Correction of Metacarpal Neck Malunion: Advanced Surgical Guide

Key Takeaway
Metacarpal neck malunions often result in aesthetic deformity, pseudoclawing, and diminished grip strength. Surgical correction is indicated when angulation exceeds acceptable biomechanical tolerances, particularly in the index and long fingers. This comprehensive guide details the dorsal approach, corrective osteotomy, and intramedullary cortical bone peg fixation techniques required to restore anatomical alignment, rotational stability, and optimal hand kinematics in the postgraduate orthopedic setting.
INTRODUCTION TO METACARPAL NECK MALUNION
Metacarpal neck fractures are among the most ubiquitous injuries in hand trauma, frequently presenting as the classic "boxer's fracture" of the fifth metacarpal. While the vast majority of these fractures are managed non-operatively with excellent functional outcomes, a subset will progress to symptomatic malunion. Metacarpal neck malunions are characterized by apex-dorsal angulation, volar displacement of the metacarpal head, shortening of the metacarpal ray, and potentially debilitating malrotation.
For the orthopedic surgeon, addressing a established metacarpal neck malunion requires a profound understanding of hand biomechanics. The functional deficit is rarely due to the bone deformity alone; rather, it is the secondary soft-tissue imbalances—specifically the alteration of the intrinsic muscle tension and the contracture of the metacarpophalangeal (MCP) joint collateral ligaments—that drive clinical symptoms.
Biomechanical Consequences of Malunion
When a metacarpal neck fracture heals with excessive volar angulation, the biomechanical cascade is predictable and often debilitating:
* Pseudoclawing: The volar displacement of the metacarpal head relatively lengthens the interosseous muscles, reducing their mechanical advantage. To compensate, the extensor digitorum communis (EDC) hyperextends the MCP joint, leading to secondary proximal interphalangeal (PIP) joint flexion.
* Loss of Knuckle Contour: The dorsal apex of the fracture becomes prominent, while the normal prominence of the metacarpal head is lost, leading to cosmetic dissatisfaction.
* Grip Strength Reduction: The altered vector of the flexor tendons and the shortened metacarpal lever arm can significantly diminish grip strength, particularly in power grip.
* Digital Overlap: Even minor degrees of malrotation (as little as 5 degrees) at the metacarpal level can result in 1.5 cm of digital overlap at the fingertips during composite flexion, severely impairing grasp.
Clinical Pearl: The tolerance for sagittal plane angulation varies significantly across the hand. The index and long fingers (2nd and 3rd metacarpals) are rigidly fixed at their carpometacarpal (CMC) joints and tolerate almost no angulation (maximum 10–15 degrees). Conversely, the ring and small fingers (4th and 5th metacarpals) possess 15 to 30 degrees of compensatory CMC mobility, allowing them to tolerate up to 40 to 50 degrees of angulation without severe functional deficit.
PREOPERATIVE EVALUATION AND INDICATIONS
Surgical correction is not indicated for cosmetic deformity alone. The primary indications for corrective osteotomy of a metacarpal neck malunion include:
1. Symptomatic pseudoclawing that interferes with hand function.
2. Painful grip due to a prominent volar metacarpal head in the palm.
3. Clinically significant malrotation causing digital overlap during composite flexion.
4. Angulation exceeding acceptable biomechanical tolerances (e.g., >15° in the index/long fingers, >50° in the small finger).
Preoperative radiographic assessment must include true posteroanterior (PA), lateral, and oblique views of the individual digit. The degree of angulation is measured using the medullary canal lines of the proximal shaft and the distal articular surface.
SURGICAL TECHNIQUE: CORRECTION OF METACARPAL NECK MALUNION
The following procedure details the classic corrective osteotomy utilizing an intramedullary cortical bone peg, a highly stable and biologically sound technique for restoring metacarpal length and alignment.
1. Patient Positioning and Preparation
The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded upper arm tourniquet is applied. Regional anesthesia (brachial plexus block) is preferred to allow for intraoperative assessment of the tenodesis effect, though general anesthesia is acceptable. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
2. Surgical Approach and Exposure
- Incision: Make a longitudinal dorsal incision just proximal and lateral to the affected metacarpal head. A straight incision is preferred over a curved one to minimize the risk of creating ischemic skin flaps.
- Soft Tissue Dissection: Carefully retract the dorsal sensory branches of the ulnar or radial nerve. Expose the extensor hood.
- Extensor Hood Mobilization: Free the extensor hood on one side of the metacarpal neck using a sharp surgical knife (e.g., a #15 blade).
- Deep Exposure: Dissect the interosseous muscle from the lateral side of the metacarpal neck. Elevate the extensor tendon and its expansion from the dorsum of the metacarpal as necessary to achieve sufficient exposure of the malunion site. Preserve the periosteum where possible to aid in postoperative healing.
3. Corrective Osteotomy
The method of osteotomy depends entirely on the maturity and density of the fracture callus.
* Hard/Mature Callus: If the malunion is long-standing and the callus is sclerotic, use a fine drill bit (e.g., 1.5 mm or 2.0 mm) to create multiple transverse drill holes across the old fracture site. Complete the osteotomy by connecting the drill holes with a sharp, narrow osteotome. This prevents uncontrolled propagation of the fracture into the metacarpal head.
* Soft/Immature Callus: If the callus is relatively recent and soft, a sharp osteotome or an oscillating microsaw under continuous saline irrigation can be used to cut directly across the malunion site.
4. Medullary Canal Preparation and Bone Peg Harvesting
To provide intrinsic stability and restore length, an intramedullary cortical bone peg is utilized.
* Canal Preparation: Drill the medullary canal both proximally (into the diaphysis) and distally (into the metacarpal head) so that it can accept a medullary cortical bone peg. The diameter of the drill should be slightly larger than a standard matchstick.
* Graft Harvest: Obtain a cortical bone peg from a donor site. The proximal ulna (olecranon) or the proximal tibia are excellent sources of dense cortical bone. The peg must be meticulously shaped with a rongeur or burr to fit snugly into the prepared medullary canals.
5. Reduction and Fixation
- Peg Insertion: Insert the fashioned cortical peg proximally into the medullary canal of the metacarpal shaft.
- Distal Capping: Cap the protruding portion of the peg with the distal fragment (the metacarpal head).
- Alignment Check: Carefully check rotational alignment. Flex the MCP and PIP joints to ensure the digit points toward the scaphoid tubercle, confirming the absence of malrotation. Once alignment is perfect, impact the fragments together over the peg.
- Supplemental Grafting: Pack cancellous bone chips (harvested from the same donor site) around the osteotomy juncture as needed to promote rapid osteogenesis.
Surgical Warning: If the osteotomy remains rotationally or angularly unstable despite the snug fit of the cortical bone peg, do not rely on the peg alone. Insert a supplemental oblique Kirschner wire (K-wire) across the osteotomy site to neutralize rotational forces.



FIGURE 67-72: Malunited fracture of the fifth metacarpal neck treated by open reduction and fixation with one Kirschner wire inserted obliquely. This is rarely necessary because the normal motion of the fifth carpometacarpal joint permits tolerance of up to 40 degrees of angulation at the fracture site.
6. Soft Tissue Balancing (Capsulotomy)
A critical, often overlooked step in correcting long-standing metacarpal neck malunions is addressing the MCP joint contracture.
* Examine the metacarpophalangeal joint for passive flexion.
* Because the MCP joint collateral ligaments are eccentric (cam-shaped), they are lax in extension and tight in flexion. If the digit has been immobilized or held in extension due to the malunion, these ligaments will be severely contracted.
* When the collateral ligaments allow little or no motion, a dorsal capsulotomy and collateral ligament release/recession are strictly indicated to restore the functional arc of motion.
7. Closure
- Suture the lateral expansion of the extensor hood back into its anatomical position using fine absorbable suture (e.g., 4-0 or 5-0 Monocryl or Vicryl). Ensure the EDC tendon is centralized over the metacarpal head.
- Close the skin with non-absorbable sutures.
- Apply a sterile dressing and a protective volar splint, holding the MCP joint in 60 to 70 degrees of flexion to keep the collateral ligaments on stretch.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol is designed to protect the osteotomy while preventing stiffness in the interphalangeal joints.
* Phase 1 (0 to 2 Weeks): A dorsal blocking splint is worn continuously. The splint must maintain the metacarpophalangeal (MCP) joints in 70 degrees of flexion. Crucially, the splint should allow for active and passive flexion of the proximal and distal interphalangeal (PIP and DIP) joints to prevent tendon adhesions.
* Phase 2 (2 to 4 Weeks): Sutures are removed at the 2-week mark. The initial splint is transitioned to a lighter, custom-molded thermoplastic splint. This new splint prevents full extension of the MCP joint (protecting the volar repair and dorsal hardware) but allows full, unrestricted flexion and extension of the interphalangeal joints. This lighter splint is worn for an additional 1 to 2 weeks.
* Phase 3 (>4 Weeks): Splinting is discontinued, and progressive strengthening and range-of-motion exercises are initiated under the guidance of a certified hand therapist.
MANAGEMENT OF PHALANGEAL MALUNIONS AND NONUNIONS
The principles of metacarpal neck correction can be extrapolated to the phalanges, though the anatomical constraints differ. Malunion of a metacarpal shaft or of a phalanx can also be treated with a medullary cortical bone peg; however, the peg must be shaped with extreme care to fit snugly within the narrower phalangeal medullary canal.
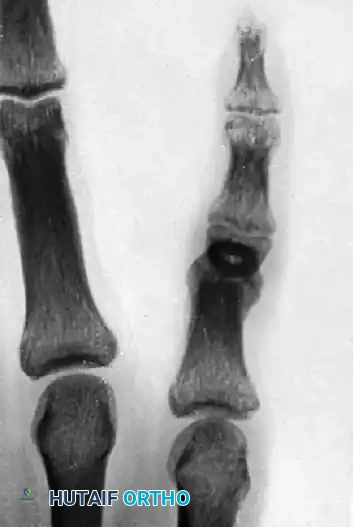



FIGURE 67-73: A, Malunited phalangeal fracture. B, Result is satisfactory after treatment by osteotomy and fixation with a medullary bone peg.
Rotational Deformities of the Proximal Phalanx
Malrotation of a proximal phalanx at any level is a severe functional impairment. When possible, rotational correction should be treated by an osteotomy at the base of the phalanx, regardless of where the original fracture occurred.
Surgical Pearl: The metaphyseal bone at the base of the phalanx heals rapidly and reliably. Furthermore, it is cut with significantly less difficulty than the hard, dense cortical bone found in the diaphyseal middle third of the phalanx.
Before completing the osteotomy, it is absolutely critical to make an orientation mark (using a surgical marker or a shallow saw score) on each side of the proposed osteotomy line. These reference points are used to precisely determine the amount of rotational change achieved during the procedure.
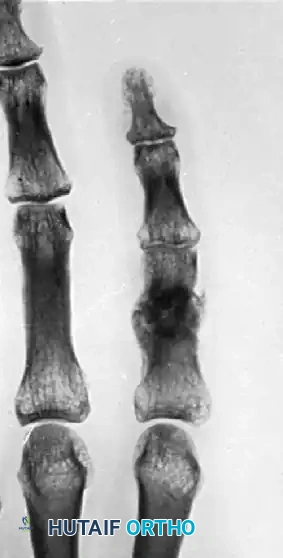

FIGURE 67-75: A, Malunited phalangeal fracture with rotational deformity. B, After treatment by osteotomy through the proximal end of the bone and fixation with two Kirschner wires. Healing is usually more rapid after osteotomy at this metaphyseal level than after one at the old diaphyseal fracture site.
Complex Intra-articular and Base Malunions
When malunions involve the articular surface, simple osteotomies may be insufficient. Splaying of the articular surface requires wedge resection and secure fixation.


FIGURE 67-70: A, Malunited fracture of the base of the middle phalanx with splaying of the volar and dorsal articular surfaces. B, After wedge resection of the bone, the volar and dorsal fragments were held securely with cerclage wire fixation.
In cases of severe joint destruction secondary to trauma, osteoarticular grafting may be required to salvage the digit and prevent the need for arthrodesis or amputation.







You Might Also Like

