Comprehensive Introduction and Patho-Epidemiology
Metacarpal neck fractures represent one of the most ubiquitous osseous injuries encountered in the realm of hand trauma, accounting for approximately ten percent of all fractures presenting to the orthopedic surgeon and up to forty percent of all hand fractures. Frequently presenting as the classic "boxer's fracture" of the fifth metacarpal, these injuries are predominantly the result of a direct axial load applied to a clenched fist. While the vast majority of these fractures are managed non-operatively with excellent functional outcomes—owing largely to the robust compensatory mechanisms of the adjacent carpometacarpal (CMC) joints—a distinct and challenging subset will progress to symptomatic malunion. The epidemiological profile of this cohort is heavily skewed toward young, active males, a demographic in which functional demands are exceptionally high and tolerance for grip weakness or digital dyskinesia is correspondingly low.
Metacarpal neck malunions are pathognomonically characterized by apex-dorsal angulation, volar displacement of the metacarpal head, shortening of the metacarpal ray, and potentially debilitating malrotation. The natural history of a poorly reduced or unstable metacarpal neck fracture involves the unopposed pull of the intrinsic musculature, specifically the volar interossei, which continuously exert a deforming force that exacerbates volar angulation. Furthermore, the extensor digitorum communis (EDC) and the flexor digitorum superficialis and profundus (FDS/FDP) tendons create a longitudinal compressive force across the fracture site, driving the distal fragment into further flexion and shortening. When these forces are not neutralized by appropriate immobilization or internal fixation during the acute phase, the fracture consolidates in this deformed position, initiating a cascade of biomechanical derangements.
For the orthopedic surgeon, addressing an established metacarpal neck malunion requires a profound understanding of hand biomechanics and soft-tissue homeostasis. The functional deficit observed in the clinical setting is rarely attributable to the osseous deformity in isolation. Rather, it is the secondary soft-tissue imbalances—specifically the alteration of the intrinsic muscle tension, the attenuation of the sagittal bands, and the severe contracture of the metacarpophalangeal (MCP) joint collateral ligaments—that drive the patient's clinical symptoms. As the metacarpal head translates volarly, the delicate balance between the extrinsic extensors and the intrinsic flexors is disrupted, leading to a predictable pattern of digital dysfunction that can severely compromise the patient's occupational and recreational capabilities.
The socioeconomic impact of symptomatic metacarpal malunions should not be underestimated. Patients frequently report chronic pain during power grip, an inability to firmly grasp cylindrical objects, and significant cosmetic dissatisfaction due to the loss of the normal dorsal knuckle contour. The evolution of surgical intervention for this condition has shifted from a purely structural focus (restoring the bone straightness) to a comprehensive biomechanical restoration, emphasizing the absolute necessity of addressing concomitant soft-tissue contractures. Consequently, the modern orthopedic approach to metacarpal neck malunion is a highly orchestrated procedure demanding precise preoperative templating, meticulous soft-tissue handling, and rigid internal fixation.

Detailed Surgical Anatomy and Biomechanics
A thorough mastery of the surgical anatomy of the metacarpal and its surrounding soft-tissue envelope is the absolute prerequisite for successful malunion correction. The metacarpal bone is structurally divided into the base, shaft (diaphysis), neck (metaphysis), and head. The metacarpal neck is an area of relative structural weakness, marking the transition from the thick cortical bone of the diaphysis to the thinner, cancellous bone of the metacarpal head. The metacarpal head itself is eccentrically shaped, presenting a cam-like profile in the sagittal plane. This cam morphology is critical for the function of the MCP joint collateral ligaments. In full extension, the collateral ligaments are lax, allowing for significant abduction and adduction of the digit. As the MCP joint flexes, the ligaments are drawn tightly over the broader volar aspect of the condyles, maximizing joint stability for power grip.
When a metacarpal neck fracture heals with excessive volar angulation, the biomechanical cascade is predictable and often debilitating. The most prominent clinical manifestation is "pseudoclawing." The volar displacement of the metacarpal head relatively lengthens the interosseous muscles, reducing their mechanical advantage and resting tension. To compensate for this perceived laxity and to achieve digital extension, the extensor digitorum communis (EDC) must exert a greater force, which inevitably hyperextends the MCP joint. This MCP hyperextension subsequently alters the tension across the extensor mechanism, leading to secondary proximal interphalangeal (PIP) joint flexion, mimicking an intrinsic-minus claw hand.
Furthermore, the altered vector of the flexor tendons and the shortened metacarpal lever arm can significantly diminish grip strength, particularly in power grip. The flexor tendons, which normally glide smoothly volar to the MCP joint, are forced to navigate a more acute angle, increasing friction and decreasing their effective moment arm. Concurrently, the dorsal apex of the fracture becomes prominent subcutaneously, while the normal prominence of the metacarpal head is lost, leading to the classic "sunken knuckle" deformity and cosmetic dissatisfaction. Even minor degrees of malrotation (as little as 5 degrees) at the metacarpal level can result in up to 1.5 cm of digital overlap at the fingertips during composite flexion, severely impairing grasp and causing the affected digit to cross under or over its neighbor.
The tolerance for sagittal plane angulation varies significantly across the hand, dictated entirely by the mobility of the respective carpometacarpal (CMC) joints. The index and long fingers (2nd and 3rd metacarpals) are rigidly fixed at their CMC joints, forming the stable central pillar of the hand. They tolerate almost no angulation, with a maximum acceptable limit of 10 to 15 degrees before symptomatic pseudoclawing and palmar pain occur. Conversely, the ring and small fingers (4th and 5th metacarpals) possess 15 to 30 degrees of compensatory CMC mobility. This mobility allows the ulnar border of the hand to cup around objects and enables these digits to tolerate up to 40 to 50 degrees of angulation without severe functional deficit. Recognizing these biomechanical thresholds is paramount in determining the necessity of surgical intervention.


Exhaustive Indications and Contraindications
Surgical correction of a metacarpal neck malunion is a technically demanding endeavor and is emphatically not indicated for cosmetic deformity alone. The decision to proceed with an osteotomy must be rooted in a thorough clinical evaluation demonstrating a clear, objective functional deficit that correlates directly with the radiographic deformity. The primary philosophy of intervention is the restoration of the hand's biomechanical equilibrium, specifically targeting the elimination of pain during grip, the correction of digital overlap, and the resolution of intrinsic muscle imbalance.
The primary indications for corrective osteotomy include symptomatic pseudoclawing that actively interferes with hand function, such as difficulty opening the hand to grasp large objects or a loss of coordinated fine motor skills. A painful grip due to a prominent volar metacarpal head in the palm is another absolute indication; this occurs when the volarly displaced head creates a localized pressure point against objects held in the hand, making manual labor or weight-bearing tasks excruciating. Furthermore, clinically significant malrotation causing digital overlap during composite flexion is an urgent indication for surgery, as rotational deformities do not remodel and permanently disrupt the parallel cascade of the flexing digits. Finally, angulation exceeding acceptable biomechanical tolerances (e.g., >15° in the index/long fingers, >50° in the small finger) in a symptomatic patient warrants surgical correction.
Conversely, absolute and relative contraindications must be meticulously respected to avoid catastrophic outcomes. Active localized or systemic infection is an absolute contraindication to any elective osteotomy and internal fixation. Severe, established Complex Regional Pain Syndrome (CRPS) is a strong relative contraindication; surgical trauma can exacerbate the condition, leading to a stiff, non-functional hand that is worse than the initial malunion. A poor soft-tissue envelope, such as thin, scarred, or adherent skin over the dorsum of the hand from prior trauma or multiple surgeries, significantly increases the risk of wound breakdown and hardware exposure. Finally, severe osteoarthritis of the adjacent MCP joint may render a simple corrective osteotomy futile, as the joint itself is the source of pain and stiffness, potentially necessitating an arthroplasty or arthrodesis instead.
| Category | Specific Factors | Clinical Rationale for Surgical Decision-Making |
|---|---|---|
| Absolute Indications | Malrotation with digital overlap | Rotational deformity does not remodel; permanently impairs composite grasp. |
| Painful palmar prominence | Volar metacarpal head creates a pressure point during power grip, disabling manual laborers. | |
| Symptomatic Pseudoclawing | MCP hyperextension and PIP flexion disrupt the functional arc of motion. | |
| Relative Indications | Angulation > 50° (Small finger) | Exceeds compensatory capacity of the 5th CMC joint; high risk of future symptoms. |
| Angulation > 15° (Index/Long) | Rigid central pillar cannot compensate; alters flexor tendon mechanics. | |
| Cosmetic dissatisfaction | Only considered if accompanied by psychological distress and mild functional impairment. | |
| Contraindications | Active Infection (Osteomyelitis) | High risk of hardware seeding and catastrophic failure of the osteotomy. |
| Severe CRPS | Surgical trauma will likely trigger a severe flare, resulting in a stiff, useless hand. | |
| Advanced MCP Osteoarthritis | Correcting the shaft will not resolve intra-articular pain; arthroplasty/fusion preferred. | |
| Non-compliant patient | Postoperative rehabilitation is rigorous; failure to comply leads to stiffness or hardware failure. |

Pre-Operative Planning, Templating, and Patient Positioning
The success of a metacarpal neck malunion correction is dictated long before the first incision is made. Preoperative radiographic assessment must be exhaustive, including true posteroanterior (PA), lateral, and oblique views of the individual affected digit, rather than standard whole-hand views, which frequently obscure the metacarpal neck due to osseous overlap. The true lateral view of the individual metacarpal is paramount for accurately measuring the degree of apex-dorsal angulation. The degree of angulation is measured using the medullary canal lines of the proximal shaft and the line perpendicular to the distal articular surface. In cases of complex, multi-planar deformities or suspected intra-articular extension of the previous fracture, a fine-cut computed tomography (CT) scan with 3D reconstructions is highly recommended to fully appreciate the spatial orientation of the malunion.
Digital templating is an indispensable step in the preoperative workflow. The surgeon must identify the Center of Rotation of Angulation (CORA) to determine the optimal site and type of osteotomy. For metacarpal neck malunions, the CORA is typically located at the apex of the deformity. A closing wedge osteotomy is historically common but has the distinct disadvantage of further shortening an already shortened metacarpal ray, which can exacerbate intrinsic muscle laxity. Therefore, an opening wedge osteotomy with structural bone grafting, or a transverse osteotomy utilizing an intramedullary cortical bone peg, is generally preferred to restore both angular alignment and anatomical length. The precise dimensions of the required bone graft or peg must be calculated preoperatively.
Anesthetic considerations require a collaborative approach between the surgeon and the anesthesiologist. Regional anesthesia, specifically a targeted brachial plexus block (supraclavicular or axillary), is highly preferred. This not only provides excellent intraoperative analgesia and sympathectomy (reducing vasospasm) but also allows the surgeon to assess the tenodesis effect intraoperatively if the patient is lightly sedated and able to actively flex the digits upon request. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) must be administered within one hour prior to tourniquet inflation.
Patient positioning is critical for optimal surgical ergonomics and fluoroscopic access. The patient is positioned supine with the operative arm extended on a specialized, radiolucent hand table. A well-padded upper arm pneumatic tourniquet is applied and typically inflated to 250 mmHg after exsanguination of the limb with an Esmarch bandage. The fluoroscopy unit (C-arm) should be positioned to enter from the head or the foot of the table, allowing the surgeon unimpeded access to both the dorsal and volar aspects of the hand. If an autologous bone graft is planned, the donor site (e.g., proximal ulna/olecranon, distal radius, or iliac crest) must be simultaneously prepped and draped in a sterile fashion.


Step-by-Step Surgical Approach and Fixation Technique
The surgical correction of a metacarpal neck malunion demands meticulous soft-tissue handling, precise osseous resection, and rigid internal fixation. The following details the classic corrective osteotomy utilizing an intramedullary cortical bone peg, a highly stable and biologically sound technique for restoring metacarpal length and alignment, alongside contemporary fixation alternatives.
Incision and Soft Tissue Dissection
A longitudinal dorsal incision is made just proximal and lateral to the affected metacarpal head. A straight incision is strongly preferred over a curved or zig-zag incision to minimize the risk of creating ischemic skin flaps, particularly in the poorly vascularized dorsal skin of the hand. The incision is carried down through the subcutaneous tissue, where meticulous hemostasis is achieved using bipolar electrocautery. The dorsal sensory branches of the ulnar or radial nerve must be identified, gently mobilized, and protected with vessel loops to prevent painful postoperative neuromas.
Once the extensor hood is exposed, it is mobilized on one side of the metacarpal neck using a sharp surgical knife (e.g., a #15 blade). The approach can be trans-tendinous (splitting the EDC longitudinally) or tendon-sparing (retracting the EDC laterally or medially). Deep exposure involves dissecting the interosseous muscle from the lateral side of the metacarpal neck. The extensor tendon and its expansion are elevated from the dorsum of the metacarpal as necessary to achieve sufficient exposure of the malunion site. It is imperative to preserve the periosteum where possible, elevating it as a continuous sleeve, to aid in postoperative healing and provide a gliding layer for the extensor tendons.
Osteotomy Execution and Graft Harvesting
The method of osteotomy depends entirely on the maturity and density of the fracture callus. If the malunion is long-standing and the callus is sclerotic, the surgeon should use a fine drill bit (e.g., 1.5 mm or 2.0 mm) to create multiple transverse drill holes across the old fracture site. The osteotomy is then completed by connecting the drill holes with a sharp, narrow osteotome. This "postage-stamp" technique prevents uncontrolled propagation of the fracture into the articular surface of the metacarpal head. If the callus is relatively recent and soft, a sharp osteotome or an oscillating microsaw under continuous saline irrigation can be used to cut directly across the malunion site.
To provide intrinsic stability and restore length, an intramedullary cortical bone peg is utilized. The medullary canal is prepared by drilling both proximally (into the diaphysis) and distally (into the metacarpal head) so that it can accept the peg. The diameter of the drill should be slightly larger than a standard matchstick. Concurrently, a cortical bone peg is harvested from a donor site. The proximal ulna (olecranon) is an excellent source of dense cortical bone with minimal donor site morbidity. The peg must be meticulously shaped with a rongeur or high-speed burr to fit snugly into the prepared medullary canals.
Reduction, Fixation, and Soft Tissue Balancing
The fashioned cortical peg is inserted proximally into the medullary canal of the metacarpal shaft. The protruding portion of the peg is then capped with the distal fragment (the metacarpal head). Rotational alignment is the most critical aspect of the reduction. The surgeon must carefully check alignment by passively flexing the MCP and PIP joints to ensure the digit points toward the scaphoid tubercle, confirming the absence of malrotation and digital overlap. Once alignment is perfect, the fragments are impacted together over the peg. Supplemental cancellous bone chips (harvested from the same donor site) are packed around the osteotomy juncture to promote rapid osteogenesis.
Surgical Warning: If the osteotomy remains rotationally or angularly unstable despite the snug fit of the cortical bone peg, do not rely on the peg alone. Insert a supplemental oblique Kirschner wire (K-wire) across the osteotomy site to neutralize rotational forces. Alternatively, modern low-profile titanium locking plates can be applied dorsally to provide absolute stability, allowing for earlier mobilization.
A critical, often overlooked step in correcting long-standing metacarpal neck malunions is addressing the MCP joint contracture. Because the MCP joint collateral ligaments are eccentric (cam-shaped), they are lax in extension and tight in flexion. If the digit has been immobilized or held in extension due to the malunion, these ligaments will be severely contracted. When the collateral ligaments allow little or no motion after the osteotomy is fixed, a dorsal capsulotomy and collateral ligament release or recession are strictly indicated to restore the functional arc of motion. The lateral expansion of the extensor hood is then sutured back into its anatomical position using fine absorbable suture (e.g., 4-0 Monocryl or Vicryl), ensuring the EDC tendon is centralized over the metacarpal head before skin closure.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the correction of metacarpal neck malunions carries a distinct complication profile. The most frequent and functionally devastating complication is postoperative stiffness, particularly involving the extensor mechanism and the MCP joint. Extensor tendon adhesions occur due to the proximity of the hardware and the osteotomy site to the gliding paratenon. The incidence of clinically significant stiffness can approach 15-20% if early, controlled mobilization is not instituted. Pathophysiologically, the hematoma and surgical trauma stimulate a robust fibroblastic response, tethering the EDC to the underlying periosteum or hardware.
Nonunion or delayed union is another significant concern, particularly in cases where the osteotomy site was thermally necrosed by an aggressive saw blade without adequate irrigation, or where structural bone grafting was insufficient. The incidence of nonunion is generally low (<5%) when utilizing the intramedullary cortical peg technique, as it provides excellent biological compatibility and rigid internal splinting. However, if rigid plate fixation is used and the soft-tissue envelope is overly stripped, the risk of avascular necrosis of the metacarpal head or atrophic nonunion increases.
Hardware prominence and subsequent tenosynovitis are common when dorsal plates are utilized. The subcutaneous nature of the dorsal metacarpal means that even low-profile titanium plates can irritate the overlying extensor tendons, necessitating hardware removal in up to 30% of cases once clinical union is achieved. Furthermore, iatrogenic malrotation or recurrence of the deformity can occur if the fixation construct fails to neutralize the deforming forces of the intrinsic musculature during the early healing phase.
Salvage management for failed malunion corrections is highly complex. For severe, recalcitrant stiffness secondary to tendon adhesions, a secondary tenolysis and dorsal capsulotomy may be required, often performed under wide-awake local anesthesia no tourniquet (WALANT) to allow the patient to actively demonstrate tendon glide intraoperatively. In cases of infected nonunion or catastrophic failure of the metacarpal head, salvage options are limited to ray amputation (to restore overall hand function at the expense of a digit) or complex joint arthroplasty/arthrodesis.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Extensor Tendon Adhesions | 15 - 20% | Prolonged immobilization; prominent dorsal hardware; excessive periosteal stripping. | Aggressive hand therapy; secondary surgical tenolysis (WALANT preferred). |
| Hardware Prominence / Pain | 20 - 30% (Plates) | Thin dorsal soft tissue envelope; use of non-low-profile implants. | Elective hardware removal after radiographic union (minimum 4-6 months). |
| Recurrent Malunion / Malrotation | 5 - 10% | Inadequate initial fixation; failure to use supplemental K-wires with bone peg; early unprotected loading. | Revision osteotomy with rigid plate fixation and structural bone grafting. |
| Nonunion / Delayed Union | < 5% | Thermal necrosis from saw; inadequate bone graft; smoking; infection. | Debridement, autologous cancellous bone grafting, and revision rigid fixation. |
| Complex Regional Pain Syndrome | 2 - 5% | Excessive surgical trauma; poorly controlled postoperative pain; tight splinting. | Multidisciplinary pain management; stellate ganglion blocks; gentle active ROM. |


Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the final functional outcome as the surgical execution itself. The protocol is meticulously designed to protect the osteotomy and the delicate soft-tissue repairs while aggressively preventing stiffness in the interphalangeal and metacarpophalangeal joints. A close, collaborative relationship with a certified hand therapist (CHT) is mandatory. The balance between allowing early motion to prevent adhesions and providing sufficient stability to prevent construct failure requires constant clinical reassessment.
Phase 1: Protection and Controlled Edema (0 to 2 Weeks)
Immediately postoperatively, a bulky, non-compressive dressing and a custom dorsal blocking splint are applied. The splint must maintain the metacarpophalangeal (MCP) joints in 70 to 90 degrees of flexion. This "intrinsic-plus" or "safe" position is non-negotiable; it keeps the cam-shaped collateral ligaments on maximal stretch, preventing the devastating complication of MCP extension contracture. Crucially, the splint should be designed to allow for active and passive flexion and extension of the proximal and distal interphalangeal (PIP and DIP) joints. Patients are instructed to perform composite fist exercises within the confines of the splint to encourage flexor and extensor tendon glide, mitigating early adhesion formation. Strict elevation and active digit mobilization are emphasized to control postoperative edema.
Phase 2: Intermediate Motion and Splint Weaning (2 to 4 Weeks)
At the 2-week postoperative mark, the surgical dressings are removed, and the incision is inspected for primary healing. Sutures are removed if the wound is stable. The initial bulky splint is transitioned to a lighter, custom-molded thermoplastic hand-based splint. This new orthosis continues to prevent full, forceful extension of the MCP joint—thereby protecting the volar osteotomy gap and any dorsal hardware from excessive tension—but allows full, unrestricted active flexion and extension of the interphalangeal joints. Gentle active range of motion (AROM) of the MCP joint is initiated out of the splint under the direct supervision of the hand therapist. Passive range of motion (PROM) and aggressive stretching are strictly contraindicated at this stage to prevent displacing the osteotomy.
Phase 3: Strengthening and Functional Restoration (>4 Weeks)
As radiographic evidence of early callus formation becomes apparent (typically around 4 to 6 weeks), continuous splinting is discontinued. The patient is transitioned to a dynamic or static-progressive splinting regimen only if specific joint contractures are identified. Progressive strengthening exercises are initiated, starting with soft putty and advancing to grip strengthening devices. The focus shifts to restoring the functional arc of motion, maximizing power grip, and resolving any residual intrinsic muscle tightness. Patients are generally cleared to return to heavy manual labor or contact sports at 8 to 12 weeks, contingent upon complete radiographic consolidation of the osteotomy and the restoration of near-normal grip strength.



Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical decision-making for metacarpal neck malunions is deeply rooted in landmark biomechanical and clinical studies. Historically, intervention was guided primarily by radiographic appearance, leading to a high rate of unnecessary surgeries for cosmetic deformities that possessed no functional deficit. The paradigm shifted dramatically with the publication of foundational biomechanical studies evaluating the compensatory mechanics of the carpometacarpal (CMC) articulations.
Landmark literature by Ali et al. and Ford et al. definitively established the differential mobility of the CMC joints, proving that the 4th and 5th rays can dynamically compensate for up to 30 and 40 degrees of sagittal plane angulation, respectively. These studies demonstrated that grip strength and the functional arc of motion remain statistically unchanged within these tolerances, forming the basis of modern conservative management protocols. Consequently, the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) clinical guidelines strongly recommend non-operative management for isolated 5th metacarpal neck fractures angulated less than 40-50 degrees without malrotation.
Conversely, biomechanical analyses of the intrinsic musculature have elucidated the pathophysiology of pseudoclawing in malunions that exceed these compensatory thresholds. Studies utilizing cadaveric models have shown that for every 2 millimeters of metacarpal shortening or 10 degrees of uncompensated volar angulation, there is a measurable decrease in the mechanical advantage of the interosseous muscles, leading directly to extensor lag at the PIP joint and hyperextension at the MCP joint. This literature underscores the absolute necessity of restoring anatomical length during corrective osteotomy, validating the use of opening wedge techniques or the intramedullary cortical bone peg over traditional, shortening closing-wedge osteotomies.
Modern consensus emphasizes a highly individualized approach. The literature clearly supports that while angular deformity is well tolerated in the ulnar digits, rotational deformity is universally poorly tolerated across all rays. A malrotation of merely 5 degrees translates to significant digital overlap, necessitating immediate surgical correction. As fixation technologies have advanced—transitioning from simple K-wires to low-profile, variable-angle locking plates and precise intramedullary devices—the ability to achieve rigid fixation and
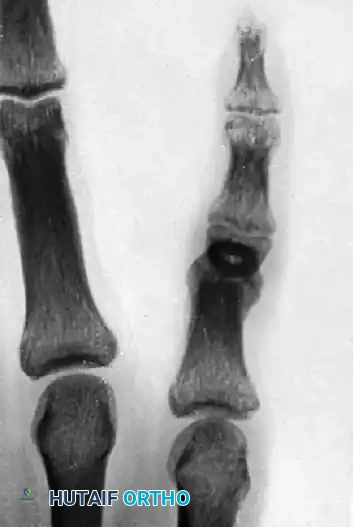
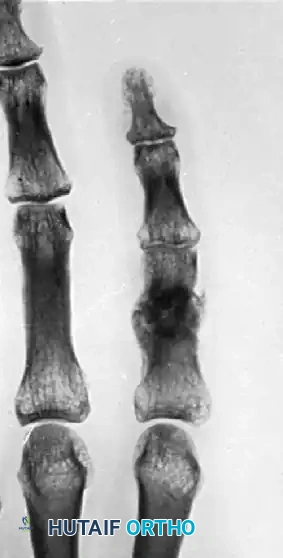
Clinical & Radiographic Imaging Archive



