lateral epicondylitis approach. It allows comprehensive exposure of the anterior elbow joint capsule without violating the common extensor origin or the lateral collateral ligament (LCL) complex.
* Anterior Release: The anterior capsule is excised to restore extension.
* Posterior Release: If flexion is limited, a posterior triceps-splitting or paratricipital approach is utilized to expose the posterior compartment. The posterior capsule is released, and any fibrotic debris or osteophytes are cleared from the olecranon fossa.
* Triceps Tenolysis: Adhesions between the triceps and the posterior humerus are lysed to further improve flexion.
Advantages of the Lateral Approach:
1. Allows simultaneous anterior and posterior capsulectomy from a single or slightly modified incision.
2. Provides excellent access to the olecranon fossa for debridement.
3. Minimizes wound healing complications, which is critical when postoperative Continuous Passive Motion (CPM) machines are utilized immediately following surgery to maintain the intraoperative gains in range of motion.
